Ventilatory and Blood Gas Response to Exercise
advertisement

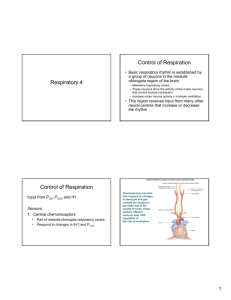
Ventilatory and Blood Gas Response to Exercise Rest to work Transitions • Change in pulmonary ventilation • Observed below lactate threshold Rest to work Transitions • Transition from rest constant-load-submaximal exercise • Arterial tensions of PCO2 and PO2 are relatively unchanged during transition during submaximal exercise • BUT: arterial PO2 decreases & PCO2 increases slight in transition from rest steady-state exercise • Therefore: at the start of exercise: Increase in ventilation is NOT as fast as increase in metabolism Rest to work transitions • At the onset of constant-load submaximal exercise: – Initially, ventilation increases rapidly • Then, a slower rise toward steady-state – PO2 and PCO2 are maintained • Slight decrease in PO2 and increase in PCO2 Changes in Ventilation, PO2 and PCO2 in transition from rest to steady state submaximal exercise Prolonged Exercise in a hot Environment • Cool, low humidity environment = 19°C, 45% humidity • Hot, high humidity = from 28°C, 75% humidity • Hot environments hamper heat loss from the body • Increase in body temperature which directly affects respiratory control centre = Minute ventilation increases (with increased breathing frequency) Prolonged Exercise in a hot Environment During prolonged sub maximal exercise: • Ventilation tends to drift upwards • Little change in PCO2 • Higher ventilation not due to increased PCO2 Incremental Exercise • Linear increase in ventilation - Up to 50 – 75% VO2max • Exponential increase beyond this point • Ventilatory threshold - Point where minute ventilation increases exponentially Ventilatory Threshold • Reflects aerobic fitness without the need to directly measure maximal oxygen uptake • Point during exercise training at which pulmonary ventilation becomes disproportionately high with respect to oxygen consumption during an incremental exercise test • Used as a guide to determine exercise intensity • Therefore: Ventilatory threshold = intensity of exercise that shows a larger ventilation than required to do work. • At this point, the contribution of anaerobic metabolism becomes significant to produce larger concentrations of lactic acid. • Lactic acid accumulates, reducing pH & increasing metabolic acidosis. • Because one of the functions of the respiratory system is acid-base balance, respiration must increase to compensate for the increased acidosis. • The point were ventilation deviates from linearity is termed the ventilatory threshold (TVENT). Ventilatory response to exercise Trained vs. Untrained: • - Trained: Decrease in arterial PO2 near exhaustion pH maintained at a higher work rate Ventilatory threshold occurs at higher work rate Effect of Training on Ventilation • Untrained: able to maintain PO2 in arteries within 10– 12 mmHg of resting value • Trained: PO2 decreases by 30- 40 mmHg during heavy exercise *low arterial PO2 vales during exercise = exercise induced hypoxemia * Low arterial Po2 values are also seen in patients with severe lung disease Males Vs. Female athletes • 50% of highly trained male endurance athletes develop exercise induced hypoxemia • Females are suggested to have experience exercise induced hypoxemia more often than males Causes • Failure of pulmonary system? • Ventilation perfusion mismatch? Indicates matching of blood flow to ventilation – Ideal: ~1.0 – Light exercise improves – Heavy exercise = inequality • Diffusion limitations during exercise ? Reduced amount of time that red blood cells spend in the pulmonary capillaries...caused by high cardiac outputs from athletes less time for gas equilibrium to be achieved Ventilatory Response to exercise: Trained Vs. Untrained Revision questions 1. 2. 3. 4. 5. 6. 7. 8. Describe the changes in PO2 and PCO2 with different exercises. What happens during prolonged sub maximal exercise? Why does this occur? What happens during incremental exercise? Explain the Ventilatory Threshold How do trained and untrained athlete’s ventilatory responses differ? How do male and female ventilatory responses differ? What is hypoxemia and how does it relate to exercise? What are the suggested causes to hypoxemia in athletes? (6) (6) (3) (8) (6) (2) (4) (6)