File - Managment of Acute Overdose

Management of Acute Overdose
By: Peter Rempel
March 27 th , 2013
Presentation Outline
Introduction and Statistics
General management strategy
Identification of Toxidromes
Management of overdose for specific medications
Role of pharmacist
Introduction - Overdose
Definition: The use of a substance in quantities greater than recommended.
Accidental vs. Intentional misuse
Epidemiology - Overdose
Approximately 2.3 million cases reported (US)
50% caused by pharmaceutics
41,592 deaths occurred in the US (2009)
76% were unintentional
91% caused by medications
Prevalence higher in males during the early years (0-12y)
Rates in females surpass males in older populations
Epidemiology (Continued)
Most common pharmaceutics:
Analgesics (Opioids)
Sedative/hypnotic/antipsychotics
Antidepressants
Antihistamines
Cardiovascular drugs
Vitamins, cough and cold products
Rates of unintentional overdose has been steadily increasing
4)
5)
6)
1)
2)
3)
General Management Strategy
ABC management (vital signs)
Call Poison Control
Obtain best possible medical history
Order Labs
Prevent absorption of toxin
Enhance elimination (antidote)
General management strategy
1)
•
•
•
ABC management
Airway patency
- head-tilt and chin-lift, removal of obstructions
Breathing
assisted ventilation
Circulation
colour change, sweating, decreased LOC
- EKG, saline infusion, vasopressers
General Management Strategy
2)
Call Poison Control
Available 24/7 to provide poison treatment information
Help guide treatment strategy
Prevent unnecessary use of health care resources http://www.capcc.ca/provcentres/on/on.html
General Management Strategy
3)
Obtain accurate history
Determine the causative agent
Dose
Time since exposure
Route
Demographics (age, weight)
Symptoms*
Physical Examination
What if you don’t know what medication/poison was ingested?
Identification of Toxidromes
What is a Toxidrome?
Characteristic symptoms that are associated with a specific group of medications.
These group of symptoms are known as a
“Toxidrome”
Identification of Toxidromes
Cholinergic Toxidrome
“SLUDGE”
Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis
Miosis, diaphoresis, bradycardia
Causative Agents: Physostigmine, Organophosphates,
Carbamate
Identification of Toxidromes
Anticholinergic Toxidrome
Hot as a Hare - fever
Red as a Beet - flushing
Mad as a Hatter – confusion, delirium
Dry as a bone – dry skin/mucus membranes
Mydriasis, tachycardia, urinary retention
Causative Agents: Antihistamines, TCA`s, Antiparkinson medications
Identification of Toxidromes
Sympathomimetic Toxidrome
Anxiety, Delusions, Sweating, Piloerrection, Seizures,
Hyperreflexia, Mydriasis
Causative Agents: cocaine, salbutamol,, amphetamines, ephedrine, pseudoephedrine, methamphetamine
Identification of Toxidromes
Sedative/Hypnotic/Opiate Toxidrome
Slurred speech, confusion , stupor, coma, apnoea, respiratory depression
Hypotension, bradycardia, miosis
Causative agents: opioids, anticonvulsants, antipyschotics, barbiturates, benzodiazepines, ethanol
Back to the Management Strategy
General Management Strategy
4)
Order lab tests
Confirm offending agent(s)
Predict prognosis
Direct therapy/monitoring
Includes: Toxicology screen, anion gap, osmol gap,
CBC, BUN, SCr, blood glucose, electrolytes, EKG monitoring
General Management Strategy
5)
Prevent absorption
*Activated Charcoal- first line therapy in most emergency departments
Whole Bowel Irrigations- clears the GI tract using high volumes of PEG
Orogastric Lavage- No benefit over the use of activated charcoal
Syrup of Ipecac- NO LONGER RECOMMENDED http://www.freepatentsonline.com
/7077825.html
General Management Strategy
Activated Charcoal
Ability to adsorb substances due to its high surface area
Offending agent(s) become trapped by the charcoal and are excreted in the feces
Dosing: 1g/kg po OR by NG tube (usually given multiple times)
AE: aspiration pneumonia, GI obstruction
Contraindications: presence of ileus
General Management Strategy
Activated Charcoal
Does not adsorb the following compounds:
Iron
Lithium
Lead
Cyanide
Alcohol
General Management Strategy
6)
Enhance Elimination
Hemodialysis/Hemoperfusion
Administer Antidote
General Management Strategy
Administer Antidote:
Offending Agent
Tylenol
Anticholinergics
Benzodiazepines
CCB
Beta Blockers
Opioids
Antidote
N-acetylcysteine
Physostigmine
Flumazenil
Glucagon, Calcium
Glucagon
Naloxone
*See my website for a more exhaustive list www.ODmanagement.weebly.com
Opioid Overdose Managment
Opioid Overdose Management
Signs and Symptoms?
