Cardiovascular System
advertisement

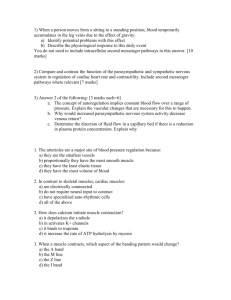
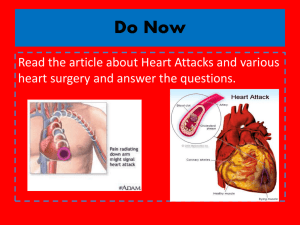
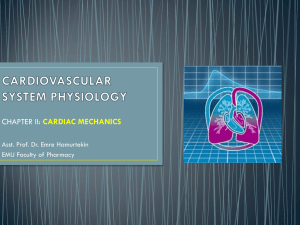
Physiology Cardiovascular System PreMMed Course 2013 East Coast Basic Science Course • What events occur in the heart each time it beats? • How much blood does the heart pump out? • What factors affect the amount of blood the heart pumps out? • How is blood pressure related to blood flow from the heart? • What are the normal cardiovascular response to hypovolaemia? • How do anaesthetics affect the cardiovascular system? Cardiovascular System Function • Functional components of the cardiovascular system: – Heart – Blood Vessels – Blood • General functions these provide – Transportation • Everything transported by the blood – Regulation • Of the cardiovascular system – Intrinsic & extrinsic – Protection • Against blood loss – Production/Synthesis Cardiovascular System Function • To create the “pump” we have to examine the Functional Anatomy – Cardiac muscle – Chambers – Valves – Intrinsic Conduction System Functional Anatomy of the Heart Cardiac Muscle • Characteristics – Striated – Short branched cells – Uninucleate – Intercalated discs – T-tubules larger and over z-discs Cardiac Ultrastructure Cardiac Myocyte Structural Unit:Sarcomere Functional Anatomy of the Heart Chambers • 4 chambers – 2 Atria – 2 Ventricles • 2 systems – Pulmonary – Systemic Functional Anatomy of the Heart Valves • Function is to prevent backflow – Atrioventricular Valves • Prevent backflow to the atria • Prolapse is prevented by the chordae tendinae – Tensioned by the papillary muscles – Semilunar Valves • Prevent backflow into ventricles Functional Anatomy of the Heart Intrinsic Conduction System • Consists of “pacemaker” cells and conduction pathways – Coordinate the contraction of the atria and ventricles Myocardial Physiology Autorhythmic Cells (Pacemaker Cells) • Characteristics of Pacemaker Cells – Smaller than contractile cells – Don’t contain many myofibrils – No organized sarcomere structure • do not contribute to the contractile force of the heart conduction myofibers normal contractile myocardial cell SA node cell AV node cells Myocardial Physiology Autorhythmic Cells (Pacemaker Cells) • Characteristics of Pacemaker Cells – Unstable membrane potential • “bottoms out” at -60mV • “drifts upward” to -40mV, forming a pacemaker potential – Myogenic • The upward “drift” allows the membrane to reach threshold potential (-40mV) by itself • This is due to 1. Slow leakage of K+ out & faster leakage Na+ in » Causes slow depolarization » Occurs through If channels (f=funny) that open at negative membrane potentials and start closing as membrane approaches threshold potential 2. Ca2+ channels opening as membrane approaches threshold » At threshold additional Ca2+ ion channels open causing more rapid depolarization » These deactivate shortly after and 3. Slow K+ channels open as membrane depolarizes causing an efflux of K+ and a repolarization of membrane Pacemaker Action Potential Myocardial Physiology Autorhythmic Cells (Pacemaker Cells) • Characteristics of Pacemaker Cells Myocardial Physiology Autorhythmic Cells (Pacemaker Cells) • Altering Activity of Pacemaker Cells – Sympathetic activity • NE and E increase If channel activity – Binds to β1 adrenergic receptors which activate cAMP and increase If channel open time – Causes more rapid pacemaker potential and faster rate of action potentials Sympathetic Activity Summary: increased chronotropic effects heart rate increased dromotropic effects conduction of APs increased inotropic effects contractility Myocardial Physiology Autorhythmic Cells (Pacemaker Cells) • Altering Activity of Pacemaker Cells – Parasympathetic activity • ACh binds to muscarinic receptors – Increases K+ permeability and decreases Ca2+ permeability = hyperpolarizing the membrane » Longer time to threshold = slower rate of action potentials Parasympathetic Activity Summary: decreased chronotropic effects heart rate decreased dromotropic effects conduction of APs decreased inotropic effects contractility Myocardial Physiology Contractile Cells • Special aspects – Intercalated discs • Highly convoluted and interdigitated junctions – Joint adjacent cells with » Desmosomes & fascia adherens – Allow for synticial activity » With gap junctions – More mitochondria than skeletal muscle – Less sarcoplasmic reticulum • Ca2+ also influxes