ECMO * Extra coporeal membrane oxygenation
advertisement

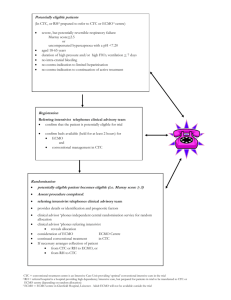
ECMO – Extracorporeal membrane oxygenation Support in critically ill adult patients – is its use evidence driven? A META-ANALYSIS SILVAARIANA | MORAISCATARINA | PEREIRADIOGO | SILVAEUNICE | ROCHAHENRIQUE | SILVAJOÃO |JARDIMMÓNICA | SANTOSPEDRO | MARTINSRITA | LOPESRUI | CLASS9 Adviser: Prof. Sandra Filipa Canário Almeida Introdução à Medicina II 2010/2011 In what circumstances can ECMO be used ? Introduction Aims Heart failure Respiratory insufficiency Heart failure Heart failure Critical ill patients Respiratory insufficiency Methods > Heterogenous condition in which the > Individuals Heterogenous condition ofin Inadequate supply of sufficient oxygen heart is unablewhose to pump state out blood to the meet the metabolic needs which heart unable toof disease may eminent to the cells oflead theisto body, and Critically ill patient the body1. pump out blood to death .insufficiency removal ofsufficient carbon dioxide . Respiratory 3 Inexistance of other forms of treatment which are likely to be successful Results Conclusions 2 > Inadequate of oxygen to the of cells meet thesupply metabolic needs of the body, and removal of carbon 1. body 2 Acknowledgements References the . dioxide Critical ill patients > Individuals whose state of disease may ECMO lead to eminent death3. 1 MeSH Browser [Internet]. MeSH Unique ID: D006333. MeSH Browser [Internet]. MeSH Unique ID: D012131. 3 MeSH Browser [Internet]. MeSH Unique ID: D016638. 2 Diagram 1 ECMO’s application. 2 ECMO and its importance Introduction > Technique used to provide life support to the critically ill; Aims > Temporary support for patients with pulmonary or Methods cardiac failure (or both), when no other form of Results treatment is likely to be successful [1]; Conclusions > Expensive therapy, requiring the weighing of its application, instead of other forms of treatment [1]. Acknowledgements Fig. 1: ECMO system. References Are there any positive outcomes of this treatment in critical ill adult patients? [1] Marasco SF. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008; 3 Past records Introduction > Mechanical circulatory support has evolved markedly since the first successful application of the heart–lung machine in 1953 [2]; Aims > First successful implantation of ECMO , by Robert Bartlett , dates from 1972 Methods [3]; Results > Used commonly at several specialized hospitals for the treatment of infants Conclusions and, less frequently, for adults with respiratory or cardiac failure [3]; > Its use in adults remained controversial for some time, due to lower survival Acknowledgements rates [4]. References Studies stating satisfactory results in critically ill adults have been published recently. 4 [2] Lindstrom SJ. Extracorporeal membrane oxygenation. Med J Aust. 2009; [3] Schmid C. Extracorporeal life support - systems, indications, and limitations. Thorac Cardiovasc Surg. 2009; [4] Sidebotham D. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory disease in adults: Part 1-overview of extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009; Modalities of ECMO Venoarterial ECMO Introduction Aims > Blood is drawn from the venous system, oxygenated and pumped into Methods the arterial circulation; Results > Provides partial or complete support Conclusions of heart, and allows the oxygenation of blood [3]. Acknowledgements References Fig. 2 Venoarterial ECMO system. Diagram 2 Venoarterial ECMO system. [3] Schmid C. Extracorporeal life support - systems, indications, and limitations. Thorac Cardiovasc Surg. 2009. 5 Modalities of ECMO Venovenous ECMO Introduction Aims > Blood is drained and returned to venous system, providing complete or Methods partial support of the lungs, as long as Results the cardiac output is sufficient; Conclusions > Diseased lungs may heal while the potential additional injury of aggressive Acknowledgements mechanical ventilation is avoided [3]. References Fig. 3 Venovenous ECMO system. Diagram 3 Venovenous ECMO system. [3] Schmid C. Extracorporeal life support - systems, indications, and limitations. Thorac Cardiovasc Surg. 2009. 