Chấn thương thanh quản có thể được điều trị nội khoa hoặc ngoại
advertisement

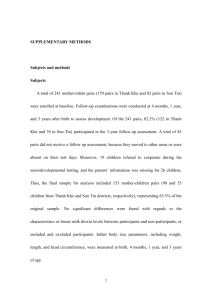
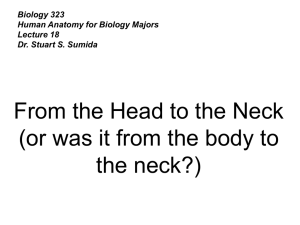
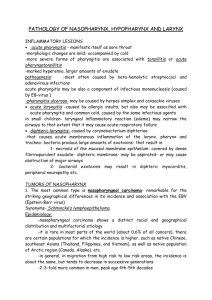
TITLE: Chấn thương thanh quản SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: September 02, 2003 RESIDENT PHYSICIAN: Michael Underbrink, MD FACULTY PHYSICIAN: Anna Pou, MD SERIES EDITORS: Francis B. Quinn, Jr., MD and Matthew W. Ryan, MD Dịch: BSNT ĐINH TẤT THẮNG "This material was prepared by resident physicians in partial fulfillment of educational requirements established for the Postgraduate Training Program of the UTMB Department of Otolaryngology/Head and Neck Surgery and was not intended for clinical use in its present form. It was prepared for the purpose of stimulating group discussion in a conference setting. No warranties, either express or implied, are made with respect to its accuracy, completeness, or timeliness. The material does not necessarily reflect the current or past opinions of members of the UTMB faculty and should not be used for purposes of diagnosis or treatment without consulting appropriate literature sources and informed professional opinion." Giới thiệu Chấn thương ngoài thanh quản là chấn thương ít gặp có tỷ lệ xấp xỉ 1/30,000 trong các trường hợp cấp cứu. Đây có thể là điều may mắn vì chấn thương thanh quản có thể dẫn tới những vấn đề nghiêm trọng về hô hấp và ảnh hưởng đến giọng nói nếu không được chẩn đoán nhanh chóng. Xử trí ban đầu với một chấn thương thanh quản cấp là đảm bảo đường thở. Chức năng nói, có thể được ưu tiên quan trọng thứ 2. Vì thế,thúc bách bác sỹ Tai Mũi Họng biết tới chẩn đoán và điều trị với những trường hợp hiếm nhưng là loại chấn thương nghiêm trọng này. Giải phẫu và sinh lý May mắn là thanh quản được bảo vệ tốt bởi xương hàm dưới, xương ức và sự linh hoạt của cổ. Chức năng đầu tiên của thanh quản là tạo nên một đường khí, bảo vệ đường hô hấp dưới, và là cơ quan phát âm. Thanh quản có thể được chia thành 3 vùng: thượng thanh môn, thanh môn và hạ thanh môn. Nâng đỡ bởi xương móng, sụn giáp và sụn nhẫn. Thượng thanh môn ít được nâng đỡ hơn tùy thuộc vào việc nâng đỡ bên ngoài và gồm nhiều tổ chức mô mềm và niêm mạc thừa Thanh môn tựa chặt vào sự nâng đỡ bên ngoài và sự phối hợp linh hoạt của sụn nhẫn phễu và hoạt động thần kinh cơ để hỗ trợ hô hấp và tạo âm. Ở người lớn, thanh môn là chỗ hẹp nhất của khí đạo. Vì thế, tổn thương ở vị trí này có thể làm ảnh hưởng hô hấp nghiêm trọng. Hạ thanh môn được hỗ trợ bởi chỉ bởi sụn nhẫn, chỗ mà ở sơ sinh và trẻ nhỏ khí đạo hẹp nhất. Cơ chế chấn thương Loại chấn thương có thể được chia thành vết thương đụng giập hoặc xuyên thủng. Vết thương đụng giập thường gặp hơn do tai nạn giao thông. Hộp thanh quản bị dồn nén giữa những những vật bên ngoài (ví dụ,tay lái ô tô hoặc tấm gương chắn trước xe) và mặt trước của cột sống cổ. Cánh sụn giáp bè ra và với một lực đủ mạnh, có thể vỡ sụn thường theo chiều đứng giữa hoặc cạnh giữa tự nhiên. Các loại khác của vết thương chột như do chấn thương thể thao,hành hung cưỡng hiếp, hoặc vướng dây treo quần áo hay các nguyên nhân về tai nạn xe cộ. Lực chấn thương có theery làm thương tổn mô mề và/hoặc mất liên tục sụn với các dấu hiệu chấn thương ở bên ngoài.Vết thương chột cũng có thể gây nên trật khớp nhẫn phễu hoặc tổn thương dây thần kinh quặt ngược làm hạn chế sự di động của dây thanh. Vết thương xuyên thủng thanh quản có thể xảy ra thứ phát do dao đâm hoặc đạn bắn. Phạm vi tổn thương thay đổi theo loại vũ khí tác động, và quan trọng là phát hiện các thương tổn phối hợp, ví dụ như thần kinh, mạch máu, hoặc thực quản, là những tình trạng thường gặp. Đánh giá ban đầu Xử trí ban đầu nên theo nguyên tắc ATLS. Đảm bảo một đường thở được ưu tiên 1. Chấn thương cột sống cổ nên được nghĩ tới cho tới khi có bằng chứng chính xác. Có một số bàn luận về việc xử trí đường thở ở những bệnh nhân này, nhưng hầu hết các tác giả khuyến cáo mở khí quản dưới gây tê tại chỗ đối với những bệnh nhân suy hô hấp.Việc cố gắng đặt nội khí quản qua đường mũi và qua đường miệng ở những bệnh nhân này có thể dẫn tới những tổn thương nặng hơn cho khí đạo vốn dĩ đã nhỏ/yếu. Thủ thuật mở sụn nhẫn giáp nên tránh trong quy trình xử trí chấn thương thanh quản vì điều này có thể làm tổn thương nặng hơn.Sự cân nhắc cần kỹ lưỡng ở những bệnh nhân nhi. Do kích thước nhỏ hơn của khí đạo trẻ nhỏ và nguy cơ sưng nề mô mềm kèm theo trong chấn thương thanh quản, người ta khuyến cao rằng cần thực hiện mở khí quản nhờ nội soi khí quản ở phòng mổ. Ở những bệnh nhân không có những rối loạn đường thở cấp, cần phải thăm khám thực thể và hỏi tiền sử bệnh nhân cẩn thận. Các triệu chứng của chấn thương thanh quản có thể bao gồm thay đổi giọng, đau, nuốt khó, nuốt đau, ho ra máu và/hoặc stridor (tiếng thở rít). Khi ngửa cổ không chịu được do các triệu chứng của chấn thương thanh quản liên quan với những ảnh hưởng khí đạo. Schaefer báo cáo triệu chứng tương quan với hầu hết các thương tổn nặng là suy hô hấp. Fuhrman, et al., báo cáo triệu chứng xác thực nhất là khàn giọng. Các dấu hiệu kinh điển của chấn thương ngoại thanh quản bao gồm khàn tiếng,tràn khí và khái huyết.Triệu chứng xác thực nhất theo báo cáo Fuhrman là nhạy cảm đau và tràn khí dưới da. Các dấu chứng thực thể khác, như là cổ trước thâm tím và lệch khí quản. Các thương tổn phối hợp bao gồm cột sống cổ, thực quản và thương tổn mạch máu phải được nghĩ tới và đánh giá. Ở những bệnh nhân bất động, nội soi mềm thanh quản ở phòng cấp cứu nên được chỉ định. CT scan, soi thanh quản trực tiếp, soi khí quản và thực quản được sử dụng để lượng giá dựa trên những dấu hiệu trên nội soi mềm ban đầu. Trong việc phân loại bệnh nhân có chấn thương thanh quản việc thăm khám nội soi mềm và những hình ảnh trên CT ngày càng quan trọng hơn để hỗ trợ xử trí các thương tổn. Một số sơ đồ điều trị được đưa ra chia thành 4 nhóm bởi Schaefer và Close và Fuhrman et al đã chia thành 5 nhóm là nhóm tách rời nhẫn khí quản. Phân loại các tổn thương thanh quản Nhóm I các tổn thương gồm có tụ máu nhẹ ở nội thanh quản, phù nề hoặc rách không tìm thấy chỗ vỡ. Nhóm II là các tổn thương phù nề, tụ máu,rách nhẹ niêm mạc mà không ảnh hưởng sụn không thấy tổn thương vỡ trên CT scan. và Khối phù nề, rách niêm mạc, chỗ vỡ bị thế chỗ, lộ sụn và/hoặc cố định dây thanh bất được xếp vào nhóm thứ III. Nhóm IV tổn thương tương tự như nhóm II kèm theo hai đường vỡ hoặc nhiều hơn, khung thanh quản không vững hoặc có biểu hiện chấn thương mép trước. Nhóm V là sự tách rời hoàn toàn thanh khí quản. Hình ảnh X quang Ở những bệnh nhân bất động, sau khi xử trí đường thở, chụp CT scan thanh quản có thể được chỉ định. CT không cần thiết ở bệnh nhân không có các triệu chứng đưa đến chỉ định phẫu thuật, ví dụ như đang chảy máu, khái huyết, cần thiết cho xử trí cấp cứu đường thở, lộ sụn và xé rách nhiều trên nội soi thanh quản, hoặc có phì phò qua miệng vết thương. Ngược lại ở những bệnh nhân có thương tổn tối thiểu và thăm khám thông thường hầu như không có giá trị bằng phim CT scan vùng cổ. Ở những bệnh nhân chấn thương thanh quản nặng và những thăm khám cận lâm sàng thì CTscan đóng vai trò khách quan và là nền tảng nên được chỉ định. Điều đáng chú ý là một số tác giả chỉ định CT ngay ở những bệnh nhân chấn thương nặng trước khi xử trí tại phòng mổ như là một “bản đồ chỉ đường (road map)” đối với những bệnh nhân bị chấn thương. Toàn bộ cột sống cổ nên được đánh giá qua điện quang. Chụp mạch và thực quản có thuốc có thể được chỉ định trong một số trường hợp chọn lọc, đặc biệt ở những vùng chấn thương xuyên thủng sâu. Xử trí không phẫu thuật Chấn thương thanh quản có thể được điều trị nội khoa hoặc ngoại khoa tùy thuộc vào nội soi thanh quản ban đầu và những hình ảnh trên CT scan. Bệnh nhân có thể được điều trị nội khoa và theo dõi sát nếu tổn thương se được giải quyết mà không can thiệp phẫu thuật và khí đạo ổn định. Nhóm I có thể xử trí một cách an toàn với thời gian theo dõi sát tối thiểu là 24h, nằm đầu cao, nhịn nói và thở qua không khí được làm ấm, ẩm. Kháng sinh được khuyến cáo đối với tổn thương niêm mạc thanh quản. Điều trị thuốc chống trào ngược cũng được chỉ định ban đầu. Mặc dù không có bằng chứng, sử dụng corticoid toàn thân thường đem lại hiệu quả trong việc làm giảm phù nề . Ăn qua xông dạ dày qua đường mũi nên được cân nhắc nếu có rách niêm mạc nhiều. Việc thăm khám nội soi mềm theo trình tự nên được thực hiện để đánh giá đường thở và sự lành thương để xuất viện. Điều trị phẫu thuật Điều trị phẫu thuật có thuật có thể từ thấp đến cao từ việc thiết lập đường thở tới việc mở rộng giải quyết chỗ vỡ của khung thanh quản. Các vết thương xuyên thủng cần được mở ra để thăm dò hơn là vết thương chột.