from ECF reducing storage need – Larger t-tubules • Internally branching – Myocardial contractions are graded! Myocardial Physiology Contractile Cells • Special aspects – The action potential of a contractile cell • Ca2+ plays a major role again • Action potential is longer in duration than a “normal” action potential due to Ca2+ entry • Phases 4 – resting membrane potential @ -90mV 0 – depolarization » Due to gap junctions or conduction fiber action » Voltage gated Na+ channels open… close at 20mV 1 – temporary repolarization » Open K+ channels allow some K+ to leave the cell 2 – plateau phase » Voltage gated Ca2+ channels are fully open (started during initial depolarization) 3 – repolarization » Ca2+ channels close and K+ permeability increases as slower activated K+ channels open, causing a quick repolarization Cardiac Myocyte Action Potential Phase 0 – Rapid Depolarisation Phase 1 – Spike Phase 2 – Plateau Phase 3 – Repolarisation Phase 4 – Diastolic potential Myocardial Physiology Contractile Cells • Skeletal Action Potential vs Contractile Myocardial Action Potential Myocardial Physiology Contractile Cells • Plateau phase prevents summation due to the elongated refractory period • No summation capacity = no tetanus – Which would be fatal Summary of Action Potentials Skeletal Muscle vs Cardiac Muscle Excitation Contraction Coupling Pressure in Cardiac Chambers Cardiac Cycle • One complete sequence that occur during the contraction (systole) and relaxation (diastole) of the ventricular muscle • This activity is initiated by cardiac action potential Cardiac Cycle Coordinating the activity • Electrical Conduction Pathway Cardiac Cycle Coordinating the activity • The electrical system gives rise to electrical changes (depolarization/repolarization) that is transmitted through isotonic body fluids and is recordable – The ECG! • A recording of electrical activity • Can be mapped to the cardiac cycle Conduction speeds Tissue Conduction rate (m/s) SA node .05 Atrial pathways 1 AV node .05 Bundle of His 1 Purkinje 4 Ventricular muscle 1 • The sum of these action potential is recorded as the ECG P wave – atrial depolarisation PR interval – spread of excitation through the atria, AV node and bundle of His QRS complex – spread of excitation through the ventricles T wave – ventricular repolarisation Cardiac Cycle Phases Atrial Contraction (A-V Valves Open, Semilunar Valves Closed) • The first phase - initiated by the p wave of ECG - electrical depolarization of the atria. • Atrial depolarization then causes contraction of the atrial musculature. As the atria contract, the pressure within the atrial chambers increases, which forces more blood flow across the open A-V valves, leading to a rapid flow of blood into the ventricles. • Blood does not flow back into the vena cava because of inertial effects of the venous return and because the wave of contraction through the atria moves toward the AV valve thereby having a "milking effect." • Atrial contraction produce a small increase in venous pressure that can be noted as the "a-wave" of the left atrial pressure. Just following the peak of the a wave is the x-descent. • After atrial contraction is complete, the atrial pressure begins to fall causing a pressure gradient reversal across the AV valves. This causes the valves to float upward (pre-position) before closure. At this time, the ventricular volumes are maximal - end-diastolic volume (EDV). • The left ventricular EDV (LVEDV) ~ 120 ml, represents the ventricular preload and is associated with end-diastolic pressures of 8-12 mmHg and 3-6 mmHg in the left and right ventricles, respectively. • A heart sound is sometimes noted during atrial contraction (fourth heart sound, S4). This sound is caused by vibration of the ventricular wall during atrial contraction. Isovolumetric Contraction (All Valves closed) • This phase of the cardiac cycle begins with the QRS complex of the ECG - ventricular depolarization. • This triggers excitation-contraction coupling, myocyte contraction and a rapid increase in intraventricular pressure. Early in this phase, the rate of pressure development becomes maximal - maximal dP/dt. • The AV valves close as intraventricular pressure > atrial pressure. Ventricular contraction also triggers contraction of the papillary muscles with their attached chordae tendineae that prevent the AV valve leaflets from bulging back into the atria and becoming incompetent . Closure