PFO Slides - Drug Delivery Experts
advertisement

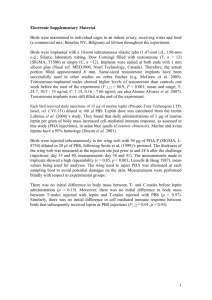
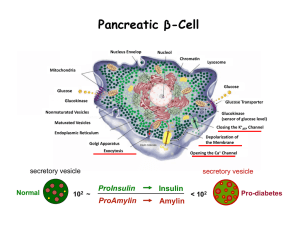
Revisiting the Therapeutic Potential of Leptin David Litzinger, PhD Director, Pharmaceutical Sciences Amylin Pharmaceuticals, Inc. 2011 AAPS National Biotechnology Conference San Francisco, CA Leptin History • 1950 Obese mice appear randomly in a colony at Jackson Laboratory. • 1994 Dr. Jeffrey Friedman and colleagues at Rockefeller University discover the ob gene and protein, and explore their role in body weight regulation, appetite, and metabolism. • 1997 Amgen begins clinical trials of leptin for obesity. • 1999 Amgen publishes disappointing obesity trial results. • 2007 Amylin conducts clinical POC test of leptin/pramlintide combination; reduces bodyweight on average by 12.7% over 24 weeks. • 2009 A 28-week pramlintide/leptin clinical study, followed by a 52-week extension study, showed sustained and robust weight-loss. • 2010 Amylin submits the initial sections of a rolling submission for a BLA for the use of leptin to treat patients with rare forms of lipodystrophy. • 2011 Amylin and JDRF announce that they entered into a research collaboration agreement to provide financial support for a clinical POC study to investigate leptin in patients with type 1 diabetes. 2 Multi-Hormonal Control of Body Weight Vagal afferents Hypothalamus GI tract Adipose tissue Ghrelin Hindbrain Leptin CCK PYY3-36 Insulin Amylin Resistin GLP-1 Visfatin OXM Adiponectin GIP PP Pancreatic Amylinislets Adapted from Badman M.K. and Flier J.S. Science 2005; 307: 1909-1914. Question: Why aren’t anti-obesity drugs more effective? 3 Pramlintide (25,28,29Pro-h-amylin) • 3949.4 Da, 37 amino acids • Isoelectric point 5.3 • Single disulfide bond, C-term amidated • No free cysteines • Limited solubility at neutral pH (<0.5 mg/mL), higher at lower pH 4 Pramlintide: Clinical Studies in Obesity Placebo (n = 17) Pramlintide 360 µg BID (n = 21) DoubleBlind Study D in Body Weight (%) 0 In obese patients, pramlintide elicits Single-Blind Extension Reduced food intake -2 -4 6.8% • • • • • Increased satiation and satiety Reduced 24-h intake (~500-750 kcal/d) Reduced fast food intake Reduced binge eating score (~45%) Effects independent of nausea -6 Sustained weight loss -8 -10 • With proportionate reduction in leptin Weight Loss 0 2 Weight Maintenance 4 6 8 Time (mo) 10 Data are for evaluable population; N = 38; Mean ± SE Smith SR, et al Diabetes Care. 2008; 31: 1816-1823 12 5 Metreleptin (r-metHuLeptin) • 16.2 kDa, 147 amino acids, (native leptin 146 AA) • Isoelectric point 6.1 • Single disulfide bond • No free cysteines • Limited solubility at neutral pH (2-3 mg/mL), higher at lower pH • Four helix bundle tertiary structure 6 Leptin Replacement Elicits Profound Weight Loss in Leptin-Deficient Mice and Humans ob/ob Mice Before After (Leptin Deficiency) (Leptin Replacement) Congenital Leptin Deficiency* Before After (Leptin Deficiency) (Leptin Replacement) Zhang,Y, et al. Nature. 1994;372:425–432 * Republished with permission of American Society for Clinical Investigation, from Farooqi IS, et al. J Clin Invest. 2002;110:1093–1103; permission conveyed through Copyright Clearance Center, Inc. 7 Leptin Does Not Cause Weight Loss in Dietinduced (Non-leptin deficient) Obesity DIO Rats Obese Humans Placebo BID (n = 25) Metreleptin 10 mg BID (n = 71) Vehicle Leptin 500 µg/kg per day 0 D Body Weight (kg) DBody Weight (%) (Vehicle Corrected) 2 -5 -10 1 0 -1 -2 -3 -4 -5 -15 0 1 2 Time (wk) 3 4 Dietary Lead-In -3 Randomized Treatment 0 3 6 9 Time (wk) Obese humans, mean ± SE; Continuous infusion of peptide at full doses (osmotic minipump) Roth et al., Obesity. 