Cardioversion Curriculum
advertisement

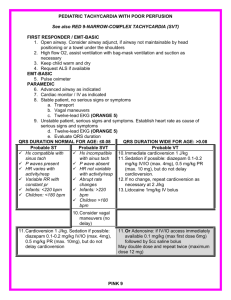
Cardioversion Curriculum Learning Objectives At the conclusion of this activity, the learner will be able to: • Identify appropriate anticoagulation strategies prior to and following cardioversion. • Provide anticoagulation therapy for the appropriate period before and after cardioversion. • Determine appropriate antiarrhythmic drug therapy to restore sinus rhythm in patients who have AF of greater than or less than 7 days. • Administer antiarrhythmic drug therapy to prevent ERAF after cardioversion. • Recognize that administration of antiarrythmic medication prior to cardioversion may promote restoration of sinus rhythm and the implications with respect to thromboembolism. • Recognize the different methods of cardioversion as well as both preand post-procedure anticoagulation strategies and anti-arrhythmic drug management. www.HRSonline.org Candidates for Elective Cardioversion • Patients with a reasonable expectation to remain in sinus rhythm • Patients with substantial symptoms in AF with good rate control • Patients in whom the physician considers sinus rhythm the preferred treatment strategy www.HRSonline.org Special Considerations for Anticoagulation Prior to Cardioversion • For patients with AF > 48 hours of AF, or when duration is unknown, 3 weeks of anticoagulation are required prior to cardioversion. • Documentation of anticoagulation adequacy is important prior to cardioversion • It may take longer than 3 weeks to achieve 3 consecutive weeks of adequate anticoagulation • Anticoagulation must be continued for at least 4 weeks post cardioversion • TEE can be used to assess LA for thrombus as alternative to 3-week anticoagulation (however, anti-coagulation must continue for 4 weeks post cardioversion Fuster et al. J Amer Coll Cardiol 2006; 48: 854-906 www.HRSonline.org Prospective Companion of TEE-guided vs. Conventional-treatment Cardioversion of A. Fib Klein AL, N Engl J Med 2001; 344: 1411-20 Atrial fibrillation > 2 days’ duration, DC cardioversion prescribed Random assignment (1:1) Transesophagealechocardiography group Conventional treatment group Therapeutic anticoagulation with heparin or warfarin Thrombus detected No DC cardioversion No thrombus detected DC cardioversion Warfarin for 3 wk Warfarin for 3 wk Repeated transesophageal echocardiography No thrombus DC cardioversion Thrombus No DC cardioversion Warfarin for 4 wk Warfarin for 4 wk Warfarin for 4 wk Warfarin for 4 wk Follow-up examination 8 wk after assignment www.HRSonline.org DC cardioversion Clinical Outcomes of TEE-guided vs. Conventional-treatment Cardioversion of A. Fib Variable TEE Guided (n= 619) Conventional Treatment (n=603) 80.3 79.9 Time to Cardioversion (d) 3.0 + 5.6* 30.6 + 10.6 Embolic Events (%) 5 (0.8%) 3 (0.5%) Hemorrhagic events (%) 18 (2.9%)* 33 (5.5%) Death (%) 15 (2.4%) 6 (1.0%) 52.7 50.4 Successful Cardioversion (%) SR at 8 wks (%) *significant Klein AL, N Engl J Med 2001; 344: 1411-20 6 www.HRSonline.org Daily Incidence of AF Relapse After Electrical Cardioversion Number of patients with relapse of AF 6 5 4 3 2 1 0 0 5 10 20 Days post cardioversion Tieleman RG et al. J Am Coll Cardiol 1998; 31: 167-73 www.HRSonline.org 15 25 30 35 Procedural Aspects of Direct-current Cardioversion of Atrial Fibrillation • Ensure appropriate anticoagulation • Use adequate general anesthesia in fasting state • Electrodes positioned anterior-posterior or anterior-lateral • Confirm R-wave synchronization • Biphasic shock waveform preferable • Determine the need for pretreatment with antiarrhythmic drugs www.HRSonline.org Proportion, with 95% Confidence Interval Cumulative Success in Cardioversion of A. Fib: Biphasic vs. Monophasic Waveform 1.0 Biphasic 0.8 * Monophasic * * 0.6 0.4 0.2 0.0 1st Shock www.HRSonline.org 1-2 Shocks 