of the AV valves results in the first heart sound (S1) - normally split (~0.04 sec) because MV closure precedes TV • During the time between the closure of the AV valves and the opening of the aortic and pulmonic valves, ventricular pressure rises rapidly without a change in ventricular volume - no ejection occurs. • Ventricular volume does not change because all valves are closed during this phase. Contraction - "isovolumic" or "isovolumetric." • The "c-wave" noted in the LAP may be due to bulging of mitral valve leaflets back into left atrium. Just after the peak of the c wave is the x'-descent. Rapid Ejection (Aortic and Pulmonic Valves Open; AV Valves Remain Closed) • Initial and rapid ejection of blood into the aorta and pulmonary arteries from the left and right ventricles, respectively. • Ejection begins when the intraventricular pressures > the pressures within the aorta and pulmonary artery, which causes the aortic and pulmonic valves to open. • Ventricular pressure normally > outflow tract pressure by a few mmHg. This pressure gradient across the valve is ordinarily low because of the relatively large valve opening (low resistance). Maximal outflow velocity is reached early in the ejection phase, and maximal (systolic) aortic and pulmonary artery pressures are achieved. • Normally no heart sounds noted during ejection because the opening of healthy valves is silent. The presence of sounds during ejection indicate valve disease or intracardiac shunts. • Left atrial pressure initially decreases as the atrial base is pulled downward, expanding the atrial chamber. Blood continues to flow into the atria from their respective venous inflow tracts and the atrial pressures begin to rise, and continue to rise until the AV valves open at the end of phase 5. Reduced Ejection Aortic and Pulmonic Valves Open; AV Valves Remain Closed • Approximately 200 msec after the QRS and the beginning of ventricular contraction, ventricular repolarization occurs (T-wave of the ECG). • Repolarization leads to a decline in ventricular active tension and therefore the rate of ejection falls. • Ventricular pressure falls slightly below outflow tract pressure; however, outward flow still occurs due to kinetic (inertia) energy of the blood. • Left atrial and right atrial pressures gradually rise due to continued venous return from the lungs and from the systemic circulation, respectively Isovolumetric Relaxation All valves closed • When the intraventricular pressures fall sufficiently at the end of phase 4, the aortic and pulmonic valves abruptly close (aortic precedes pulmonic) causing the second heart sound (S2) and the beginning of isovolumetric relaxation. • Valve closure is associated with a small backflow of blood into the ventricles and a characteristic notch (incisura or dicrotic notch) in the aortic and pulmonary artery pressure tracings. • After valve closure, the aortic and pulmonary artery pressures rise slightly (dicrotic wave) following by a slow decline in pressure. • The rate of pressure decline in the ventricles is determined by the rate of relaxation of the muscle fibers, which is termed lusitropy. This relaxation is regulated largely by the sarcoplasmic reticulum that are responsible for rapidly re-sequestering calcium following contraction. • Although ventricular pressures decrease during this phase, volumes remain constant because all valves are closed. The volume of blood that remains in a ventricle is called the end-systolic volume ~ 50 ml in the left ventricle. The difference between the end-diastolic volume and the end-systolic volume is ~70 ml and represents the stroke volume. • Left atrial pressure (LAP) continues to rise because of venous return from the lungs. The peak LAP at the end of this phase is termed the v-wave. Rapid Filling A-V Valves Open • As the ventricles continue to relax, the intraventricular pressures will at some point fall below their respective atrial pressures. When this occurs, the AV valves rapidly open and ventricular filling begins. • Despite the inflow of blood from the atria, intraventricular pressure continues to briefly fall because the ventricles are still undergoing relaxation. Once the ventricles are completely relaxed, their pressures will slowly rise as they fill with blood from the atria. • The opening of the mitral valve causes a rapid fall in LAP. The peak of the LAP just before the valve opens is the "v-wave." This is followed by the