2006: 14(9 Suppl): A57-8. Abstract 177-P 12 8 Amylin+Leptin Synergy for Weight Loss is not Explained by the Anorexigenic Effect of Amylin 250 Food Intake % Change in Body Weight (Vehicle-Corrected) Cumulative Food Intake (grams) Vehicle Leptin 500 µg/kg/d Amylin 100 µg/kg/d (Pairfed-Amylin)+Leptin Amylin+Leptin 200 150 100 * 50 2 Body Weight 0 -2 -4 -6 -8 -10 * -12 -14 0 0 3 6 9 12 Time (Days) 0 3 6 9 12 Time (Days) *p<0.05 compared to all groups Diet-induced obesity prone rats (CRL; N=7/group). Roth JD, et al. Proc Natl Acad Sci USA. 2008;105:7257–7262. 9 Amylin/Leptin Induced Greater Fat Loss and Prevented Counter Regulatory Adaptations • Amylin + Leptin treated DIO rats lost nearly 2-fold greater fat mass than pair-fed control* Veh PF A+L Adipose Tissue (H&E) • Amylin + Leptin prevented metabolic counter-regulatory adaptations − No decrease in energy expenditure as was seen in pair-fed controls (oxygen consumption results) − Fat utilized throughout study whereas pair-fed controls initially showed fat followed by carbohydrate utilization (respiratory quotient results) *Pair-fed control: no leptin or amylin Trevaskis JL et al. Endocrinology. 2008; 149(11):5679-87 10 Plasma Pharmacology of Synergy: Requires Leptin Replacement, Pharmacological Amylin Plasma Leptin Plasma Amylin 600 25 500 Amylin (pM) 15 10 50 125 50 + 125 A+L 10 Leptin Vehicle 0 Amylin 5 Amylin Leptin (ng/mL) 20 400 300 200 100 0 Veh/Veh Amylin (10) Amylin (50) Diet induced obesity prone rats (CRL; N=5/group). Plasma leptin determined at Day 28 Selected doses (µg/kg/d) shown Trevaskis JL et al. Endocrinology. 2008; 149(11):5679-87 11 Amylin Upregulated pSTAT3 Signaling in the Ventromedial Hypothalamus in DIO Rats Vehicle Controls Leptin 15 mg/kg i.p. Ventromedial Hypothalamus pSTAT3-Activated Cells (n) 500 400 *, ** 300 Lean DIO–Vehicle DIO–PF DIO–Amylin 200 100 0 Lean Vehicle PF Amylin Leptin-Stimulated pSTAT3 Shown DIO Rats Lean Harlan Sprague Dawley rats or DIO-prone rats; Mean ± SE; *P<0.05 vs vehicle controls; **P<0.05 vs PF(amylin) Roth JD, et al. Proc Natl Acad Sci U S A. 2008;105:7257–7262 12 Pramlintide/Metreleptin: Phase 2 Clinical Proof-of-Concept Study – Design: Randomized, double-blind, controlled, multicenter – Study population: Overweight or obese subjects (BMI 27-35 kg/m2) – Treatment: 4-week lead-in requiring 2-8% weight loss followed by 20 weeks randomized treatment 2:2:1 pramlintide: pramlintide/metreleptin: metreleptin – Primary efficacy endpoint: Weight loss in pramlintide vs pramlintide/metreleptin 20% kcal deficit Pramlintide 360 µg BID Pramlintide 180 µg BID 40% kcal deficit Placebo-P + Metreleptin 5 mg BID Pramlintide 360 µg BID + Placebo-M Pramlintide 360 µg BID + Metreleptin 5 mg BID Lead-in Screen -4 -2 Randomized Treatment Day 1 1 4 8 12 16 20 Time (wk) Roth JD et al Proc Natl Acad Sci USA. 2008; 105: 7257-7262. 13 Amylin Agonism Restores Leptin Responsiveness in DIO Rats . . .and in Humans DIO Rats Obese and Overweight Humans 0 Mean (SE) % Change in Body Weight D Body Weight (%) (Vehicle Corrected) 0 -5 -10 -15 -20 0 1 2 3 4 Time (Week) Vehicle Leptin (250 µg/kg/d) Amylin (100 µg/kg/d Amylin + Leptin 5 6 -5 -10 -15 -4 0 4 8 12 16 20 Time (Week) Leptin (n=19) Pramlintide (n=38) Pramlintide + Leptin (n=36) 14 Lipodystrophy (LD) Pathophysiology Metabolic Abnormalities Often more severe than those associated with excess adiposity (i.e. obesity) • Severe insulin resistance / diabetes: • Often on 100’s-1000’s IU insulin/day • Rare set of syndromes characterized by loss of adipose tissue (primarily subcutaneous) - Inability to store fat in normal depots - Ectopic fat deposition (liver, muscle) Severe hypertriglyceridemia: • Often several 100’s-1000’s mg/dL • Increased risk of acute pancreatitis • Hepatic steatosis / steatohepatitis: • Hepatomegaly and elevated LFTs • Can lead to cirrhosis • Multiple other co-morbidities LFT, liver function test; Oral. Rev Endo Metab Disord 2003, 4:61-77. Chan et al. Endocr Pract 2010 ; 16:310-323. 