Childhood Urinary Tract Infection (UTI)
advertisement
")
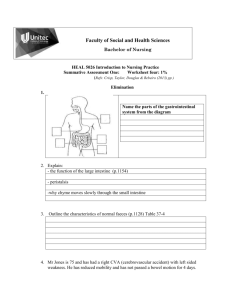
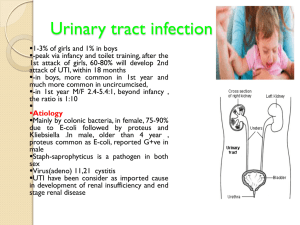
Childhood Urinary Tract Infection Definition and classification It is an infection of both upper and lower urinary tract. Upper : pyelonephritis, renal abscess. Lower : cystitis , urethritis Epidemiology UTI is one of the most common bacterial infections of childhood. Affects up to 10% by the teenage years. Before age of 1 year boys : girls = 3 : 1 After age of 1 year girls : boys = 10 : 1 40% of children with UTI will have anatomic or functional abnormalities of the urinary tract. e.g. reflux, malpositions, duplications, megaureter and hydronephrosis. Etiology Source of infection: Mostly ascending. The bacteria arise from the fecal flora, colonize the perineum, and enter the bladder via the urethra In neonates ……………… HEMATOGENEUS. Etiological organisms: Escherichia coli: (80%), Klebsiella and Proteus. Staphylococcus saprophyticus in adolesent girls. Viral infections (adenovirus), can cause cystitis. Fungal infections Risk Factors Type of patient: -Female )short urethra) -Uncircumcised male. -Tight clothing. -Urethral instrumentation Abnormal Urinary tract: -Vesicoureteral reflux. -Obstructive uropathy (major risk factor): Hydronephrosis -Neurogenic bladder Clinical Manifestations Pyelonephritis Constitutional symptoms: Fever, malaise, chills. Nausea, vomiting ± diarrhea. Localizing symptoms: Abdominal or flank pain. Clinical Manifestations (cont) Cystitis Usually afebrile Dysurea Urgency Frequency Incontinence Hematuria Malodorous urine. Suprapubic pain & tenderness. Clinical Manifestations (cont) Urethritis -Dysurea -Reluctance to void -Perineal discomfort, erythema -Vulval irritation & erythema (girls) -Urethral discharge in older boys Symptoms of UTI Neonates & infants Change in urine color (or odor) as well as, crying during micturation in an infant may be noted by the mother. BUT Nonspecific symptoms: Jaundice Poor feeding Irritability Weight loss (or poor weight gain) Asymptomatic bacteriurea Refers to individuals who have a positive urine culture without any manifestations of infection. Occurs almost exclusively in girls. This condition is benign and does not cause renal injury. Complications recurrance ( up to 25% to 40% )( follow up) bacteremia (more in infants) focal renal abscess ( uncommon ) cont. Acute pyelonephritis may result in renal injury “pyelonephritic scarring” Hypertension If recurrent scarring Chronic renal failure Diagnosis of UTI Diagnosis of UTI Suspect: Symptoms Findings on urinalysis, or both. Confirm: Urine culture. The diagnosis of UTI depends on having the proper sample of urine Urine analysis Urine microscopy: Pus cells White cell cast ……… RBCs …….. Gram staining Urine dipstick: - Leucocyte estrase - Nitrite Collecting the urine sample Collecting the urine sample In toilet-trained children midstream urine sample Satisfactory if The culture shows greater than 100,000 colonies of a single pathogen. There are 10,000 colonies and the child is symptomatic, it is considered a UTI. Collecting the urine sample (cont): In infants: (1) Clean catch sample. (2) Urine collection bag. contamination is possible (3) In & out urinary catheterization. (4) Suprapubic urine sample Notes about urine analysis & culture: Prompt plating of the urine sample is important - not more than one hour. A urinalysis should be obtained from the same specimen as that cultured. Pyuria (leukocytes in the urine) suggests infection, but infection can occur in the absence of pyuria. Treatment of UTI Treatment In acute febrile infections suggestive of pyelonephritis: Parenteral treatment with ceftriaxone or ampicillin with gentamicin for 10-14 days. Treatment of UTI (cont): Acute cystitis: Should be treated promptly to prevent its possible progression to pyelonephritis. trimethoprim-sulfamethoxazole . Nitrofurantoin Amoxicillin for 3-5 days If the symptoms are mild and the diagnosis is doubtful, treatment can be delayed until the results of culture are known, and the culture can be repeated if the results are uncertain FOLLOW UP We usually do urine culture 1 week after stopping of antibiotics ; then periodic reassessment for the next 1-2 years . Imaging Studies The goal of imaging studies in children with a UTI The goal of imaging studies in children with a UTI is to identify anatomic abnormalities that predispose to infection and to If there are any UTI complications Renal ultrasonogram Renal ultrasonogram - - hydronephrosis renal or perirenal abscesses Pyelonephritis renal scars ( 30%) VCUG( MCUG) Voiding cystourethrogram (VCUG) Miturating cystourethrogram (MCUG) Indications: All children younger than 5 yr with a UTI, School-aged girls who have had two or more UTIs Any male with a UTI The most common finding is vesicoureteric reflux DMSA scan & DTPA scan DMSA scan: Technetium-labeled Acute pyelonephritis Structural malformations of the kidney DTPA scan: Dynamic study for: Excretory Function Reflux DETPA Prevention of reccurrence of UTI Prevention of reccurrence of UTI Aderss and treat underlying cause. Manage constipation. Correct bottom wiping. Encourage drinking adequate fluid. Advice child not to delay voiding. Use of prophylactic antibiotics ………….. THANK YOU