Hint: Remember the toxidrome!
Opioid Overdose Management
Signs and Symptoms?
Hint: Remember the toxidrome!
Decreased LOC, RR, GI motility
Hypotension, bradycardia, miosis
Naloxone
Reverses effects from opioid overdose
Pure opioid receptor antagonist
Duration of action 30-120 minutes
0.4-2mg (IV,IM,SC); repeat q2-3 minutes until reversal of symptoms
Use continuous IV infusion for exposure to long-acting opioids or SR formulations
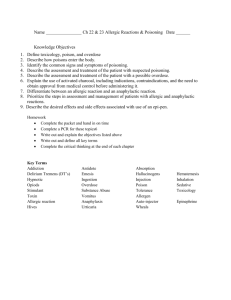
Acetaminophen Overdose
Hamm J. Acute acetaminophen overdose in adolescents and adults.Critical Care Nurse; Jun 2000; 20(3) 69-74
Hamm J. Acute acetaminophen overdose in adolescents and adults.Critical Care Nurse; Jun 2000; 20(3) 69-74
N-acetylcysteine
Indicated for the reversal of Acetaminophen toxicity
Hepatoprotective agent
Restores hepatic glutathione and acts as a glutathione substitute
Prevents the production of the toxic by-product of acetaminophen
N-acetylcysteine Dosing
21 hour IV dosing regimen (3 doses)
LD: 150 mg/kg (Max 15g) over 1 hour
2 nd dose: 50 mg/kg (max 5g) over 4 hours
3 rd dose: 100 mg/kg (max 10g) over 16 hours
Oral dosing regimen also available (72 hours)
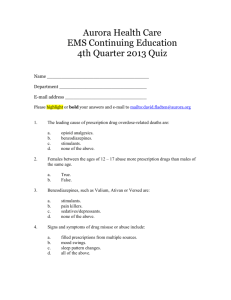
Therapy is guided by the Matthew-Rumack
Nomogram
Matthew-Rumack Nomogram
The Merck Manual for Health Professionals. Acetaminophen Poisoning.
http://www.merckmanuals.com/professional/injuries_poisoning/poisoning/acetaminophen_poisoning.html
Anaesthetic Overdose/Refractory Cases
Lipids 20%- Intralipid®
Used in anaesthetic overdose and refractory cases
(unlabelled use)
Mechanism unknown
Effective for lipophilic medication overdose
Suggested Dose:
1.5 mL/kg bolus infused over 1 minute (may repeat up to 2 times)
Followed by 0.25 mL/kg/minute continuous infusion http://www.lipidrescue.org/
Role of the Pharmacist
Role in both the community and hospital setting
Educating patients on the dangers of drug misuse
Identifying potential at risk patients
Identifying inappropriate medication regimens
Medication Reconciliation
Highlights
Majority of overdoses are accidental
Rates of accidental overdose is steadily increasing
Identifying Toxidromes plays a vital role in the management of overdose
Activated charcoal and whole bowel irrigation are effective at lowering absorption
Pharmacists can play a role in both the prevention and treatment of an overdose
References
1) Clinical Practice Guidelines. Management of Drug Overdose
& Poisoning. Ministry of Health, Singapore. May 2000.
2)
Green SL, Dargan PI, Jones AL. Acute poisoning: understanding 90% of cases in a nutshell. Postgrad Med J.
2005;81:204-216.
3)
4)
5)
Tenenbein M et al. Efficacy of ipecac-induced emesis, orogastric lavage, and activated charcoal for acute drug overdose. Annals of Emergency Medicine; 16(8): 838-841
Lab Tests Online. Emergency and Overdose Drug Tests. http://labtestsonline.org/understanding/analytes/emergenc y/tab/test : Accessed March 22, 2013
Thim T, Niels HV, et al. Initial assessment and treatment with the Airway, Breathing, Circulation, Disability, Exposure
(ABCDE) approach. International Journal of General
Medicine; 2012:5 117-121
References
6) Centers for disease control and prevention. Home and
Recreational Safety. Unintentional Poisoning Data and
Statistics. Retrieved from http://www.cdc.gov/HomeandRecreationalSafety/Poiso ning/data.html
; accessed March 3, 2013
7) Hodgman MJ et al. A review of Acetaminophen Toxicity.
Crit Care Clin. 28 (2012) 499-516
8) G Cave et al. Intravenous Lipid Emulsion as Antidote
Beyond Local Anesthetic Toxicity: A Systematic Review.
Academic Emergency Medicine: 2009; 16:815-824
9) Boyer EW. Management of Opioid Analgesic Overdose..
N Engl J Med: 367;2 146-155
Thank you for listening