6 Coronary artery bypass graft surgery and valve replacement [4]; Post-cardiotomy and primary graft failure after heart transplant [5]. Severe cardiac failure (e.g. myocarditis, decompensated cardiomyopathy, acute coronary syndrome with cardiogenic shock, sepsis, drug related) [1], [4]; Severe trauma with coexisting bleeding shock [6]. Introduction Less Recommended* Bridge for patients with end-stage heart failure to heart transplant [3]; More Recommended* Cardiac indications Indications for the use of ECMO Conclusions Aims Methods Results Acknowledgements References * In published literature [1] Marasco SF. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008; [3] Schmid C. Extracorporeal life support - systems, indications, and limitations. Thorac Cardiovasc Surg. 2009; [4] Sidebotham D. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory disease in adults: Part 1--overview of extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009; [5] Fiser SM. When to discontinue extracorporeal membrane oxygenation for postcardiotomy support. Ann Thorac Surg. 2001; [6] Arlt M. Extracorporeal membrane oxygenation in severe trauma patients with bleeding shock. Resuscitation. 2010 7 Adult respiratory distress syndrome (ARDS) [1]; Bridge for lung transplantation and primary graft failure following it [1]; Severe pneumonia and sepsis [1]; Reversable respiratory failure causes (e.g. aspiration pneumonitis, asthma, near drowning, and Wegener granulomatosis)[4]. More MoreRecommended* Recommended* Less Recommended* Respiratory indications Indications for the use of ECMO Introduction Aims Methods Results Conclusions Acknowledgements References * In published literature 8 [1] Marasco SF. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008; [4] Sidebotham D. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory disease in adults: Part 1--overview of extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009 ECMO support Introduction ADVANTAGES Aims Support of the critically ill patients. Methods Successfully implemented in several situations (stated previously); Results The benefits of ECMO were seen in the CESAR trial regardless of age, duration of ventilation, diagnosis, and number of organs failing [7]. The heterogenic data, due to the several indications, and the lack of quality Conclusions Acknowledgements References randomized trials in adults, difficult the evaluation of the benefits of this technique. 9 [7] Peek GJ. CESAR: a multicentre randomised controlled trial. Lancet. 2009; ECMO support Introduction DISADVANTAGES Aims Mechanical complications (e.g. oxygenator failure, tubing/circuit disruption, pump Methods or heat exchanger malfunction, problems with cannula placement/removal) [8]; Results Bleeding, coagulopathy and haemolysis [2], [8], [9]; Hemorrhages associated with anticoagulation requirements [2], [8], [9]; Compartment syndrome and leg ischemia [2], [9]; Conclusions Acknowledgements References Air embolism, thromboembolism and neurological sequelae [1], [2], [10]; 10 [1] Marasco SF. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008; [2] Lindstrom SJ. Extracorporeal membrane oxygenation. Med J Aust. 2009; [8] Conrad SA. Extracorporeal Life Support Registry Report 2004. ASAIO J. 2005; [9] Luo XJ. Extracorporeal membrane oxygenation for treatment of cardiac failure in adult patients. Interact Cardiovasc Thorac Surg. 2009; [10] Rossi M. Cardiopulmonary bypass in man. Ann Thorac Surg. 2004. Aims Introduction MAIN OBJECTIVE > Determine if the application of the ECMO (Extracorporeal membrane oxygenation) support is better, in detriment of the usual standard care, in critically ill adult patients who present cardiac or respiratory failure (or both). Aims Methods Results Conclusions Acknowledgements OTHER OBJECTIVES References Evaluate the support of ECMO in the treatment of the least recommended indications in the literature. 