Ở những bệnh nhân nhóm II tới nhóm V đòi hỏi một vài hình thức can thiệp phẫu thuật. Các lựa chọn phẫu thuật được chia thành 1 trong 3 loại sau: nội soi đơn thuần, nội soi kèm theo mổ thăm dò, và nội soi mổ thăm dò và đặt stent thanh quản.Nếu có bất cứ nghi ngờ về sự lan rộng của tổn thương nội soi nên được thực hiện. Các chỉ định để phẫu thuật thăm dò bao gồm: xé rách rộng niêm mạc, lộ sụn, nhiều chỗ vỡ và thế chỗ sụn vỡ, bất động dây thanh, vỡ sụn nhẫn, trật khớp nhẫn phễu, và xé rách cả bờ tự do dây thanh hoặc mép trước. Đường vỡ theo hướng đứng giữa hoặc cạnh giữa cánh sụn giáp có thể đi vào trong khung thanh quản và thường đòi hỏi ORIF. Mở khí quản nên được thực hiện ở những bệnh nhân có tổn thương lan rộng và nên được rạch xuống thấp hơn bình thường (sụn 4,5) theo đường dọc( tốt hơn ở những trường hợp có tách rời thanh khí quản. Khi chỉ định mở thanh quản kiểm tra, cần phải thực hiện trong vòng 24h của chấn thương để đem lại kết quả tối ưu cho chức năng thở và phát âm. Một đường rạch da ngang ở mức màng nhẫn giáp và bóc tách vạt cơ bám da cổ. Bộc lộ các cơ băng và khung thanh quản sau đó theo đường giữa. Thanh quản có thể được kiểm tra qua việc mở sụn giáp ở đường giữa hoặc theo đường vỡ thẳng đứng phía trong 2-3mm của đường giữa.Cánh sụn giáp được vén ra ngoài để thấy được nội thanh quản. Tất cả các sụn được bộc lộ và các mô dưới niêm mạc được che phủ sau đó bằng niêm mạc từ sau ra trước.Khâu kín ban đầu là luôn luôn có thể và mở ổ dẫn lưu tối thiểu. Đóng vết thương bằng chỉ tiêu với mũi khâu bên ngoài lòng thanh quản để tránh sự lên mô hạt. Sụn phễu bị trật nên được nắn lại.Mép trước nên được khâu lại bằng chỉ 4.0 để treo phía trước của dây thanh thật vào phía ngoài màng sụn giáp. Mở sụn giáp có thể sau đó có thể được cố định lại bằng chỉ không tiêu, dây thép hoặc nẹp cứng nhỏ. Các sụn vỡ được nắn lại và có thể làm cho vững bằng cách sử dụng các vật liệu khác nhau, như dây thép, chỉ không tiêu, và nẹp nhỏ. Nếu vỡ vụn, các mảnh nhỏ của sụn không còn màng sụn nguyên vẹn được lấy bỏ để tránh viêm sụn. Sự thích nghi với nẹp nhỏ về mặt lý thuyết có chỗ thuận lợi trong việc cố định trực tiếp thanh quản (ít cần thiết đối với việc sử dụng ống nong nội thanh quản), khả năng tạo cầu với những khoảng hỗng lớn ( gãy vụn), và phục hình lại khung thanh quản. Sử dụng nong nội thanh quản để bảo tồn đối với các tổn thương gồm rách mép trước, khối thương tổn niêm mạc và vỡ vụn thanh quản. Stent giúp tái lập lại hình thuyền của mép trước, làm vững những vỡ vụn nghiêm trọng và tránh tạo mảng và sẹo hẹp. Các dạng stent khác nhau có thể được sử dụng như ống nội khí quản Portex được thu ngắn lại, tạo thành một ống nong đàn hồi, hoặc tạo một võng hình ngón tay lấp đầy bởi spongel. Ống nong nên đặt từ chỗ nếp tiền đình tới sụn khí quản thứ nhất và làm cho vừa với hình dạng của nội thanh quản. Ống nong nên được làm cho vững bên trong thanh quản và cho phép thanh quản di động trong khi nuốt. Mũi khâu sâu bằng chỉ không tiêu được đưa qua stent và thanh quản ở thanh thất và một chỗ khác ở màng nhẫn giáp và tạo một nút ra ngoài qua da. Ống nong không nên để lâu quá 2-3 tuần. Lấy ống nên thực hiện dưới gây mê toàn thân với sự hỗ trợ của nội soi và các phẫu thuật them để lấy bỏ các mô hạt nếu thấy cần thiết. Tổn thương đơn độc tách rời thanh khí quản thường dẫn tới chết ngay lập tức. Thỉnh thoảng khí đạo có thể được duy trì được ổn định với tình trạng lớp niêm mạc còn nguyên vẹn. Mặc dù việc cố gắng đặt nội khí quản thành công với nội soi phế quản đã được báo cáo, cách xử trí an toàn và thường làm hơn vẫn là khai khí quản. Tổn thương dây quặt ngược hai bên và sẹo hẹp hạ thanh môn thường gặp ở bệnh cảnh chấn thương này.Phẫu thuật sữa chữa đòi hỏi những mũi khâu cố định chắc giữa sụn nhẫn và vòng sụn khí quản thứ hai để nâng đỡ cho khí đạo. Điều này có thể gặp khó khăn nếu vỡ sụn nhẫn đi kèm sau khi cố định phía trong Các thương tổn nặng và rộng ở mô mềm và làm mất liên tục ở thượng thanh môn hoặc nửa thanh quản có thể được xử trí bằng các phẫu thuật cắt nửa thanh quản để phục hồi chức năng. Cắt thanh quản toàn phần là phương án cuối cùng và được chỉ định đối với các tình huống nơi mà những yếu tố cơ bản của khung thanh quản và mô mềm không còn giá trị sử dụng để phục hồi lại. Kết quả Chất lượng cuối cùng của đường thở, giọng nói và chức năng nuốt là những điều quan trọng sau khi phẫu thuật sữa chữa đối với chấn thương ngoại thanh quản. TÌnh trạng khí đạo xấu nếu bệnh nhân vẫn duy trì việc thở qua canuyn, vừa nếu thở vào nhẹ hoặc không thích ứng khi tập thở, tốt nếu tình trạng hô hấp như trước khi bị chấn thương. GIọng nói có thể coi như là xấu nếu còn mất tiếng và chỉ thì thầm, vừa nếu chức năng có thay đổi ( khàn giọng cải thiện), và tốt nếu bình thường. Chức năng nuốt một là bình thường hoặc không bình thường theo nhận định chủ quan của bệnh nhân.Nói chung,xử trí chấn thương một cách dè dặt tốt hơn là phẫu thuật lớn do các tổn thương nặng nề lúc đầu. Việc sử dụng stent nội thanh quản là khuynh hướng làm cải thiện giọng mà không ảnh hưởng chung đến tình trạng của khí đạo. Thời gian lấy stent cũng ít hơn, và kết quả cũng khả quan hơn. Liệt dây thanh tác động đến cả hai chức năng thở và nói. Các kết quả cải thiện cũng cho thấy sớm hơn đối với thời gian được sữa chữa ( dưới 48h từ lúc bắt đầu bị tổn thương.) Kết luận Chấn thương ngoại thanh quản là một chấn thương ít gặp trong khi cần xử trí một cách hệ thống. Việc nhận định sớm là quan trọng đối với việc cứu sống bệnh nhân cũng như đảm bảo đường thở tốt và chức năng phát âm. Các triệu chứng chính là khàn tiếng, tràn khí dưới da, và đau với một tiền sử chấn thương nên nghĩ tới một sự lượng giá đúng lúc về thanh quản và hỗ trợ đường thở. Nội soi mềm thanh quản theo sau bởi CTscan và phẫu thuật cho thấy rằng cần thiết như là một tiêu chuẩn trong xử trí ban đầu. Các tổn thương phối hợp như cột sống cổ, mạch máu và các tổn thương thực quản nên được kiểm tra. ĐIều trị có thể nội khoa hoặc ngoại khoa (có hoặc không đặt stent) dựa vào vị trí và độ lan rộng của tổn thương. Tài liệu tham khảo O’Mara, W and Hebert, F. External laryngeal trauma. J La State Med Soc. Vol 152(5): 218222. May 2000. Jewett, B.S., Shockley, W.W., Rutledge, R. External laryngeal trauma analysis of 392 patients. Arch Oto HNS. Volume 125(8): 877-880. August 1999. Pou, A.M., Shoemaker, D.L., Carrau, R.L., Snyderman, C.H., Eibling, D.E. Repair of laryngeal fractures using adaptation plates. Head & Neck. Vol. 20: 707-713. December 1998. Offiah, C.J., Endres, D. Isolated laryngotracheal separation following blunt trauma to the neck. J Laryng Oto. Vol. 111: 1079-1081. November 1997. Beasley, D.J. and Miller, R.H. Acute laryngeal trauma. J La State Med Soc. Vol 148(4):143145. April 1996. Carrau, R.L. and Myers, E. Contemporary management of laryngeal trauma. University of Pittsburgh Medical Center: Trauma Rounds. Vol. 5(3):1-5. June 1994. Yen, P.T., Lee, H.Y., Tsai, M.H., Chan, S.T., and Huang T.S. Clinical analysis of external laryngeal trauma. J Laryng Oto. Vol. 108:221-225. March 1994. Bent, J.P. and Porubsky, E.S. The management of blunt fractures of the thyroid cartilage. Oto HNS. Vol. 110:195-202. 