y-descent of the LAP. A similar wave and descent are found in the right atrium and in the jugular vein. Reduced Filling A-V Valves open • As the ventricles continue to fill with blood and expand, they become less compliant and the intraventricular pressures rise. This reduces the pressure gradient across the AV valves so that the rate of filling falls. • In normal, resting hearts, the ventricle is about 90% filled by the end of this phase. In other words, about 90% of ventricular filling occurs before atrial contraction. • Aortic pressure and pulmonary arterial pressures continue to fall during this period. Cardiac Cycle LV Pressure-Volume Relationship Pressure Volume Loop Cardiac Output • Volume of blood ejected by each ventricle per minute • CO = Stroke Volume, SV X Heart Rate = l/min • Cardiac Index = CO/body surface area = l/min/m2 • Factors Affecting Stroke Volume – Degree of filling of ventricle, Preload – Contractility of myocardium – Resistance against which the ventricle has to work, Afterload Preload • The load on the myocardial muscle just prior to the onset of contraction. • The more a muscle fibre is stretched before being stimulated to contract, the greater its force of contraction. • Limited by internal molecular structure of muscle, that above a critical (optimal) point further lengthening reduces force of contraction. Effect of Preload on PV loop Myocardial Contractility • (Intrinsic) ability of the cardiac muscle fibres to contract. • Independent of the degree of preload and afterload. • Referred as degree of inotropy • +ve inotropic – Sympathetic nervous system – catecholamines • -ve inotropic – Acidosis – Hypoxia – Hypocalcaemia – Drugs – anaesthetics, antiarrhythmic Effect of Inotropy on PV loop Afterload • The impedence to the ejection of blood from the heart into the arterial circulation. • At the end of diastole, venticular muscle starts to contract. • Need to overcome forces that preventing it; – Tension in ventricular wall – Resistance to ejection of blood from ventricle • Approximated as – L vent afterload – resistance by systemic circulation – Systemic Vascular Resistance (SVR) – R vent afterload – resistance by pulmonary circulation – Pulmonary Vascular Resistance (PVR) Effect of Afterload on PV loop Law Of Laplace T = P x r/wt Tension = Pressure x Radius / wall thickness How does Laplace Work? Heart Rate • Heart has an intrinsic pacemaker, the sinoatrial node. ~ discharged around 100 beats/min • Control by autonomic nervous system • Sympathetic stimulation – increase HR +ve chronotropic • Parasympathetic stimulation (Vagus) – decrease HR - -ve chronotropic CO tends to fall when heart rate surpasses 150/min due to inadequate filling time. Too low heart rate, CO also tends to drop due to insufficient heart rate Location Effects Alpha-1 Blood vessels Vasoconstriction Alpha-2 Blood vessels Vasoconstriction Beta-1 Heart Increase heart rate Increase force of contraction Beta-2 Blood vessels Lungs Vasodilatation Bronchodilatation Receptor type Cardiac Reflexes • • • • • • • Baroreceptor reflex Chemoreceptor reflex Bainbridge reflex Bezold jarish reflex Valsalva maneuver Cushings reflex Occulocardiac reflex Baroreceptor Reflex • Stretch receptors in walls of heart and blood vessels • Responsible for maintenance of blood pressure Baroreceptor Reflex ↑ BP ↑ BR in carotid sinus & aortic arch Sinus nerve & Aortic nerve IX & X nerve N. solitarius ↑ vagal tone ↓ HR Chemoreceptor Reflex ↓pO2 ↑ pCO2 & ↓pH ↑ CR in carotid body & aortic arch Sinus nerve & Aortic nerve IX & X nerve ↑ Respiratory centre ↑ ventilatory drive Bainbridge Reflex Venous engorgement of atria & great veins Stimulation of stretch receptors X nerve CVS center medulla ↓ Vagal tone ↑ HR Bezold Jarish Reflex Ischemia Receptors in LV X nerve Reflex bradycardia, Hypotension & coronary artery dilation Valsalva Maneuver • Forced expiration against closed glottis • Increase in intrathoracic pressure ↑ Intrathoracic pressure → ↑CVP → ↓ V.R → ↓ CO &BP → sensed by BR → ↑ HR & contractility • When glottis opens ↑ VR → ↑ contractility → ↑ BP →sensed by BR → ↓ HR & BP Initial Pressure Rise On application of expiratory force, pressure rises inside the chest forcing blood out of the pulmonary circulation into the L atrium. This causes a mild rise in SV. Reduced VR & Compensation Return of systemic blood to the heart is impeded by the pressure inside the chest. The output of the heart is reduced and SV falls. The