1-3 Shocks Page RL et al. J Am Coll Cardiol 2002; 39: 1956-63 1-4 Shocks www.HRSonline.org www.HRSonline.org Recommendations for Direct-current Cardioversion of Atrial Fibrillation Class I 1. When a rapid ventricular response does not respond promptly to pharmacological measures for patients with AF with ongoing myocardial ischemia, symptomatic hypotension, angina, or HF, immediate R-wave synchronized direct-current cardioversion is recommended. (Level of Evidence: C) 2. Immediate direct-current cardioversion is recommended for patient with AF involving preexcitation when very rapid tachycardia or hemodynamic instability occurs. (Level of Evidence: B) 3. Cardioversion is recommended in patients without hemodynamic instability when symptoms of AF are unacceptable to the patient. In case of early relapse of AF after cardioversion, repeated direct-current cardioversion, repeated direct-current cardioversion attempts may be made following administration of antiarrhythmic medication. (Level of Evidence: C) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Recommendations for Direct-current Cardioversion of Atrial Fibrillation Class IIa 1. Direct-current cardioversion can be useful to restore sinus rhythm as part of a long-term management strategy for patients with AF. (Level of Evidence: B) 2. Patient preference is a reasonable consideration in the selection of infrequently repeated cardioversions for the management of symptomatic or recurrent AF. (Level of Evidence: C) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Recommendations for Direct-current Cardioversion of Atrial Fibrillation Class III 1. Frequent repetition of direct-current cardioversion is not recommended for patients who have relatively short periods of sinus rhythm between relapses of AF after multiple cardioversion procedures despite prophylactic antiarrhythmic drug therapy. (Level of Evidence: C) 2. Electrical cardioversion is contraindicated in patients with digitalis toxicity or hypokalemia. (Level of Evidence: C) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Pharmacological Cardioversion of Atrial Fibrillation < 7 days Duration Drug Class of Recommendation (level of evidence) Agents with proven efficacy Dofetilide I (A) Flecainide I (A) Ibutilide I (A) Propafenone I (A) Amiodarone IIa (A) Less effective or incompletely studied Disopyramide IIb (B) Procainamide IIb (B) Quinidine IIb (B) Should not be administered Digoxin III (A) Sotalol III (A) Modified from: ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 15 www.HRSonline.org Successful Conversion Rate of Atrial Fibrillation and Flutter with Intravenous Ibutilide vs. Procainamide 100 Ibutilide ** Success rate (%) 80 60 * Procainamide *** 40 20 0 Combined Volgman AS et al. J Am Coll Cardiol 1998; 31: 1414-19 www.HRSonline.org Flutter Fibrillation Success Rates of Conversion to Sinus Rhythm with Vernakalant Compared with Placebo P<0.001 60 Vernakalant Placebo 51.7 50 Percentage P<0.001 37.6 40 30 20 P=0.09 7.9 10 4.0 2.6 0 0 (n=75) (n=145) Short-Duration AF Roy D Circulation 2008; 117:1518-1525 www.HRSonline.org (n=40) (n=76) Long-duration AF (n=115) (n=221) Overall Population Cumulative Success Rates of Conversion to Sinus Rhythm Over Time with Vernakalant vs. Placebo Proportion of Patients with Conversion to SR 0.6 Vernakalant Placebo 0.5 0.4 P<.001 (Log-Rank Test) 0.3 0.2 0.1 0 20 40 60 80 0 100 Time from First Infusion of Study Drug (min.) Roy D Circulation 2008; 117:1518-1525 www.HRSonline.org Pharmacological Cardioversion of Atrial Fibrillation > 7 days Duration Drug Class of Recommendation (level of evidence) Agents with proven efficacy Dofetilide I (A) Amiodarone IIa (A) Ibutilide IIa (A) Less effective or incompletely studied Disopyramide IIb (B) Flecainide IIb (B) Procainamide IIb (B) Propafenone IIb (B) Quinidine IIb (B) Should not be