1994. Stack, B.C. and Ridley, M.B. Arytenoid subluxation from blunt laryngeal trauma. Amer J Otolaryng. Vol 15(1): 68-73. Jan-Feb 1994. Bent, J.P., Silver, J.R., and Porubsky, E.S. Acute laryngeal trauma: a review of 77 patients. Oto HNS. Vol 109:441-449. 1993. Schaefer, S.D. Use of CT Scanning in the management of the acutely injured larynx. Otolaryng Clinics NA. Vol 24(1): 31-36. February 1991. Schaefer, S.D. The treatment of acute external laryngeal injuries. Arch Otolaryng HNS. Vol 117: 35-39. January 1991. Fuhrman, G.M., Stieg, F.H., and Buerk, C.A. Blunt laryngeal trauma: Classification and management protocol. J Trauma. Vol 30(1): 87-92. January 1990. Gussack, G.S., Jurkovich, G.J. and Luterman, A. Laryngotracheal trauma: A protocol approach to a rare injury. Laryngoscope. Vol 96: 660-665. 1986. Schaefer, S.D. Primary management of laryngeal trauma. Ann Oto Rhino Laryng. Vol 91:399402. 1982. Leopold, D.A. Laryngeal Trauma. Arch Otolaryng. Vol 109: 106-111. February 1983. Laryngeal Fractures Author: Samir S Pancholi, DO, Consulting Surgeon, Cosmetic Surgery of Las Vegas; Adjunct Assistant Professor of Cosmetic Surgery, Touro University; Assistant Professor of Otolaryngology-Facial Plastic Surgery, Michigan State University Coauthor(s): Wayne K Robbins, DO, FAOCO, Program Director, Department of Otolaryngology-Facial Plastic Surgery, Genesys Regional Medical Center, Michigan State University; Alpesh Desai, DO, Assistant Professor, Department of Dermatology, Western University of Health Sciences; Tejas Desai, DO, Staff Physician, Department of Dermatology, Western University of Health Sciences Contributor Information and Disclosures Updated: Jan 9, 2009 Print This Email This Overview Workup Treatment Follow-up Multimedia References Keywords Introduction A laryngeal fracture can occur following direct trauma to the neck region and may lead to lifethreatening airway obstruction. For this reason, a patient suspected of having a fractured larynx should be treated in an emergent manner. Problem A traumatically injured patient may present with many distracting injuries. Appropriate treatment of this patient requires that airway patency be the first priority. Injury to the larynx may range from simple mucosal tears to fractured and comminuted cartilage. Any combination of injuries along this continuum can result in a precipitous airway emergency. Although advancements in imaging techniques have improved their diagnosis, the rarity of laryngeal fractures and the limited experience of otolaryngologists have made this a challenging entity to manage. An organized approach to laryngeal fractures can prevent misdiagnosis and inadequate management. Frequency A laryngeal fracture is a rare condition, occurring in approximately 1 per 137,000 inpatient visits,1 1 patient per 14,000-42,000 emergency department visits,2 and less than 1% of all blunt traumas.3 The rarity of this condition is likely due to the protected location of the larynx, with the rigid cervical spine posterior and the mandible hanging in a superior and anterior position. This protection is amplified in the pediatric population, secondary to the high position of the larynx and its elastic nature. In addition, the decrease in traumatic motor vehicle injuries because of increased seatbelt and supplemental restraint system use contributes to the rarity of laryngeal trauma. Less than 50% of all laryngeal traumas are thought to result in cricoid injury.4 Females tend to have slimmer, longer necks, predisposing them to a higher susceptibility to laryngeal injury, in particular supraglottic injury. Overall, males (77% vs 33%) tend to present with the highest percentage of traumatic laryngeal injuries,1 likely secondary to greater participation in violent sports and other activities such as fighting.5 A predisposition to comminuted fractures in older persons is attributed to calcification. The most common associated injuries with laryngeal fractures are intracranial injuries (13%), open neck injuries (9%), cervical spine fractures (8%), and esophageal injuries (3%).1 Etiology Laryngeal fractures can be categorized as either penetrating or blunt injuries, which can be further categorized as either high or low velocity.6 Most commonly, trauma to the larynx occurs as a result of a motor vehicle accident (MVA) or clothesline injury. A small percentage of causes include direct blows sustained during assaults, sport injuries, hanging, manual strangulation, and iatrogenic causes. Pathophysiology The mechanism of injury reflects the causative agent. Inherent in any injury resulting in a laryngeal fracture is the possibility of skeletal disruption, specifically, cricothyroid and cricoarytenoid dislocations. Laryngeal fractures from MVAs may occur in an unrestrained passenger when the extended neck impacts the steering wheel or dashboard during rapid deceleration. The anterior force compresses the larynx against the cervical vertebrae, resulting in injury. Clothesline injuries occur when an individual in motion strikes a stationary object. The result is a crush injury to the larynx against the cervical spine. Manual strangulation is a low-velocity, high-amplitude injury that commonly results in multiple fractures without significant displacement of cartilage, early presentation of hematoma, or endolaryngeal mucosal tears. Common to all traumatic mechanisms is the direct transfer of severe forces to the larynx. These forces have the potential to produce many devastating injuries, including mucosal tears, dislocations, and fractures. Edema, hematoma, cartilage necrosis, voice alteration, cord paralysis, aspiration, and airway loss may accompany these injuries. Laryngeal injuries vary by anatomical location. Supraglottis: Traumatic forces commonly produce horizontal fractures of the thyroid alae and disruption of the hyoepiglottic ligament with subsequent superior and posterior displacement of the epiglottis. Repositioning of the epiglottis may result in the creation of a false lumen anterior to the epiglottis. This lumen may tunnel into the larynx or pass anterior to the thyroid cartilage and cause cervical emphysema. Glottis: Traumatic force results in cruciate fractures of the thyroid cartilage near the attachment of the true vocal cords. Subglottis: Crushing forces to the cricoid cartilage cause injury to the cricothyroid joint and may result in bilateral vocal cord paralysis from recurrent laryngeal nerve damage. Hyoid bone: Found more commonly in women, hyoid fractures tend to occur in the central part of the hyoid bone because of the inherent strength of the cornua. Cricoarytenoid joint: Traumatic forces that displace the thyroid alae medially or cause compression of the larynx against the cervical vertebrae often result in cricoarytenoid dislocation. This injury generally occurs unilaterally. Cricothyroid joint: Injury