fall in SV reflexively causes blood vessels to constrict with some rise in pressure. This compensation can be quite marked with pressure returning to near or even above normal, but the cardiac output and blood flow to the body remains low. During this time the PR increases. Pressure Release Return of CO The pressure on the chest is released, allowing the pulmonary vessels and the aorta to re-expand causing a further initial slight fall in SV due to decreased L ventricular return and increased aortic volume, respectively. Venous blood can once more enter the chest and the heart, CO begins to increase. Blood return to the heart is enhanced by the effect of entry of blood which had been dammed back, causing a rapid increase in CO. The SV usually rises above normal before returning to a normal level. With return of BP, the PR returns towards normal. • Clinical Uses of Valsalva Manoeuvre; – Reversion of supraventricular tachycardia – Testing autonomic function – Aid in assessment of some heart murmurs Cushings Reflex ↑ Intracranial pressure Cerebral ischemia ↑ VMC ↑SNS - ↑BP ↑BR ↑CIC ↑Vagal tone reflex bradycardia ↓ HR Occulocardiac Reflex Pressure on eye long & short ciliary nvs ciliary ganglion gasserion ganglia ↑ PNS → BRADYCARDIA Systemic Circulation Physical laws governing blood flow and blood pressure • Flow of blood through out body = pressure gradient within vessels X resistance to flow - Pressure gradient: aortic pressure – central venous pressure - Resistance: -- vessel radius -- vessel length -- blood viscosity Factors promoting total peripheral resistance (TPR) • Total peripheral resistance = TPR -- combined resistance of all vessels -- vasodilation resistance decreases -- vasoconstriction resistance increases Vasculature Arteries and blood pressure • Pressure reservoir • Arterial walls are able to expand and recoil because of the pressure of elastic fibers in the arterial wall • Systolic pressure: maximum pressure occurring during systole • Diastolic pressure: pressure during diastole Capillaries • Allow exchange of gases, nutrients and wastes between blood and tissues • Overall large surface area and low blood flow • Two main types: - continuous capillaries: narrow space between cells permeable to small or lipid soluble molecules - fenestrated capillaries: large pores between cells large molecules can pass Movement of materials across capillary walls • Small molecules and lipid soluble molecules move by diffusion through the cell membrane • Larger molecules, charged molecules must pass through membrane channels, exocytosis or in between 2 cells • Water movement is controlled by the capillary hydrostatic and osmotic pressures Forces controlling water movement • Arterial side of the capillary: – High capillary hydrostatic pressure (BHP), lower capillary osmotic pressure (BOP, due to proteins and other molecules in the blood) Net filtration pressure pushes fluid from the blood toward the tissue (but the proteins remain in the capillary • Venous side of the capillary: - Lower hydrostatic pressure (due to resistance) and higher capillary osmotic pressure Net filtration pressure moves fluid back toward the capillary • Interstitial fluid hydrostatic (IFHP) and osmotic pressures (IFOP) remain overall identical Starling’s Hypothesis • A quote from Starling (1896) "... there must be a balance between the hydrostatic pressure of the blood in the capillaries and the osmotic attraction of the blood for the surrounding fluids. " " ... and whereas capillary pressure determines transudation, the osmotic pressure of the proteids of the serum determines absorption.“ Starling, 1896 • • Starling’s hypothesis - the fluid movement due to filtration across the wall of a capillary is dependent on the balance between the hydrostatic pressure gradient and the oncotic pressure gradient across the capillary. The four Starling’s forces are: – – – – • • hydrostatic pressure in the capillary (Pc) hydrostatic pressure in the interstitium (Pi) oncotic pressure in the capillary (∏ c ) oncotic pressure in the interstitium (∏ i ) The balance of these forces allows calculation of the net driving pressure for filtration. Net Driving Pressure = [ ( Pc - Pi ) - ( ∏c - ∏i ) ] CAPILLARY FILTRATION HYDROSTATIC FORCES OSMOTIC FORCES ONCOTIC PRESSURE Arterial Pressure Venous Pressure Pre-post Capillary Res. Interstitial Fluid Pressure BALANCE STARLING’S HYPOTHESIS Qf = k (Pc + i) - (Pi + p) Albumin Veins • Veins