NURSING CARE PREPARATION
advertisement

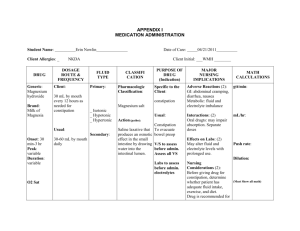
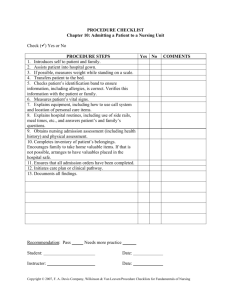
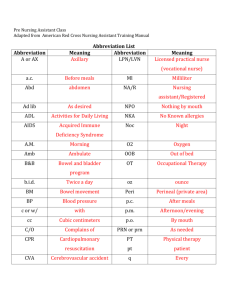
NURSING 110 CARE PREPARATION Student Name: Stephanie Perkins Unit/Room Number: 214 Age: 31 Gender: Female Erikson’s Developmental Level: Intimacy vs. Isolation Date of Care: 1/15/15 Date of Admission: 1/14/15 Ethnic/Cultural Preferences: Allergies: Latex Code Status: Full Primary Diagnosis: Large gestational age caesarian Co-morbidities: Obesity, previous caesarian Discharge Plan (add day of clinical): Go home with baby to father and babies siblings Pathophysiology (explain in 250 words or less your clients primary diagnosis) A caesarian is the surgical procedure of delivering a baby. The reason for this caesarian was due to the baby being a large gestational age. Data Collection (Record exactly what is written on the personal information sheet [aka Kardex]. Any assessment/elaboration should be made on the assessment sheet): Diet (Type): Regular I&O (MD order/Nursing Order/Frequency): Daily Fall Risk/Safety Precautions (Yes/No): yes due to post op Wound Care (Yes/No): yes Drains (Yes/No, Type): no Other Tubes: IV (Fluid type, rate, access type): no CBG (Yes/No, frequency): no Activity (What is ordered): assist first time, up ad lib Oxygen (Yes/No, Delivery method, how much): no Last BM: 1/14/15 am hard ASSESSMENTS (Include Subjective & Objective Data) Integumentary: O: Appropriate for race, warm, dry, incision above pubic symphysis from caesarian with dressing over it. No areas of redness. Scar on left shin approximately 5 ½ inches long. Head and Neck: O: Normocephalic, hair clean and pulled back, conjunctivae pink and moist sclera white, PERRLA 2. Full ROM in tact. S: “My neck is a little stiff from lying in bed” S: “It’s from first grade. Cut it on glass. Never got stitches.” Ear/Nose/Throat: O: Ears intact, cecum visible in L ear. No complaints of drainage or congestion of nose. Nares patent able to distinguish smells. Mucous membranes intact pink and moist. Teeth and tongue intact. Able to swallow and say “ah”. Thorax/Lungs: Lung sounds clear throughout. No tactile fremitus. Respirations easy and regular bilaterally. S: S: Cardiac: No reports of chest pain, S1 and S2 heard, no edema present cap refill less than 2 sec, no clubbing. S: Musculoskeletal: Pain of 2/10 grips strong full ROM except ability to bend at waist is altered due to surgery. Wears scuds when in bed. Ambulates to bathroom independently. Ambulated down hallway to nursery and back without assistance or complaints of SOB. S: Genitourinary: O: Voiding independently, yellow, no odor. Blood present voided 325 ml Gastrointestinal: Obese, last BM 1/14/15 in am abdomen distended from fundus, fundus at -1 from umbilicus, firm. S: S: Pt winced with fundus massage Neurological: A/O x 3 GCS 15 S: Other (Include vital signs, weight): BP: 94/62 HR: 83 RR: 16 O2: 97 T: 98 Pain: 2/10 CURRENT MEDICATIONS List ALL regularly scheduled and prn medications scheduled on your client. (Due morning of clinical) Generic & Trade Name Classification Dose/Route/ Rate if IV Onset/Peak Intended Action/Therapeutic use. Why is this client taking med? Adverse reactions (1 major side effect) Nursing Implications for this client. (No more than one) Docusate Sodium (Colace) Stool Softener 100 mg Po BID Unknown Prevent constipation Diarrhea Assess abdomen Ferrous Gluconate (Ferate) Iron Preparatio n 324 mg PO daily Unknown Treat iron deficiency Black stool Assess RBC count Ibuprofen (motrin) Analgesic 600 mg PO q6h 1h/ 1-2 h Relief mild to moderate pain Nausea Assess pain level Bisacodyl (dulcolax) Stimulant Laxative 6-8 h/unknown Temp relief of acute constipation Mild cramping Assess abdomen Diphenhydr amine (Benadryl) Antihistam ine 10 mg 1 supp rectal prn 25 mg PO q8h prn itching 15-30 min/1-4 h Temp relief various allergic reactions Drowsiness Assess for allergy relief Hydrocodon e/APAP (Norco) Analgesic 10-20 min/3-6 h Relief of moderate to severe pain Constipation Assess abdomen Hydrocodon e/APAP (Norco) Analgesic 10/325 1 tab PO q4h prn moderate pain 10/325 2 tab PO q4h prn moderate pain 10-20 min/36 h Relief of moderate to severe pain Constipation Assess pain Magnesium Hydroxide (milk of Mag) Laxative 30 ml PO HS PRN constipation Unknown Short term treatment of constipation Diarrhea Assess for diarrhea Methylergo novine (Methergin e) Oxytocic 0.2 