administered Digoxin III (B) Sotalol III (B) Modified from: ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 19 www.HRSonline.org Outpatient Treatment of Recent-onset Atrial Fibrillation with the “Pill-in-the-Pocket” Approach • 268 consecutive patients with recent-onset (< 48 hours) A. Fib with mean heart rate > 70/min and systolic BP > 100mmHg • Patients treated in emergency room or cardiology ward • Some exclusions: • Preexcitaiton; BB block; IHD; DCM; HCM; • History of HF; prev AF > 7 days duration • Single oral AA drug dose: • Flecainide 300mg (>70kg); 200mg (<70kg) • Propafenone 600mg (>70kg); 450mg (<70kg) • 58 (22%) patients excluded because of treatment failures or side effects (n=14) • hypotension (n=4); symptomatic bradycardia (n=3); transient A Fl (n=7) Alboni P et al. N Engl J Med 2004; 351: 2384-91 www.HRSonline.org “Pill-in-the-Pocket” Approach to Cardiovert A. Fib Alboni P et al. N Engl J Med 2004; 351: 2384-91 268 patients treated in hospital 58 patients excluded - 3 patients (1%) met echocardiographic exclusion criteria - 41 patients (15%) had drug inefficacy - 14 patients (5%) had adverse effects 210 patients enrolled for out-of-hospital treatment 4 patients (2%) lost to follow-up 41 patients (20%) had no recurrence www.HRSonline.org 165 patients (79%) had recurrences “Pill-in-the-Pocket” Approach to Cardiovert A. Fib 165 patients (79%) had recurrences 618 arrhythmic episodes 49 untreated episodes (8%) 569 treated episodes (92%) 5 episodes (10%) involved 534 episodes (94%) interrupted < 6 hr ER contact 16 episodes (3%) interrupted > 6hr; did not contact ER 26 episodes (5%) involved ER contact Alboni P et al. N Engl J Med 2004; 351: 2384-91 Total of 31 episodes (5% involved ER contact www.HRSonline.org Recommendations for Pharmacological Cardioversion of Atrial Fibrillation Class I • Administration of flecainide, dofetilide, propafenone, or ibutilide is recommended for pharmacological cardioversion of AF. (Level of Evidence: A) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Recommendations for Pharmacological Cardioversion of Atrial Fibrillation Class IIa 1. Administration of amiodarone is a reasonable option for pharmacological cardioversion of AF. (Level of Evidence: A) 2. A single oral bonus dose of propafenone or flecainide (“pill-in-thepocket”) can be administered to terminate persistent AF outside the hospital once treatment has proved safe in a hospital for selected patients without sinus or AV node dysfunction, bundle-branch block,QT-interval prolongation, the Brugada syndrome, or structural heart disease. Before antiarrhythmic medication is initiated, a beta blocker or nondihydropyridine calcium channel antagonist should be given to prevent rapid AV conduction in the event atrial flutter occurs. (Level of Evidence: C) 3. Administration of amiodarone can be beneficial on an outpatient basis in patients with paroxysmal or persistent AF when rapid restoration of sinus rhythm is not deemed necessary. (Level of Evidence: C) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Recommendations for Pharmacological Cardioversion of Atrial Fibrillation Class IIb • Administration of quinidine or procainamide might be considered for pharmacological cardioversion of AF, but the usefulness of these agents is not well established. (Level of Evidence: C) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org Recommendations for Pharmacological Cardioversion of Atrial Fibrillation Class III 1. Digoxin and sotalol may be harmful when used for pharmacological cardioversion of AF and are not recommended. (Level of Evidence: A) 2. Quinidine, procainamide, disopyramide, and dofetilide should not be started out of hospital for conversion of AF to sinus rhythm. (Level of Evidence: B) ACC/AHA/ESC Practice Guidelines, Fuster et al. JACC 2006; 48: e149-246 www.HRSonline.org