occurs when traumatic forces to the anterior portion of the neck cause the inferior cornu of the thyroid cartilage to be displaced posterior to the cricoid cartilage. This dislocation limits cricothyroid muscle function and therefore pitch control. Injury to the recurrent laryngeal nerve may also contribute to vocal cord paralysis. Presentation Suspect upper-airway injury in any patient who has signs of cervical trauma. Common presenting symptoms in patients with laryngeal trauma include hoarseness, neck pain, dyspnea, dysphonia, aphonia, dysphasia, odynophonia, and odynophagia; however, no single symptom correlates well with the severity of laryngeal injury. A thorough physical examination is vital to the appropriate management of laryngeal injury. Before progressing to other areas of physical examination, the cervical spine must first be cleared of injury. Common signs of laryngeal injury include stridor, subcutaneous emphysema, hemoptysis, hematoma, ecchymosis, laryngeal tenderness, vocal cord immobility, loss of anatomical landmarks, and bony crepitus. Suspect an acute fracture if tenderness is present upon palpation of the larynx. Assess for supraglottic airway obstruction if inspiratory stridor is present and lower airway injury if expiratory stridor is evident. Further examination of the glottis is necessary if a combination of inspiratory and expiratory stridor is present. Indications After completing a thorough clinical examination and review of radiologic studies, laryngeal damage can be staged as described below. This classification system can then be used to direct management of the patient and to predict morbidity and mortality. Management of Laryngeal Trauma Open table in new window [ CLOSE WINDOW ] Table Group Symptoms Signs Management Group 1 Minor airway symptoms Minor hematomas Observation Small Lacerations Humidified air No detectable fractures Head of bed elevation Group 2 Airway compromise Edema/hematoma Tracheostomy Minor mucosal disruption Direct laryngoscopy No cartilage exposure Esophagoscopy Group 3 Airway compromise Massive edema Tracheostomy Mucosal tears Direct laryngoscopy Exposed cartilage Esophagoscopy Vocal cord immobility Exploration/repair No stent necessary Group 4 Airway compromise Massive edema Tracheostomy Mucosal tears Direct laryngoscopy Exposed cartilage Esophagoscopy Vocal cord immobility Exploration/repair Stent required Group Symptoms Signs Management Group 1 Minor airway symptoms Minor hematomas Observation Small Lacerations Humidified air No detectable fractures Head of bed elevation Group 2 Airway compromise Edema/hematoma Tracheostomy Minor mucosal disruption Direct laryngoscopy No cartilage exposure Esophagoscopy Group 3 Airway compromise Massive edema Tracheostomy Mucosal tears Direct laryngoscopy Exposed cartilage Esophagoscopy Vocal cord immobility Exploration/repair No stent necessary Group 4 Airway compromise Massive edema Tracheostomy Mucosal tears Direct laryngoscopy Exposed cartilage Esophagoscopy Vocal cord immobility Exploration/repair Stent required Relevant Anatomy Collectively, the hyoid bone, the thyroid and cricoid cartilages, and the cricothyroid and thyrohyoid membranes form the laryngeal architecture. The arytenoid, corniculate, and cuneiform cartilages also contribute to the laryngeal structure. Membranes, ligaments, and muscles connect the entire framework (see Images 4-5). Posterior view of the laryngeal cartilages and ligaments. Posterior view of the laryngeal cartilages and ligaments. Sagittal view of the laryngeal cartilages and ligaments. [ CLOSE WINDOW ] Sagittal view of the laryngeal cartilages and ligaments. The thyroid cartilage is the largest cartilage of the larynx. The shieldlike shape of this cartilage provides protection to the internal components of the larynx. Its 2 quadrilateral plates (right and left lamina) meet to form the laryngeal prominence (Adam's apple). The superior portion of this protuberance forms the superior thyroid notch. Inferiorly, the laryngeal prominence forms the inferior thyroid notch. Superior and inferior cornua project from the posterior margin of each side. The lower cornu articulates with the lateral edges of the cricoid cartilage and forms the cricothyroid joint. The thyrohyoid ligament connects the upper thyroid cornu to the greater cornu of the hyoid bone. The thyrohyoid membrane extends between the hyoid bone and the upper surface of the thyroid cartilage. The cricothyroid membrane extends between the thyroid and cricoid cartilages. The oblique line, the attachment site for the sternothyroid, thyrohyoid, and inferior pharyngeal constrictor muscles, is located on the outer surface of the thyroid cartilage. Like the thyroid cartilage, the cricoid cartilage also protects the internal laryngeal structures. The cricoid cartilage is the only true supporting structure of the laryngeal skeleton and is shaped like a signet ring. Anteriorly, this cartilage forms a relatively narrow band, while posteriorly it forms a larger lamina that is approximately 2-3 cm high. The cricothyroid articulation occurs at each junction of the lamina and arch. The inferior horn of the thyroid cartilage articulates with each side of the cricoid cartilage. The hyoid bone provides additional support to the larynx. The membrane attached to the hyoid bone elevates the larynx to prevent aspiration. The anterior body and the 2 greater cornua are directed posteriorly, and the 2 lesser cornua project superiorly. The epiglottis is a flexible, leaflike, elastic, cartilaginous structure that tapers inferiorly to become a stalklike extension called the petiole. The petiole is the attachment site for the thyroepiglottic ligament, which connects the epiglottis to the laryngeal prominence. The superior part of the epiglottis is located posterior to the tongue and anterior to the laryngeal aditus and is not protected by the thyroid cartilage. Laterally, the aryepiglottic folds attach the epiglottis to the arytenoid cartilage. The hyoepiglottic and thyroepiglottic ligaments help stabilize the epiglottic cartilage. The paired arytenoid cartilages are located on the superior-posterior border of the cricoid cartilage lamina. The triangular base of each arytenoid cartilage has 3 surfaces (posterior, anterolateral, medial) for the attachment of muscles and ligaments. The transverse arytenoid muscle attaches to the posterior surface. The vestibular ligament and the thyroarytenoid and vocalis muscles attach to the anterolateral surface. The medial surface contains laryngeal mucous glands. The base of each arytenoid also has a posterolateral muscular process (to which the posterior and lateral cricoarytenoid muscles attach) and an anterior caudal vocal process (to which the vocal ligaments attach). A cricoarytenoid joint is situated at the base of each arytenoid cartilage. The corniculate cartilages (of Santorini) are located superior to the arytenoid cartilages. The cuneiform cartilages (of Wrisberg) are located lateral and superior to the corniculate cartilages. The triticeous cartilage is located in the thyrohyoid ligament. The quadrangular membrane is elastic tissue that forms the intrinsic ligaments of the larynx— one of which is the vocal ligament. The quadrangular membrane attaches posteriorly to the upper arytenoid and corniculate cartilages. It then travels across the upper larynx to the lateral margin of the epiglottis. The lower margin of this membrane is the ventricular ligament, and the superior margin supports the aryepiglottic fold. The