are blood volume reservoir • Due to thinness of vessel wall less resistance to stretch = more compliance Normal distribution of blood volume • Heart • Pulmonary circulation • Systemic circulation Arteries Capillaries Veins 7% 9% 15% 5% 64% Factors influencing venous return • 1- Skeletal muscle pump and valves • 2- Respiratory pump • 3- Blood volume • 4- Venomotor tone Role of The Parts of Circulation Aorta & Large Elastic Arteries Auxillary pump to obtain continuous (though pulsatile) flow throughout the cardiac cycle Muscular Arteries Distribute oxygenated blood to the tissues Arterioles Resistance vessels – determined the systemic vascular resistance & the distribution of the CO Capillaries Exchange vessels – gas, nutrients and waste Veins Capacitance vessels Return blood to the heart Heart & Lung Contain the central blood volume – Pump & Gas exchange function All together Closed circuit with pump-oxygenator designed for distribution & exchange Mean Arterial Pressure And Its Regulation • Regulation of blood flow in arteries - Intrinsic control - Extrinsic control -Neural control -Hormonal control * Control of blood vessel radius * Control of blood volume Regulation of blood flow in arteries • It is important to adjust blood flow to organ needs Flow of blood to particular organ can be regulated by varying resistance to flow (or blood vessel diameter) • Vasoconstriction of blood vessel smooth muscle is controlled both by the ANS and at the local level. • Four factors control arterial flow at the organ level: - change in metabolic activity - changes in blood flow - stretch of arterial smooth muscle - local chemical messengers Autoregulation Definition: Intrinsic ability of an organ to maintain a constant blood flow despite changes in perfusion pressure, independent of any neural or humoral influences Myogenic Mechanism • The myogenic mechanism is how arteries and arterioles react to an increase or decrease of blood pressure to keep the blood flow within the blood vessel constant • The smooth muscle of the blood vessels reacts to the stretching of the muscle by opening ion channels, which cause the muscle to depolarize, leading to muscle contraction. This significantly reduces the volume of blood able to pass through the lumen, which reduces blood flow through the blood vessel. Alternatively when the smooth muscle in the blood vessel relaxes, the ion channels close, resulting in vasodilation of the blood vessel; this increases the rate of flow through the lumen. From: AJP - Heart October 2008 vol. 295 no. 4 H1505-H1513 Metabolic Mechanism • Any intervention that results in an inadequate oxygen (nutrient) supply for the metabolic requirements of the tissues results in the formation of vasodilator substances which increase blood flow to the tissues Metarteriole Precapillary Sphincter Capillary Relaxation of smooth muscle Lack of oxygen? Formation of vasodilators? Combination of both?? Increased Blood Flow Intrinsic control of local arterial blood flow • Change in metabolic activity – Usually linked to CO2 and O2 levels (↑ CO2 vasodilation ↑ blood flow) intrinsic control • Changes in blood flow - decreased blood flow increased metabolic wastes vasodilation • Stretch of arterial wall = myogenic response - Stretch of arterial wall due to increased pressure reflex constriction • Locally secreted chemicals can promote vasoconstriction or most commonly vasodilation - inflammatory chemicals, (nitric oxide, CO2) Extrinsic control of blood pressure • Two ways to control BP: - Neural control - Hormonal control ** Use negative feedback Neural control of BP • Baroreceptors: carotid and aortic sinuses sense the blood pressure in the aortic arch and internal carotid send signal to the vasomotor center in the medulla oblongata • Other information are sent from the hypothalamus, cortex • Neural control of BP • The vasomotor center integrates all these information • The vasomotor sends decision to the ANS center: - Both parasympathetic and sympathetic innervate the S/A node can accelerate or slow down the heart rate - The sympathetic NS innervates the myocardium and the smooth muscle of the arteries and veins promotes vasoconstriction Hormonal control of BP • Hormones can control blood vessel radius and blood volume, stroke volume and heart rate • On a normal basis, blood vessel radius and blood volume are the main factors • If there is a critical loss of pressure, then the effects on HR and SV will