15 Metreleptin Improved Hyperglycemia in Lipodystrophy Patients HbA1c 200 Mean (SE) FPG (mg/dL) Mean (SE) HbA1c (%) 10 9 8 7 6 5 0 54 4 8 Time (months) 40 41 Number of Patients 12 38 Fasting Plasma Glucose 180 160 140 120 100 80 0 55 4 8 Time (months) 40 43 Number of Patients 12 39 National Institutes of Health (NIH) open label study of metreleptin treatment, n=55 patients with metreleptin exposure ranging from 3 months to 9 years (Data on File, Amylin Pharmaceuticals, Inc.) 16 Metreleptin Improved Hypertriglyceridemia in Lipodystrophy Patients Mean Triglycerides Median Triglycerides 500 Median Triglycerides (mg/dL) Mean (SE) Triglycerides (mg/dL) 1750 1500 1250 1000 750 500 250 400 300 200 100 0 0 0 54 4 8 Time (months) 40 42 Number of Patients 12 39 0 4 8 Time (months) 12 54 40 42 Number of Patients 39 National Institutes of Health (NIH) open label study of metreleptin treatment, n=55 patients with metreleptin exposure ranging from 3 months to 9 years (Data on File, Amylin Pharmaceuticals, Inc.) 17 Effect of Metreleptin on Lipodystrophy • Unique therapy that directly addresses underlying pathophysiology • Corrects relative leptin deficiency and associated hyperphagia, which exacerbates metabolic abnormalities as patients are driven to consume more • Stimulates breakdown of fat in liver and muscle and reduces high triglyceride levels • Improves insulin sensitivity and reduces hyperglycemia Oral et al. Endocr Pract 2010; 16:324-333. 18 Glycemic Volatility of Insulin Monotherapy: Why? 700 Insulin Dose 0.2 U b.i.d. 600 500 mg/dl 400 300 200 100 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Days 19 Normal Roles of Endogenous Insulin: Paracrine (Local) and Endocrine (Systemic) GLUCAGON Paracrine (Local) a b INSULIN PERIPHERAL GLUCOSE UPTAKE + Endocrine (Systemic) GLYCOGENOLYSIS GLUCONEOGENESIS KETOGENESIS Fuels 20 STRATEGY: Since injected insulin cannot approach paracrine levels in normal islets a-cells, let leptin suppress glucagon. GLUCAGON a X b + INSULIN X PERIPHERAL GLUCOSE UPTAKE GLYCOGENOLYSIS GLUCONEOGENESIS KETOGENESIS Fuels 21 Glycemic Volatility of Insulin Monotherapy is Eliminated by Leptin 700 Insulin Dose 0.2 U b.i.d. 600 500 mg/dl 400 300 200 100 0 Leptin + Low Dose Insulin (0.02 U b.i.d.) 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Days 22 Adenoviral Leptin Normalizes Hyperglucagonemia in Insulin-deficient T1DM Rodents L Plasma Glucagon p<0.01 800 pg/mL 600 400 200 0 Nondiabetic N=4 Untreated diabetic N=4 Ad Leptin diabetic N=5 23 Product Development Product Presentation/Patient Compliance • Co-Formulation − Both API’s in single formulation for administration • Sustained-Release Formulations − Extend duration of release from injection site − Extend duration of activity, reduce injection frequency • Second Generation Compounds − Reduce clearance and extend circulation − Extended duration of activity, reduce injection frequency − Improve pharmaceutical properties • Other − Devices 24 Summary • Weight loss with leptin can be restored by amylin/pram – a potential drug for obesity • Leptin markedly improves the metabolic pathology of LD - a potential drug for LD • Leptin normalizes diabetes in preclinical models - a potential drug for Type 1 diabetes • SR formulations, Second Generation molecules, and devices in development for optimal product presentation and patient compliance 25 Acknowledgements • In Vivo Pharmacology – – – – – – – – – • Jonathan Roth James Trevaskis Victoria Turek Christine Mack Carrie Wittmer Chunli Lei Calvin Vu Pete Griffin David Parkes • – – – – – • • Research Alain Baron Christian Weyer Joy Koda Amy Halseth Larry Shen Biometrics – Todd Coffey – Colleen Burns • R&D Strategic Relations – Elaine Chiquette Functional Imaging – Barbara Roland – Rebecca Cole – Guibao Gu Clinical Research • Collaborators – Barry Levin • Roger Unger and Group – Soumitra Ghosh 26