conus elasticus (cricothyroid membrane) bridges the space between the cricoid and thyroid cartilages. Posteriorly, the conus elasticus attaches to the arytenoid cartilage and vocal process on each side. The vocal processes project outward to form the vocal ligaments, which join anteriorly to form the anterior commissure. The ventricular ligaments attach to the superior part of the arytenoid cartilage and then across the larynx to attach to the thyroid cartilage just superior to the vocal ligaments. The ventricular ligament forms the lower free margin of the quadrangular membrane and also forms part of the plica ventricularis. The boundaries of the laryngeal aditus include the epiglottis anteriorly, the corniculate cartilages posteriorly, and the aryepiglottic folds laterally. The inferior border of the larynx is the cricoid cartilage. The larynx is divided into the supraglottis (vestibule), glottis (ventricle), and subglottis regions. The supraglottis extends from the laryngeal inlet to the vestibular folds. The vestibular folds (ie, false vocal cords, superior vocal cords) are attached anterior to the thyroid cartilage just inferior to the attachment site for the epiglottis. Posteriorly, the folds attach to the arytenoid cartilages. The ventricle of the larynx (ventricle of Morgagni) is the space between the vestibular and true vocal folds. The anterior segment of this ventricle extends into a diverticulum known as the laryngeal saccule or appendix of the laryngeal ventricle. The true vocal cords are located inferior to the ventricle. The area between the true vocal cords is known as the glottis. The glottis is considered to be the narrowest portion of the larynx. The glottic slit (rima glottidis) is the slit that separates the true vocal cords from the arytenoid cartilages. The subglottic area extends from the glottis to the cricoid cartilage. The conus elasticus forms the lateral boundary of the subglottis. The true vocal cord consists mainly of the thyroarytenoid muscle. The thyroarytenoid muscles connect the arytenoid cartilage to the inner aspect of the thyroid cartilage. The medial and lateral bellies of each muscle parallel each other. The medial belly is called the vocalis muscle, and the lateral belly extends superiorly and inserts in the thyroid cartilage. The cricoarytenoid muscles are important for proper laryngeal function. The lateral cricoarytenoid muscle stretches from the muscular process of the arytenoid to the upper lateral cricoid cartilage. The posterior cricoarytenoid muscle stretches from the muscular process of the arytenoid to the posterior portion of the cricoid. This muscle is the only muscle that can abduct the vocal cords. The interarytenoid muscles attach one arytenoid to the other. The lateral cricoarytenoid and the interarytenoid muscles mediate adduction of the vocal cords. The interarytenoid muscles are the only laryngeal muscles to have bilateral innervation from the recurrent laryngeal nerves. Recurrent laryngeal nerves innervate all of the other intrinsic muscles. The cricothyroid muscle is the only extrinsic laryngeal muscle innervated by the external branch of the superior laryngeal nerve (a branch of cranial nerve X). This muscle originates from the lower thyroid cartilage and attaches to the cricoid cartilage. Innervation and blood supply The vagus nerve provides the primary sensory innervation to the larynx. The internal laryngeal branch of the superior laryngeal nerve (of the vagus nerve) provides sensory innervation above the vocal cords, including the taste buds. The recurrent laryngeal nerve provides sensory innervation below the vocal cords. All of the intrinsic laryngeal muscles are innervated by the recurrent laryngeal nerve, and the extrinsic muscles (cricothyroideus) are innervated by the external branch of the superior laryngeal nerve. The blood supply to the larynx parallels the nerves and consists primarily of the superior laryngeal artery (branch of the superior thyroid artery) and the inferior laryngeal branch of the inferior thyroid artery. The cricothyroid branch of the superior thyroid artery also supplies the larynx. The inferior laryngeal artery, a branch of the inferior thyroid artery, accompanies the recurrent laryngeal nerve to the larynx. The superior and inferior laryngeal veins supply venous drainage from the larynx. These veins are branches of the superior and inferior thyroid veins, respectively. More on Laryngeal Fractures Laryngeal Fractures: Workup Author: Samir S Pancholi, DO, Consulting Surgeon, Cosmetic Surgery of Las Vegas; Adjunct Assistant Professor of Cosmetic Surgery, Touro University; Assistant Professor of Otolaryngology-Facial Plastic Surgery, Michigan State University Coauthor(s): Wayne K Robbins, DO, FAOCO, Program Director, Department of Otolaryngology-Facial Plastic Surgery, Genesys Regional Medical Center, Michigan State University; Alpesh Desai, DO, Assistant Professor, Department of Dermatology, Western University of Health Sciences; Tejas Desai, DO, Staff Physician, Department of Dermatology, Western University of Health Sciences Contributor Information and Disclosures Updated: Jan 9, 2009 Print This Email This Overview Workup Treatment Follow-up Multimedia References Keywords Workup Laboratory Studies General trauma (Advanced Trauma Life Support [ATLS]) protocol is indicated for any individual who is severely injured. The airway must be secured, and other organ systems (eg, cardiac, pulmonology, vascular) must also be stabilized. Before any diagnostic study can be performed, life-threatening injuries, such as vascular injuries or internal bleeding, must be corrected. Generally, in the setting of a laryngeal fracture, chest and cervical spine radiographs are obtained to exclude associated cervical injuries. Other nonroutine studies that may be helpful are cervical arteriography and water-soluble contrast studies of the esophagus and pharynx. Laryngeal fractures are usually suspected based on symptoms and physical findings, but direct visualization of the larynx is critical to define the extent and location of injury. Endoscopy is the mainstay for direct visualization of the larynx and its surrounding structures. Abnormalities such as edema, hematomas, tears, exposed cartilage, vocal cord avulsion, vocal cord paralysis, and arytenoid dislocation can be assessed via endoscopy. Transnasal fiberoptic laryngoscopy is the procedure of choice in this setting because this procedure can assess the airway in the dynamic state and identify any abnormalities. Indirect laryngoscopy is usually avoided because of the gagging and coughing it elicits in a patient with an already compromised airway. When the cause of laryngeal injury is not readily apparent, histological studies can help to determine the cause of injury and detect other macroscopic overlooked injuries.7 Imaging Studies CT scanning is the imaging modality of choice to assess laryngeal anatomy.8,9 A clear understanding of the Schaefer classification of laryngeal injuries is required to prevent morbidity and mortality. This classification system is based on a combination of the CT and endoscopic findings, which dictate treatment modalities. o CT scanning can help detect laryngeal fractures in a patient with no clinical signs or symptoms. In patients with minor injuries and minimal symptoms (eg, edema, ecchymosis, small hematomas), a CT scan is unlikely to provide new information that would alter treatment. Similarly, a patient with airway compromise and clinically obvious fractures