11 Study design Introduction > SYSTEMATIC REVIEW + META-ANALYSIS × Analysis of previously published articles (observational studies and clinical trials). In order to compile as many information published as possible, studies were sought, particularly those which had examined the application of ECMO in different cases of critically ill patients. > A query was created and criteria for selection was defined. Aims Methods Results Conclusions Acknowledgements References 12 Methods Introduction Aims Methods Results Conclusions Acknowledgements References 13 Collecting articles Introduction Aims Methods Results Conclusions Acknowledgements References 14 Collecting articles > The literature research was conducted using the following Online databases: PubMed/MEDLINE, [http://www.ncbi.nlm.nih.gov/pubmed/]; Introduction Aims ISI Web of Knowledge [http:// www.isiknowledge.com]; Methods SciVerse/SCOPUS [http://www.scopus.com/home.url ]. Results Conclusions In order to conduct the literature research it was imperative to develop specific query’s to apply on Acknowledgements the chosen databases. The development of the query’s were based in the analysis of the main objective of this article. Determine if the application of the ECMO (extracorporeal membrane oxygenation) support is better, in detriment of the usual standard care, in critically ill adult patients who present cardiac or respiratory failure (or both). References 15 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE > To include ECMO related articles referring only to adult patients, the following descriptors were applied: Introduction Aims Methods ‘Extracorporeal membrane oxygenation’ [MeSH] ‘Adult’ [MeSH] ENTRY TERMS BRANCHES Results Conclusions Oxygenation, Extracorporeal Membrane Aged Acknowledgements Extracorporeal Membrane Oxygenations Aged, 80 and over Membrane Oxygenation, Extracorporeal Fair elderly Membrane Oxygenations, Extracorporeal Middle aged Oxygenations, Extracorporeal Membrane Young adult ECMO References 16 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE > To include patients whose state of disease may lead to eminent death, the following descriptors Introduction Aims Methods were applied: ‘Critical care’ [MeSH] ‘Critical illness’ [MeSH] Results ENTRY TERMS ENTRY TERMS Conclusions Critical care Critical illness(es) Critical ill ‘Life support care’ [MeSH] References ‘Respiratory insufficiency’ [MeSH] Life support care Respiratory failure / depression Prolongation of life Ventilatory depression Extraordinary treatment(s) Acknowledgements 17 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE > To include patients whose state of disease may lead to eminent death, the following descriptors Introduction Aims Methods were applied: ‘Heart failure’ [MeSH] ‘Catastrophic illness’ [MeSH] Results ENTRY TERMS ENTRY TERMS Conclusions Cardiac failure Catastrophic illness(es) Myocardial failure Heart failure Heart decompensation Congestive heart failure Acknowledgements References ‘Acute disease’ [MeSH] Acute disease(s) 18 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE Introduction Aims Methods Query obtained and applied on PUBMED/MEDLINE Results (“Extracorporeal membrane oxygenation"[MeSH] OR "Extracorporeal Life Support") AND Conclusions ("Adult"[MeSH]) AND ("Acute Disease"[Mesh] OR "Critical Illness"[Mesh] OR "Severe Illness" OR "Critical Care"[Mesh] OR "Life Support Care"[Mesh] OR "Catastrophic Illness"[Mesh] OR "Heart Failure"[MeSH] OR "Respiratory Insufficiency"[MeSH]) Acknowledgements References 19 Portuguese and Spanish terms were not incorporated. An aditional research revealed that such terms are not effective, as their omittance gave the same results. The presented query returned 7 articles written in Portuguese and/or Spanish. Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE Introduction Aims Methods Concepts presented in full article TOPICS ECMO OR Extracorporeal Membrane Oxygenation OR Extracorporeal Life Support (Acute OR Critical OR Severe OR Catastrophic OR Life Support) AND (Disease OR Diseases OR Illness OR Illnesses OR Care) Results Conclusions Acknowledgements References (adult OR "Young Adult" OR "Middle Age“ OR aged) 20 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE Introduction Aims Methods Query obtained and applied on SCOPUS Results (ALL(ecmo OR extracorporeal membrane oxygenation OR extracorporeal life support) AND ALL((acute OR critical OR severe OR catastrophic OR life support) AND (disease OR diseases OR illness OR illnesses OR Conclusions Acknowledgements care)) AND TITLE-ABS-KEY(ecmo OR "Extracorporeal Membrane Oxygenation")) AND ALL((adult OR "Young Adult" OR "Middle Age" OR aged)) References 21 Portuguese and Spanish terms were not incorporated. An aditional research revealed that such terms are not effective, as their omittance gave the same results. The presented query returned 3 articles written in Portuguese and/or Spanish. Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE Introduction Aims Definition of the topic Methods TOPICS (ecmo OR extracorporeal membrane oxygenation OR extracorporeal life support) (acute OR critical OR severe OR catastrophic OR life support) AND (disease OR diseases OR illness OR illnesses OR care) Definition of the target group and thematic scope Results Conclusions Acknowledgements References REFINED BY General Categories=( SCIENCE & TECHNOLOGY ) [excluding] Subject Areas=( PEDIATRICS ) 22 Building query ECMO | CRITICALLY ILL | ADULT PATIENTS | CARDIAC OR RESPIRATORY FAILURE Introduction Aims Query obtained and applied on ISI WEB OF KNOWLEDGE Methods Results Topic=(ECMO OR Extracorporeal Membrane Oxygenation OR Extracorporeal Life Support) AND Topic=((Acute OR Critical OR Severe OR Catastrophic OR Life Support) AND (Disease OR Diseases OR Illness OR Illnesses OR Care)) Conclusions Acknowledgements Refined by: General Categories=( SCIENCE & TECHNOLOGY ) AND [excluding] Subject Areas=( PEDIATRICS ) References Timespan=All Years. 23 Portuguese and Spanish terms were not incorporated. An aditional research revealed that such terms are not effective, as their omittance gave the same results. The presented query returned 6 articles written in Portuguese and/or Spanish. Collecting articles Introduction The research returned: Aims 381 Methods Results 813 Conclusions 970 Acknowledgements After elimination of duplicates, there was a total of 1444: 2164 Total articles Unique articles References 1444 24 Methods Introduction Aims Methods Results Conclusions Acknowledgements References 25 First selection phase Introduction Aims Methods Results Conclusions Acknowledgements References 26 Inclusion and exclusion criteria Introduction Inclusion Criteria All studies with appropriate data relating to the support Aims of ECMO in the treatment of critically ill adult patients; Methods Results Clinical trials and observational studies with control group. Conclusions Acknowledgements Exclusion Criteria Articles not available using UP credentials; References Articles without original data (review articles, meta-analysis); Articles not written in English, Portuguese or Spanish; Studies reporting out-of-hospital ECMO; Absense of control group. 27 First selection phase The titles and abstracts of the articles were reviewed by two revisors. Introduction Aims 1358 Excluded Language 1 Not available 2 Article type 3 Methods Results 78 Conclusions 53 Acknowledgements 450 References 4 398 Population 5 377 Not relevant Included 86 1 – Article not written in English, Portuguese or Spanish 2 – Article not available for consult 3 – Article is not a observational study or clinical trial 4 – Study does not contain relevant data 5 – Population does not have the desired characteristics 28 Methods Introduction Aims Methods Results Conclusions Acknowledgements References 29 Second selection phase Introduction Aims Methods Results Conclusions Acknowledgements References 30 Second selection phase Introduction The article was fully reviewed by two revisors. Aims 76 Excluded Methods Results Article type 1 3 Conclusions Not relevant 2 23 Acknowledgements Control group 3 Population 4 Not available5 Included 33 3 14 10 References 1 – Article is not a observational study or clinical trial 2 – Study does not contain relevant data 3 – No control group was present 4 – Population does not have the desired characteristics 5 - Article not available for consult 31 Second selection phase Introduction > In the process of reading full articles, revisors decide if they fulfill the criteria to be included. In order to help assess the quality of the article, revisors use Aims the CONSORT [11] (for reporting randomized trials) and STROBE [12] (for Methods reporting observational studies) checklists. Results Conclusions Acknowledgements References 32 [11] von Elm E.The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies]. Rev Esp Salud Publica. 