be noticeable (due to epinephrine kicking in) • Control of blood vessel radius - Epinephrine - Angiotensin II - Vasopressin (?) • Control of blood volume - Anti-diuretic hormone (vasopressin) - Aldosterone • Control of heart rate and stroke volume - Epinephrine Control of blood vessel radius • Epinephrine: secreted by the adrenal medulla and ANS reflex increase HR, stroke volume and promotes vasoconstriction of most blood vessel smooth muscles. • - • Angiotensin II promotes vasoconstriction - - - Angiotensin II secretion: Decreased flow of filtrate in kidney tubule is sensed by the Juxtaglomerular apparatus (a small organ located in the tubule) secretion of renin Renin activates angiotensinogen, a protein synthesized by the liver and circulating in the blood angiotensin I Angiotensin I is activated by a lung enzyme, AngiotensinActivating Enzyme (ACE), angiotensin II Angiotensin II is a powerful vasoconstricted of blood vessel smooth muscles Control of blood volume • Anti-diuretic hormone = ADH - - Secreted by the posterior pituitary in response to ↑blood osmolarity (often due to dehydration) Promote water reabsorption by the kidney tubules H2O moves back into the blood less urine formed Control of blood volume • Aldosterone: - - Secretion by the adrenal cortex triggered by angiotensin II Promotes sodium reabsorption by the kidney tubules (Na+ moves back into the blood) H2O follows by osmosis Whereas ADH promotes H2O reabsorption only (in response to dehydration), aldosterone promotes reabsorption of both H2O and salt (in response to ↓ BP) Coronary Circulation Coronary Blood flow – 200-250 ml/min @ 5% CO SA node:-59% RCA. 38% LCA AV node:- 90% RCA 10% LCA Distribution Of Coronary Circulation Left Coronary Artery •Ant descending branch. •Right bundle branch. •Left bundle branch. •Ant & post papillary muscle. •Ant lat left ventricle. Circumflex Branch Lateral left ventricle. Right Coronary Artery •SA and AV nodes. •RA and RV •Post interventricular septum. •Inter atrial septum. •Post fascicle of LB Occlusion in the…. • Anterior descending artery: leads V3-5. • Left circumflex artery: leads I and aVI. • Right coronary artery: leads II, III and aVF. Coronary Perfusion • Coronary perfusion is unique in that it is INTERMITTENT rather than continuous • During contraction, intramyocardial pressures approach that of systemic pressures completely occluding the intramyocardial portions of the coronary arteries Coronary Perfusion • Thus, Coronary perfusion pressure is usually determined by the difference between aortic pressure and ventricular pressure and the left ventricle is almost totally perfused entirely during DIASTOLE • As a determinant of myocardial blood flow, arterial diastolic pressure is MORE important than Mean Arterial Pressure (MAP) Coronary Perfusion • Decreases in Aortic pressure or increases in ventricular end-diastolic pressures can reduce coronary perfusion • Increases in heart rate also decrease coronary perfusion because the faster the heart beats, the less time there is for diastole for perfusion to take place Venous Drainage Of The Heart • Coronary sinus:drains the great cardiac vein, middle cardiac vein and the posterior cardiac vein. • Anterior cardiac veins. • Direct:- arterioluminal, arteriosinusoidal and thebasian veins. Cerebral Circulation Arterial supply Posterior Cerebral artery Anterior Cerebral artery Middle Cerebral artery Internal Carotid artery (70% of CBF) Basilar artery Vertebral artery 30% of CBF Cerebral Circulation Circle of Willis Anterior CA Internal CA Middle CA Posterior CA Basilar A Vertebral A Cerebral Artery Areas 1. anterior cerebral 1 2. Middle cerebral 3 2 54 3. Penetrating branches of middle cerebral 4. anterior choroidal 5 5. Posterior cerebral Cerebral Circulation Venous drainage Cerebral Physiology • 2% of BW • 20% of Total body O2 consumption – (60% used for ATP formation) • CMR O2 3-3.8mL /100 gm/min – (50 ml /min in Adult) • 15% 0f CO (750 ml/min@ 50 ml/100g/min) • Glucose consumption 5 mg/100gm/min – (25% of total body consumption/min) • High oxygen consumption but no reserve • Grey matter of cerebral cortex consumes more • Directly proportional to electrical activity – (Hippocampus & cerebellum most sensitive to hypoxic injury) Cerebral Perfusion Pressure • CPP = MAP—ICP (or CVP whichever is greater) – Normally 80 to 100mm Hg • ICP is <10 mmHg so CPP primarily dependent on MAP • Increase in ICP>30 =CPP & CBF compromise • CPP<50 