requires aggressive surgical treatment regardless of CT findings. o Used judiciously, information gained from a CT scan will guide proper management of the patient's condition and prevent unnecessary surgical exploration; thus, the CT scan is a cost-effective means of assessing laryngeal anatomy.8 o CT devices capable of spiral technique and subsecond scan times, specifically those that can reconstruct 2-dimensional axial sections, 2-dimensional coronal and sagittal images, and 3-dimensional images, can provide optimal imaging results.10 Interest in the use of 3-dimensional CT images is currently growing. This innovative and highly useful tool can provide useful information when attempting to diagnose a laryngeal fracture. Because of the complexity of laryngeal anatomy, 3-dimensional CT imaging is especially useful when conventional CT, MRI, and fibroscopy are unable to reveal laryngeal trauma.11 MRI has not gained acceptance as an evaluative tool for laryngeal fractures or trauma because of the length of time required to complete the scan and the increased physical demands placed on the patient (eg, holding breath for a long period).12 In addition, MRI is not helpful for imaging skeletal structures. Diagnostic Procedures The procedures below are used to evaluate patients with suspected laryngeal trauma. o Fiberoptic nasopharyngoscopy: This procedure is performed in a conscious patient, with topical anesthesia. The goal of the procedure is to evaluate vocal cord function and to perform a preliminary assessment of the extent of trauma. o Direct laryngoscopy: This procedure provides a detailed visual examination of the larynx. Instrumentation such as the Dedo or Pilling laryngoscope provides excellent visualization; however, complete examination of the anterior commissure may require special instrumentation. o Bronchoscopy: This procedure may be performed with either a flexible or rigid bronchoscope, depending on the experience of the operator. Examination allows observation of the subglottic larynx and supporting structures. o Esophagoscopy: This procedure allows visualization of the esophageal mucosa for traumatic lacerations. It may be performed with either a flexible or rigid esophagoscope, depending on the experience of the operator. Traumatic injury is common in the retrolaryngeal esophagus; therefore, close evaluation is required. Laryngeal Fractures: Treatment Author: Samir S Pancholi, DO, Consulting Surgeon, Cosmetic Surgery of Las Vegas; Adjunct Assistant Professor of Cosmetic Surgery, Touro University; Assistant Professor of Otolaryngology-Facial Plastic Surgery, Michigan State University Coauthor(s): Wayne K Robbins, DO, FAOCO, Program Director, Department of Otolaryngology-Facial Plastic Surgery, Genesys Regional Medical Center, Michigan State University; Alpesh Desai, DO, Assistant Professor, Department of Dermatology, Western University of Health Sciences; Tejas Desai, DO, Staff Physician, Department of Dermatology, Western University of Health Sciences Contributor Information and Disclosures Updated: Jan 9, 2009 Print This Email This Overview Workup Treatment Follow-up Multimedia References Keywords Treatment Medical Therapy Primarily, symptoms, direct nasopharyngoscopy, and CT scanning determine the need for treatment of laryngeal fractures. For minor injuries in which edema, hematoma, or certain small, insignificant mucosal tears are identified without evidence of other injury, medical treatment is appropriate. Mucosal tears of less than 2 cm have been treated effectively without surgical intervention.13 The goal of medical treatment is to return the patient to preinjury laryngeal function, which includes ventilation, phonation, and protection of the lower airway. Typically, in such minor injuries, tracheotomy is not required; however, close clinical observation is essential in the first 24-48 hours after injury. Bed rest is recommended for patients treated medically for laryngeal trauma, with the head of the bed elevated 30-45°. Voice rest is recommended to minimize edema, hematoma formation, and subcutaneous emphysema. Humidified air reduces crust formation and transient ciliary dysfunction. Supplemental oxygen is usually not needed and may be harmful in some patients (eg, patients with chronic obstructive pulmonary disease). Arterial blood gas (ABG) testing can be used to determine the need for supplemental oxygen. Initially, a nothing by mouth (NPO) status is recommended for patients with laryngeal fractures and mucosal tears, followed by a clear liquid diet.13 Diet regimens should mirror the severity of injury. Those patients without visible mucosal lacerations or fractures can initiate a clear liquid diet earlier than those patients with more severe injuries. Patients with severe injuries may require total parenteral nutrition supplementation during their NPO period. Avoid the use of nasogastric tubes for suctioning or feeding because of the potential for worsening laryngeal injury that results from local trauma during tube placement. The benefit of using systemic corticosteroids is controversial. Many otolaryngologists believe that corticosteroids are necessary to retard inflammation, swelling, and fibrosis and to help prevent granulation tissue formation. Systemic corticosteroids are helpful only in the first few days after the injury. The use of antibiotics is not necessary in the treatment of minor laryngeal trauma in which cartilaginous fractures and mucosal tears are not identified. However, when tears are visualized or with compound fractures of the larynx, systemic antibiotics should be used to reduce the high risk of local infection and perichondritis, which may delay healing and promote airway stenosis. The use of antireflux medications, such as H2-receptor antagonists and proton pump inhibitors, can help to reduce granulation tissue formation and tracheal stenosis. Use these medications throughout the emergent and convalescent phases of medical treatment for laryngeal fractures. Surgical Therapy The surgical management of an unstable patient can be guided by the flow diagram depicted in Image 6. Management protocol for laryngeal trauma. [ CLOSE WINDOW ] Management protocol for laryngeal trauma. The information gained from the history, physical examination, endoscopic procedures, and imaging studies serves as an important tool when planning a neck exploration. If the airway is compromised, a tracheotomy should be performed, preferably with the patient awake under local anesthesia with mild sedation. Usually, a tracheal incision is made at a position lower than that for standard tracheotomy. An incision below the third or fourth ring is preferred when managing the airway that has laryngeal trauma. This position helps to avoid further injury to the larynx and its supporting structures. Surgical exploration begins with a horizontal skin incision in a skin crease at the level of the cricothyroid membrane. A subplatysmal apron flap is then elevated superior to the hyoid bone and inferior to expose the cricoid cartilage. Extension of the incision site facilitates examination of neural, vascular, and visceral injuries. The strap muscles are separated in the midline and are retracted laterally so that the laryngeal skeleton can be assessed adequately. At this point, identify and remove fractured pieces of the laryngeal cartilage. Depending on the injury, the larynx is entered through the thyrohyoid membrane, a midline thyrotomy, or the thyroid cartilage within 2-3 mm of the thyroid