2008. [12] Moher D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. JAMA. 2001. Second selection phase Quality evaluation of included publications. Author Checklist Score (0-22) Beiderlinden M, et al. [13] STROBE [11] 18 Cianchi G, et al. [14] STROBE [11] 19 Shin TG, et al. [15] STROBE [11] 17 Roch A, et al. [16] STROBE [12] 15 Peek GJ, et al. [7] STROBE [11] 18 Klotz S, et al. [17] STROBE [11] 13 ANZ ECMO et al. [18] STROBE [11] 17 Lin JW, et al. [19] STROBE [11] 16 Schellonwgowski P, et al. [20] STROBE [11] 15 Taghavi S, et al. [21] STROBE [11] 17 Introduction Aims Methods Results Conclusions Acknowledgements References 33 [11] von Elm E.The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies]. Rev Esp Salud Publica. 2008. [12] Moher D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. JAMA. 2001. Methods Introduction Aims Methods Results Conclusions Acknowledgements References 34 Data extraction Introduction Aims Methods Results Conclusions Acknowledgements References 35 Data extraction Introduction > Google Docs was the plataform used to build forms, which were used for the Aims extraction of data. It was then compiled using spss. Methods Results Conclusions Acknowledgements References 36 Fig.3 Image of form used to extract data Data extraction Table 3 Synthesis table with data from each study. Introduction st 1 author Publication year Study type Population: Total Age, median (ECMO/Control) (ECMO/Control) Intervention Comparison Complications Outcomes Aims Peter Schellongowski 2011 Observational study 17 (10/7) 45/38 Veno-venous 50% of patients Conventional ECMO (8 patients) Bleeding occurred died in ECMO treatment and Veno-arterial in 41% of patients group and 71% in without ECMO ECMO (2 patients) control group 45/42 Bleeding (42,9 % 14,3% died in ECMO group); no ECMO group; No complications deaths in control referred on group control group Methods Results Giovanni Cianchi Antoine Roch Jou-Wei Lin Stefan Klotz 2011 Observational study 2010 Observational study 12 (7/5) 18 (9/9) 2010 Observational study 2007 183 (n=150 Observational ECMO; n=20 VAD; study n=13 ECMO-VAD) 118 (55/63) 49/54 59/60,6 65,9/41,7 VV Ecmo Conventional ventilation VA and VV ECMO Without ECMO E-CPR (Extracorporeal cardiopulmonary resuscitation) VA ECMO C-CPR (conventional CPR) Haemorrhagic 56% died in complications in ECMO group; 56% ECMO group died in control (44,4%) group No referrences Conclusions Acknowledgements References Survival to discharge: 29,1% ECPR, 22,2% CCPR; Survival at 1 year: 20,0%, 17,5 % Right heart failure (25%); 75% died in Ventricular Assist Cerebral bleeding ECMO group; 50% Device (VAD) (13%); VAD defect died in VAD group (6%) 37 Data extraction Introduction > The variables selected for extraction are listed below: Aims Methods Numerical Categorical Results CONTINUE NOMINAL Mortality Indication Duration of ECMO Complication Age ECMO modality Sample size Control type Conclusions Acknowledgements References 38 Data extraction Introduction > The follow categories were created to code the data: Aims Methods ECMO modality Complications Indications Control Results VA EMCO Thromboembolic Respiratory Mechanical VV ECMO Hemorragic Cardiac Pharmacological Combined Infectious Other Other Other Mechanical Conclusions Acknowledgements References Other 39 Data extraction > Whenever data was available, subgroup analysis would be performed considering: The primary outcome - Mortality Introduction Aims Methods Results Subgroup Analysis: × Type of intervention; × Indication; × ECMO vs Control; × Intervention duration × Modality of ECMO; Conclusions Acknowledgements References The primary outcome - Complications Subgroup Analysis: × Type of intervention × Modality of ECMO; × ECMO vs Control × Indication; 40 Statistical analysis Introduction Aims > After data extraction, it was compiled in a single document in order to Data Data Results simplify its posterior analysis, in Review Manager 5. Methods Data Conclusions Acknowledgements References ORGANIZED AND ANALYZED 41 Data extraction Introduction STUDY TYPE > Clinical trial (1) The quality of reviews is influenced by the type of studies found in the articles selected. Aims Methods Results Conclusions Acknowledgements > Consequences: References x Less control of the intervention; Observational study (9) x Lower valid results. 42 Data extraction THERAPY Introduction Aims Pharmacological (2) Methods Results > Most control groups used Conclusions conventional mechanical Acknowledgements treatments. References Mechanical (8) 43 Data extraction ECMO MODALITY Introduction Aims VA ECMO > VV ECMO It was verified that VV Methods ECMO was more Results requested, although the Both frequencies of the use of MISSNG each modality were Other Conclusions Acknowledgements References similar. 