mg PO q6h prn heavy bleeding max 3 doses 5-15 m/ unknown Control bleeding Drowsiness Assess bleeding DIAGNOSTIC TESTING Include pertinent labs [ABGs, INRs, cultures, etc] & other diagnostic reports [X-rays, CT, MRI, U/S, etc.] NOTE: Adult values indicated. If client is newborn or elder, normal value range may be different. Date Lab Test Normal Values Sodium 135 – 145 mEq/L Potassium 3.5 – 5.0 mEq/L Chloride 97-107 mEq/L Co2 23-29 mEq/L Glucose 75 – 110 mg/dL BUN 8-21 mg/dL Creatinine 0.5 – 1.2 mg/dL Uric Acid Plasma 4.4-7.6 mg/dL Calcium 8.2-10.2 mg/dL Phosphorus 2.5-4.5 mg/dL Total Bilirubin 0.3-1.2 mg/dL Total Protein 6.0-8.0 gm/dL Albumin 3.4-4.8gm/dL Cholesterol <200-240 mg/dL Alk Phos 25-142 IU/L SGOT or AST 10 – 48 IU/L LDH 70-185 IU/L CPK 38-174 IU/L WBC 4.5 – 11.0 RBC male: 4.7-5.14 x 10 female: 4.2-4.87 x 10 HGB male: 12.6-17.4 g/dL female: 11.7-16.1 g/dL HCT male: 43-49% female: 38-44% MCV 85-95 fL MCH 28 – 32 Pg MCHC 33-35 g/dL RDW 11.6-14.8% Platelet 150-450 Patient Values/ Date of care 8.2 4.55 13.1 39.5 87 28.8 33.2 13.5 153 Interpretation as related to Pathophysiology –cite reference & pg # DIAGNOSTIC TESTING Date UA Normal Range Results Interpretation as related to Pathophysiology –cite reference & pg # Results Interpretation as related to Pathophysiology –cite reference & pg # Color/Appearance pH Spec Gravity Protein Glucose Ketones Blood Date Other (PT, PTT, INR, ABG’s, Cultures, etc) Date Radiology X-Rays Scans EKG-12 lead Telemetry Normal Range Results Interpretation as related to Pathophysiology –cite reference & pg # DAR NURSING PROGRESS NOTE Include the same note that was written in the client record for the priority nursing diagnostic statement. Include the date/time/signature. 1/15/15 0745 Assumed care A/O x 3 awake and watching TV ate breakfast. Postop caesarian 1/14/15. Massaged fundus. -1 umbilicus. Winced in pain taught breathing technique of blowing out while massaging. Pain meds given see MAR (Ling RN gave meds). Left patient breastfeeding daughter. Scuds on properly call light and water within reach. -------------------------------------------------------------------------------------------------------------Stephanie Perkins SN PATIENT CARE PLAN Patient Information: Nursing Diagnosis should include Nanda Nursing Diagnostic statement, related to (R/T), as evidenced by (AEB). Problem #1 Acute Pain r/t incision site AEB surgical procedure Desired Outcome: Pain will be at or below a 5 on a scale of 0-10 during shift Nursing Interventions Client Response to Intervention 1. Assess pain level every hourly round 1. Stated pain was a 2/10 2. Give ibuprofen or hydrocodone when appropriate 2. Ling RN gave patient ibuprofen 3. Teach relaxation techniques 3. Demonstrated proper breathing out when massaging the fundus Evaluation (evaluate goal & interventions, what worked/what didn’t, what would you adapt if needed): I was surprised at how little pain this patient was in considering she had a c section yesterday. She did wince when we first started massaging the fundus, but she used good breathing techniques and it seemed to help. Problem #2 Risk for Injury (DVT) r/t abnormal clotting AEB surgical procedure Desired Outcome: Patient will no present with a blood clot during shift Nursing Interventions Client Response to Intervention 1. Assess LE for edema 1. No edema present 2. Use scuds properly when in bed 2. Scuds were used whenever in bed 3. Reinforce importance of ambulation postop 3. Patient ambulated down hall and to nursery and back without complaint of pain or SOB Evaluation: I think this goal worked really well with this patient. She was motivated to get up and moving. She was able to walk to the shower room and clean up as well as to the nursery and back. By the end of the shift she was ambulating independently. Problem #3 Activity Intolerance r/t surgical procedure AEB hospitalization Desired Outcome: Pt will ambulate 50 ft by end of shift Nursing Interventions Client Response to Intervention 1. Assess for pain every hourly round 1. Pt reported 2/10 2. Encourage use of assistive device if necessary for ambulation 2. Assistive device not needed 3. Teach about regulation of energy to prevent fatigue 3. unable Evaluation: Again, I was very surprised at how quickly this pt was able to get back to walking around without assistance. She was very motivated, however, and I think setting these goals only added fuel to that fire.