notch. If a thyrotomy is needed, a midline, vertical perichondrial incision is made in the thyroid cartilage. A subchondral dissection follows bilaterally. An oscillating saw or a number 15 blade can be used to cut through the thyroid cartilage, with care to avoid trauma to the endolaryngeal mucosa. After the thyroid cartilage is divided, the endolaryngeal mucosa is sharply divided. The endolarynx is examined in its entirety to identify the full extent of injury. The arytenoids are palpated to evaluate their mobility and position. Vocal cords are repaired using 5-0 or 6-0 absorbable sutures. Suturing the anterior surface of each damaged cord to the external perichondrium with 4-0 absorbable sutures resuspends the vocal cord. Reconstituting the anterior commissure is critical to preserving voice quality. Great care should be taken to identify and repair all mucosal lacerations with fine absorbable sutures (ie, 5-0, 6-0). Primarily close exposed cartilage with meticulous technique to minimize fibrosis and prevent formation of granulation tissue. Exposed cartilage that cannot be closed primarily may need skin or mucous membrane grafts. In the few circumstances in which a graft is required, mucous membrane, dermis, or split-thickness grafts are suitable.14 Laryngeal cartilage fractures must be reduced and immobilized. Small, isolated cartilage fractures that have no perichondrium are débrided to prevent chondritis and vocal cord dysfunction. Traditionally, wire sutures have been used to immobilize reduced laryngeal cartilage fractures (see Image 7). Recently, however, many surgeons have begun to use metal alloy plates (miniplates) for repairing laryngeal fractures. Miniplates have been shown to effectively stabilize the laryngeal architecture (see Image 9) and reshape the larynx back to its preinjury state. They also decrease the length of hospitalization, insignificantly alter operating time, and usually add no additional discomfort to the patient.15,16 More recently, the use of absorbable miniplates has been introduced. These plates have been found to be just as safe, effective, and manageable as their alloy counterparts. They also have the advantages of improved cosmesis after resorption, less bone growth restriction, less issue with plate migration, less bony resorption, and negligible image artifact.17 Most plates are composed of polylactic acid copolymer material and used for open reduction and stabilization of displaced fractures. Sasaki et al evaluated the efficacy of both MacroPore and Leibinger restorable reconstruction plates in 3 adult male patients and found both plates to be equally easy to use. In addition, adequate skeletal stabilization was achieved, which allowed for early phonation and respiratory function without long-term stenting.18 In Brazil, de Mello-Filho et al performed a retrospective study on the efficacy of adaptation plate fixation (APF) to repair the larynx. This group had no complications with the use of APF, and 19 out of 20 patients recovered their voices.19 Regardless of the method, the goal of surgical intervention is to restore the 3 primary functions of the larynx: breathing, phonating, and swallowing. Using permanent sutures or wires, the thyrotomy is then closed, and the strap muscles are reapproximated. The nasogastric tube is then placed using direct visualization. Preoperative Details Proper patient positioning is essential when planning a neck exploration and may require hyperextension of the patient's neck after first clearing the cervical spine. The neck and tracheotomy site is prepared and draped in sterile fashion. The midcervical transverse thyrotomy incision is marked and injected with local anesthetic. Intraoperative Details Perhaps the most important portion of the surgery is injury assessment. Failure to adequately assess for potential injuries can result in disastrous consequences. Important structures, such as the larynx, cricoid, both recurrent laryngeal nerves, and the esophagus, must be identified and evaluated. Repair esophageal injuries before manipulating the trachea. When performing the thyrotomy, use electrocautery to make the transverse incision in the cricothyroid membrane. When using the saw or a number 15 blade, exercise extreme caution to avoid entering the lumen. Placing the patient in the Trendelenburg position can sometimes provide better visualization of the subglottic region. If required, resuspension of the vocal cords must be the last step before closure of the thyrotomy. Prior to this step, all other structures must be stabilized. Postoperative Details If a tracheotomy is performed, the tube is left in place for a minimum of 5 days. Decannulation depends on several factors and should be performed on a case-by-case basis. Prophylactic antibiotics are used for at least 5 days. If a stent is used, antibiotics are continued until stent removal (usually 2-3 wk). Tube feedings are continued for at least 5-10 days. Follow-up Facial plastic and reconstructive surgery may be necessary in the future. Other procedures, such as destruction of granulation tissue, stenosis, and webs, may also be required. Patients are monitored closely for the first 6-12 months after the initial injury. Complications Complications include the following: Acute o o o o o o Airway obstruction Aphonia Dysphonia Odynophagia Dysphagia Postoperative complications (eg, hematoma, infection) Chronic o Voice compromise (21-25%)20,21 o Chronic obstruction (15-17%)20,21 o Vocal cord injuries (eg, paralysis, fixation) o Fistula (tracheoesophageal, esophageal, or pharyngocutaneous) o Cosmetic deformity o Chronic aspiration o Inability to decannulate Injury to the recurrent laryngeal nerve is a dreaded complication of surgery and may cause vocal fold impairment. Unilateral injuries result in a weak voice, and bilateral injuries can cause respiratory compromise. Unless the recurrent laryngeal nerve is severed during surgery, no intervention is needed. However, if no improvement is noted after 6-12 months, a thyroplastytype vocal cord medialization procedure can be performed to strengthen the voice. The vocal cord can be injected with Gelfoam if aspiration or dysphonia is present and severe. 14 This procedure is only a temporary solution. Cricoarytenoid joint fixation must be excluded before initiating any of these procedures.22 To accomplish this goal, assess vocal cord mobility using direct laryngoscopy, and assess arytenoid mobility using direct palpation. If an adequate airway and voice are present, no treatment is needed. Bilateral arytenoid fixation or recurrent laryngeal paralysis with an unstable airway is treated with arytenoidectomy, cordotomy, or vocal cord lateralization. The most common problem in the immediate postoperative period is the development of granulation tissue and ulceration from exposed cartilage. Granulation tissue may be decreased with the use of antibiotics and stents if the stents are removed in a timely fashion. The main concern with granulation tissue formation is the potential for the development of fibrosis and eventually stenosis. Many techniques have been used to slow the formation of granulation tissue, including systemic and intralesional administration of corticosteroids, long-term splinting, and low-dose radiation. These techniques have resulted in little success.14 Debulking granulation tissue through endoscopy is probably the most effective alternative treatment currently available. Subglottic stenosis is a difficult complication to treat effectively. Incomplete