0 1 2 3 44 Data extraction ECMO INDICATIONS Introduction Aims > Cardiac indication The main indications Methods observed for the use of Results ECMO were respiratory. Respiratory indication MISSING > There were some difficulties categorizing the Other 0 1 2 3 4 5 6 Conclusions Acknowledgements References diagnosis. 45 Data extraction ECMO COMPLICATIONS Introduction Aims Hemorrhagic > Neurological Complications were mainly observed in ECMO’s group. Methods Results Thromboembolic Infectious > Mechanical There was almost no reference to the amount of MISSING individuals who suffered Other Conclusions Acknowledgements References from each complication. 0 1 2 3 4 5 6 46 Mortality rates ANZ ECMO ECMO group Beiderlinden M Introduction Aims Control group Cianchi G Methods Klotz S Results Lin JW Conclusions Pee GJ Acknowledgements Roch A References Schellongowski P Shin TG 47 Taghavi S 0% 25% 50% 75% 100% Results RESPIRATORY + CARDIAC INDICATIONS Introduction Aims Methods Results Conclusions Acknowledgements References 48 Results RESPIRATORY + CARDIAC INDICATIONS > There was no statistical difference between ECMO and Control groups. Introduction Aims Methods Results > Studies with a higher N and more control over the intervention would be needed to achieve better conclusions. Conclusions Acknowledgements References Does it worth to continue using ECMO over other conventional therapies? 49 Results RESPIRATORY INDICATIONS Introduction Aims Methods Results Conclusions Acknowledgements References 50 Results RESPIRATORY INDICATIONS > There was no statistical difference between ECMO and Control groups. Introduction Aims Methods Results > Conventional therapies showed better results than ECMO’s therapies. Conclusions Acknowledgements This data contradicts the scientific literature. References 51 Results CARDIAC INDICATIONS Introduction Aims Methods Results Conclusions Acknowledgements References 52 Results CARDIAC INDICATIONS Introduction Aims > There was no statistical difference between ECMO and Control groups. Methods Results > ECMO support showed better results than ECMO’s treatments. This data is against the scientific literature. Conclusions Acknowledgements References 53 Results CARDIAC INDICATIONS Introduction Aims Methods Results Conclusions Acknowledgements > Control seems to be advantageous over ECMO. > ANZ ECMO et al. has a weight that far exceeds other studies (74,4%). The results are biased, therefore it is not possible to draw conclusions. References 54 Cost assessment > Compared to conventional therapies, ECMO is more expensive; > According to Peek et al. (2009), this values are relevant to other countries where ECMO is provided or being considered, although local costs, health services, Introduction Aims Methods practice, and distances from treatment centers might vary. Results Conclusions Mean* ECMO 83 354 € Conventional management 37 684 € Cost difference Acknowledgements References 45 670 € + 121 % 55 *Value per patient in a six months period. Data from Peek et al. (2009)[7] Conclusion Introduction > The use of ECMO in critically ill adults does not offer any improvement; Aims > There is a tendency for ECMO to have better results (lower mortality) in cardiac indications; Methods Results > Conventional treatments present better results in respiratory indications; > ECMO has more complications than other therapies; Conclusions Acknowledgements > More clinical trials are needed to establish a more valid assumption. References Before embarking on the costly task of instituting an ECMO program for adults, healthcare systems should carefully evaluate the comparative effectiveness of ECMO compared with conventional treatments. 56 Study limitations > Low number of clinical trials compared to the number of observational studies (1/9); > Bias inherent to original data from observational studies could not be eliminated; > Some articles were not accessible using UP credentials; > Lack of data related to indication, complications, Introduction Aims Methods Results Conclusions Acknowledgements References among others; > Individual outcomes were affected by the period in which they occurred. 