slowing of EEG – 25-40 Flat EEG – CPP <25 result in Irreversible brain death Factors Influencing CBF • • • • Chemical/metabolic Myogenic Rheologic Neurologic Chemical/Metabolic • Cerebral Metabolic Rate – – – – – Arousal Seizure Mental State Anaesthetic Temperature • PaCO2 • PaO2 • Vasoactive drugs – Anaesthetic – Vasodilators – Vasopressors Cerebral Metabolic Rate • Increased neuronal activity results in increased local brain metabolism • Local metabolic factors play a major role in these adjustments in CBF. • CMR is influenced by several phenomena in the neurosurgical environment – functional state of the nervous system – anesthetic agents, temperature Functional State • CMR decreases during sleep and increases during sensory stimulation, mental tasks, or arousal of any cause. • During epileptoid activity, CMR increases may be extreme, whereas CMR may be substantially reduced in coma. Temperature • CMR decreases by 6 - 7 %/ oC of temperature reduction. • However, in contrast to anesthetic agents, temperature reduction beyond that at which EEG suppression first occurs does produce a further decrease in CMR The effect of temperature reduction on the cerebral metabolic rate of oxygen Temperature on CBF 6-7 % decrease /0C FALL IN TEMP. 37-42 0C >42 0C 20 0C CBF & CMRO2 CMRO2 - ISOELECTRICITY Partial Pressure of Carbon Dioxide • CBF varies directly with PaCO2 • The effect is greatest within the range of physiologic PaCO2 variation. • CBF changes 1 to 2 mL/100 g/min for each 1 mm Hg of change in PaCO2around normal PaCO2 values. • This response is attenuated below a Pa CO2 of 25 mm Hg. • The changes in CBF caused by PaCO2 are apparently dependent on pH alterations in the extra cellular fluid of the brain • Note that in contrast to respiratory acidosis, acute systemic metabolic acidosis has little immediate effect on CBF because the blood-brain barrier (BBB) excludes the hydrogen ion from the perivascular space. • Although the CBF changes in response to PaCO2 alteration occur rapidly, they are not sustained. • In spite of the maintenance of an elevated arterial pH, CBF returns to normal over 6 to 8 hours because cerebrospinal fluid (CSF) pH gradually normalizes as a result of the extrusion of bicarbonate. • Acute normalization of PaCO2 results in a significant CSF acidosis (after hypocapnia) or alkalosis (after hypercapnia). • The former results in increased CBF with a concomitant intracranial pressure (ICP) increase that will depend on the prevailing intracranial compliance. The latter conveys the theoretic risk of ischemia. Partial Pressure of Oxygen • Changes in PaO2from 60 - 300 mmHg have little influence on CBF. • When the PaO2is less than 60 mm Hg, CBF increases rapidly . • At high PaO2values, CBF decreases modestly. • The mechanisms mediating the cerebral vasodilation during hypoxia are not fully understood, but they may include neurogenic effects initiated by peripheral and/or neuraxial chemoreceptors as well as local humoral influences • At 1 atm O2,CBF is reduced by 12 percent. Myogenic Regulation Autoregulation refers to the capacity of the cerebral circulation to adjust its resistance in order to maintain CBF constant over a wide range of mean arterial pressure Neurogenic Regulation • There is considerable evidence of extensive innervation of the cerebral vasculature. • The density of innervation declines with vessel size, and the greatest neurogenic influence appears to be exerted on larger cerebral arteries. • This innervation includes autonomic, serotonergic, and vasoactive intestinal peptideergic (VIPergic) systems of extra-axial and intraaxial origin. Viscosity Effects • Blood viscosity can influence CBF. • Hematocrit is the single most important determinant of blood viscosity. • In healthy subjects, hematocrit variation within the normal range (33-45%) probably results in only trivial alteration of CBF. • Beyond this range, changes are more substantial. "a Systems Approach for PHysiological Integration of Renal, cardiac, and respiratory functions" oxygen delivery muscles thirst kidney ADH control local blood flow control autonomic control heart rate… capillary membrane dynamics circulatory dynamics angiotensin control aldosterone control tissue fluids, pressures, gel pulmonary red cells, dynamics viscosity heart hypertrophy electrolytes & cell water Guyton, Coleman, Granger (1972) Ann. Rev. Physiol. Guyton's modular Systems Model for blood pressure regulation Good Luck