ring and weblike subglottic stenosis can be treated with laser excision or incision and dilation.23 More significant stenosis may require anterior or posterior cricoid splits with cartilage grafting. Direct laryngoscopy and bronchoscopy should be performed during the follow-up period to examine the extent of stenosis. Laryngeal trauma complications can manifest as inadequate voice and failure to decannulate. These can be prevented or treated in the following ways: Granulation tissue o Covering all exposed cartilage to prevent o Avoiding stents when possible o Careful excision Laryngeal stenosis o Excision with mucosal coverage o Stenting selected cases o Laryngotracheoplasty o Tracheal resection with reanastomosis Vocal fold immobility o Observation o Vocal fold injection o Thyroplasty-type vocal fold medialization o Arytenoidectomy and vocal fold lateralization for bilateral paralysis Laryngeal Fractures: Follow-up Author: Samir S Pancholi, DO, Consulting Surgeon, Cosmetic Surgery of Las Vegas; Adjunct Assistant Professor of Cosmetic Surgery, Touro University; Assistant Professor of Otolaryngology-Facial Plastic Surgery, Michigan State University Coauthor(s): Wayne K Robbins, DO, FAOCO, Program Director, Department of Otolaryngology-Facial Plastic Surgery, Genesys Regional Medical Center, Michigan State University; Alpesh Desai, DO, Assistant Professor, Department of Dermatology, Western University of Health Sciences; Tejas Desai, DO, Staff Physician, Department of Dermatology, Western University of Health Sciences Contributor Information and Disclosures Updated: Jan 9, 2009 Print This Email This Overview Workup Treatment Follow-up Multimedia References Keywords Outcome and Prognosis The overall outcome and prognosis of a patient with a laryngeal fracture depends on several factors, such as extent of injury, timing of repair, and the ability of the otolaryngologist to properly evaluate and treat the patient who has been traumatized. Generally, success is measured in terms of voice and airway function. Minor injuries usually result in return to preinjury airway and voice status. More significant trauma results in voice changes and requires more intensive procedures for airway stabilization. Certain factors have been identified that correlate with a good outcome. Although controlling some of these factors is virtually impossible, a basic understanding and knowledge of these indicators can help predict the ultimate morbidity or mortality of a patient. Early repair of injury is essential in obtaining the best outcome. Evidence suggests that ideal timing for the repair of laryngeal fractures is within the first 24-48 hours after injury.24,25 If repair occurs later, the rate of complications (dysphonia, aspiration, and tracheotomy dependence) increases considerably. Early repair decreases the complications of chronic airway obstruction, poor voice quality, persistent granulation tissue, wound contractures, and stenosis. After studying 392 patients with laryngeal trauma, Jewett (1999) found an increased mortality rate (0.78% vs 0.5%) in patients in whom tracheostomy was performed versus those in whom it was not performed.1 The reason for tracheostomy was unclear and possibly associated with other common associated injuries (eg, head or chest injury). Penetrating trauma is prognostically more favorable than blunt trauma. Leopold (1983) found that penetrating trauma resulted in good airway function 93% of the time, and 70% of patients recovered with excellent voice quality. In contrast, 68% of patients who had sustained blunt trauma had good airway function, while 39% of patients recovered with excellent voice quality. Vocal cord mobility is another documented favorable prognostic sign. Vocal cord dysfunction usually results from recurrent laryngeal nerve injury or arytenoid subluxation. Leopold's study revealed that good airway function was found in 81% of patients with good vocal cord mobility, while good airway function was found in only 72% of patients with vocal cord dysfunction. The data are even more impressive when voice change was compared. Excellent voice quality was found in 56% of patients with normal vocal cords, while excellent voice quality was found in only 17% of patients with vocal cord immobility (1983).26 Much controversy exists regarding the use of laryngeal stents and whether their use improves patient outcome in laryngeal trauma. Inherent difficulties arise when measuring their influence because most injuries that require stent placement are severe and probably will have some complications regardless of stent use. The basic tenet for the use of laryngeal stents requires that they serve as internal fixation devices and as a means of preventing endolaryngeal scarring; however, the use of stents is associated with risks. Stents may increase the prevalence of infection and granulation tissue formation. Specific indications are needed for their use, including multiple cartilaginous fractures, anterior commissure lacerations, and significant distortion of laryngeal architecture. Stent placement does not serve as a substitute for primary closure of mucosal lacerations and reduction and internal fixation of laryngeal fractures.14,27 Patients treated without stents had better resultant airway function (88% of patients without stents vs 71% of patients with stents).26 Similarly, patients treated without stents had better voice results (61% of patients without stents had excellent voice results vs 33% of patients with stents).26 Choices of stents range from finger clots with foam rubber to commercially prepared polymeric silicone stents. Place the material in the larynx so that the material moves freely with the larynx during swallowing. Also, contour the stents to the shape of the larynx to avoid mucosal damage. If internal sutures break, use a 4-point fixation device to allow an easier recovery from the stent. Most authors agree that stents should be removed in 10-14 days. Future and Controversies Because of the rarity of serious laryngeal trauma, limited clinical research is available to guide treatment decisions. The poor results associated with the use of internal stents remains an obstacle in treatment. Research that describes specific injuries necessitating the use of stents will help to improve outcomes. Recently, investigation and clinical use of adaptation plates to stabilize laryngeal fractures has shown promising results and may reduce future need for internal laryngeal stents. Further investigation into the use of absorbable polyvicryl miniplates or mesh could reduce long-term complications. Several promising techniques that may be beneficial in the future of laryngotracheal reconstruction have been recently described. Several authors have described the use of autogenous laryngeal cartilage in laryngotracheal reconstruction.28 Others have described the use of tracheal homografts from cadavers.29 In 1998, at the Cleveland Clinic, the first laryngeal transplant was performed in a patient who lost phonation after a motorcycle accident. Reports of patients with laryngeal transplants suggest good-to-excellent results in phonation and airway.30 Perfecting laryngeal transplantation in the future could provide an alternative for patients with poor outcomes resulting from laryngeal fractures. Acknowledgments I would like to thank Drs. Alpesh Desai and Tejas Desai for their hard work, long hours, initiative, dedication, and assistance in getting this article off the ground and into publication.