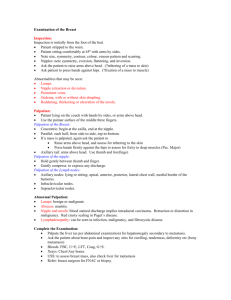
ASSESSING THE BREAST
advertisement

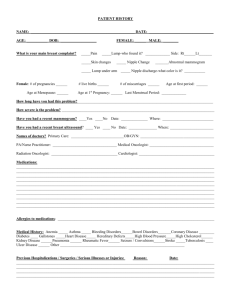
ASSESSING THE BREASTS NUR211 Kathleen Hancock Assessing the Breasts Obtain a breast history. Perform a breast physical assessment. Document breast assessment findings. Differentiate between normal and abnormal findings. Breast Composition 3 types of tissue: *Glandular *Fibrous *Adipose Structures Lobes and lobules Lactiferous ducts and sinuses Areola Montgomery’s glands Structures Nipple Cooper’s ligament Pectoralis major and serratus anterior muscles Functions What are the functions of… Lobes & lobules: Contain alveoli cells that produce milk Lactiferous ducts & sinuses: Carry and store milk Areola: Dark tissue surrounding nipple (Continued) Functions What are the functions of… Montgomery’s glands: Sebaceous gland Nipple: Nursing and sexual stimulation Cooper’s Ligament: Ligament attached to chest wall muscles that supports breasts (Continued) Functions What are the functions of… Pectoralis major & serratus anterior muscles: Breast overlies these muscles Lymph nodes: Drain breast, chest, and arms Breast Health: Cancer Prevention Self Breast Exam (SBE) Every month Mammogram After age 40 every year More frequent if personal or family history Breast Exam by nurse or doctor every year Developmental Variations What developmental breast variations might be seen with: Children Pregnant clients Older adults History What can the history tell you about the breast? Biographical data Current health status Past health history Family history Review of systems Psychosocial history Symptoms What symptoms signal a problem with the breasts? Breast lump or mass Pain or tenderness Nipple discharge Physical Assessment Anatomical landmarks: quadrants of the breast, include Tail of Spence (Continued) Inspection Breasts: size, shape, symmetry, color, lesions, venous pattern, dimpling, or retraction Nipple and areola: nipple position and direction; discharge Axillae: color, lesions, rashes Physical Exam Inspection Position: sitting, hands on hips, hands over head, leaning forward Tools: small pillow or towel, ruler, gloves, slide, and culture slide. Sitting, arms at sides Arms overhead Arms pressing on hips Leaning forward Palpation Lymph nodes: axillary, clavicular while sitting Breasts: consistency, masses, tenderness in supine position Nipple: elasticity, masses, tenderness, discharge Supraclavicular Nodes Infraclavicular Nodes Axillary Nodes Palpation –Vertical Strip Method Preferred Approach: supine with pillow or towel under shoulder Pattern (vertical, wedge, or circular) light, medium, and deep Supine with shoulder support –Use pads of fingers of dominant hand Strip Method of Palpation Cover all of breast Use 3 middle finger pads, not tips Use sliding motion Overlapping dime size circles 3 pressure levels: light, medium, deep Include nipple and areola Large Breasts Bimanual palpation to adequately examine all areas Often have an inframammary ridge Male Breast Inspection Palpation Lymph nodes while sitting Breast while sitting or if large while lying down Male Breast Enlargement: Gynecomastia Characteristics of Masses Note: Location Size Mobility Temperature Shape/Borders Tenderness Consistency Redness Example: Pertinent Physical Findings Right breast larger than left No dimpling, retraction Small, pea size (0.5cm), movable, rubbery, smooth-edged lesion in right breast at 2 o’clock in RUQ No palpable nodes