57 Acknowledgements Introduction “ Aims We gratefully thank our Professor Filipa Canário for her endeavor throughout the whole year, whose help allowed us to complete the task we have been assigned. Moreover, we feel our acknowledgements should also be directed to Professor Altamiro Pereira, PhD, whose reviews provided our work an undeniable level of quality. Methods Results Conclusions Acknowledgements References 58 References [1] Marasco SF, Lukas G, McDonald M, McMillan J, Ihle B. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008; 17 Suppl 4:S41-7 [2] Lindstrom SJ, Pellegrino VA, Butt WW. Extracorporeal membrane oxygenation. Med J Aust. 2009 Aug 3; 191(3):17882 [3] Schmid C, Philipp A, Mueller T, Hilker M. Extracorporeal life support - systems, indications, and limitations. Thorac Cardiovasc Surg. 2009 Dec; 57(8):449-54 [4] Sidebotham D, McGeorge A, McGuinness S, Edwards M, Willcox T, Beca J. Extracorporeal membrane oxygenation for treating severe cardiac and respiratory disease in adults: Part 1--overview of extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009 Dec ;23(6):886-92 [5] Fiser SM, Tribble CG, Kaza AK, Long SM, Zacour RK, Kern JA, et al. When to discontinue extracorporeal membrane oxygenation for postcardiotomy support. Ann Thorac Surg. 2001 Jan;71(1):210-4 Introduction Aims Methods Results Conclusions Acknowledgements References [6] Arlt M, Philipp A, Voelkel S, Rupprecht L, Mueller T, Hilker M, et al. Extracorporeal membrane oxygenation in severe trauma patients with bleeding shock. Resuscitation. 2010 Jul; 81(7):804-9 [7] Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17; 374(9698):1351-63 [8] Conrad SA, Rycus PT, Dalton H. Extracorporeal Life Support Registry Report 2004. ASAIO J. 2005 Jan-Feb; 51(1):4-10 59 References [9] Luo XJ, Wang W, Hu SS, Sun HS, Gao HW, Long C, et al. Extracorporeal membrane oxygenation for treatment of cardiac failure in adult patients. Interact Cardiovasc Thorac Surg. 2009 Aug; 9(2):296-300 [10] Rossi M, Sganga G, Mazzone M, Valenza V, Guarneri S, Portale G, et al. Cardiopulmonary bypass in man: role of the intestine in a self-limiting inflammatory response with demonstrable bacterial translocation. Ann Thorac Surg. 2004 Feb; 77(2):612-8 [11] von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. [The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies]. Rev Esp Salud Publica. 2008 May-Jun;82(3):251-9. [12] Moher D, Schulz KF, Altman D; CONSORT Group (Consolidated Standards of Reporting Trials). The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. JAMA. 2001 Apr 18;285(15):1987-91. [13] Beiderlinden M, et al. Extracorporeal gas exchange. Intensive Care Medicine. 2006 Oct;32(10):1627-31. Introduction Aims Methods Results Conclusions Acknowledgements References [14] Cianchi G, et al. Ventilatory and ECMO treatment of H1N1-induced severe respiratory failure: Results of an Italian referral ECMO center. BMC Pulmonary Medicine. 2011 Jan 11;11:2. [15] Shin TG, et al. Extracorporeal cardiopulmonary resuscitation in patients with inhospital cardiac arrest: A comparison with conventional cardiopulmonary resuscitation. Critical Care Medicine. 2011 Jan;39(1):1-7. 60 References [16] Roch A, et al. Extracorporeal membrane oxygenation for severe influenza A (H1N1) acute respiratory distress syndrome: A prospective observational comparative study. Intensive Care Medicine. 2010 Nov;36(11):1899-905. [17] Klotz S, et al. Primary extracorporeal membrane oxygenation versus primary ventricular assist device implantation in low cardiac output syndrome following cardiac operation. Artificial Organs. 2007 May;31(5):390-4. [18] ANZ ECMO et al. [19] Lin JW, et al. Comparing the survival between extracorporeal rescue and conventional resuscitation in adult inhospital cardiac arrests: Propensity analysis of three-year data. Resuscitation. 2010 Jul;81(7):796-803. Introduction Aims Methods Results Conclusions [20] Schellonwgowski P, et al. A surge of flu-associated adult respiratory distress syndrome in an Austrian tertiary care hospital during the 2009/2010 Influenza A H1N1v pandemic. Wien Klin Wochenschr. 2011 Apr;123(7-8):209-214. Acknowledgements [21] Taghavi S, et al. Extracorporeal membrane oxygenation is superior to right ventricular assist device for acute right ventricular failure after heart Transplantation. Annals of Thoracic Surgery. 2004 Nov;78(5):1644-9. References 61 DO YOU HAVE ANY QUESTIONS? 62