Back to Basics
advertisement

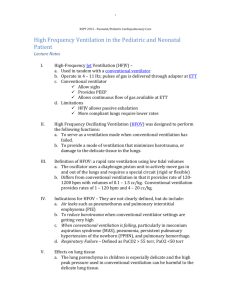
High Frequency Ventilation Back to Basics Case Two hfov • • BG is 39 wk, 3400 g infant vaginally delivered to 27 YO G1P0 mom with complete prenatal care. At delivery, amniotic fluid is meconium • stained and BG is distressed.no time for amnioinfusion of saline,because of variable deceleration that is recommmended in 41 gw Case Two hfov • • Direct laryngoscopy reveals meconium in airways. BG intubated with 3.5 mm ETT and suctioned with meconium aspirator for thick meconium.BG lavaged with Surfactant and placed on SIMV: f = 40; PIP = 25; PEEP = 5;FIO2 = 1.0-ABG: 7.21/78/73 • Over several hours, f increased to 60;PIP increased to 40. • BG worsened. CXR revealed Rt pneumothorax. Post-chest tube ABG:7.08/85/46. • HFO initiated. f = 5 Hz; delta P = 32;MAP = 26.-ABG: 7.19/75/45 • What to do about PaO2?What to do about PaCO2? • 4/5/2011-Copyright 2008 AP Jones 11 Case Two hfov • ABG: 7.19/75/45 • What to do about PaO2? • MAP increased to 30, observing SPO2 • and CXR • What to do about PaCO2? • delta P increased to 36 • ABG: 7.32/52/85 Case Two hfov • Over two days, BG improves; but small • air leak persists. • FIO2 weaned to 40% with SPO2 • ABG: 7.56/24/213 • Next changes? Case Two hfov • Over two days, BG improves; but small • air leak persists. • FIO2 weaned to 40% with SPO2 • ABG: 7.56/24/213 • Next changes? • reduce MAP, using SpO2 = 94% • reduce delta P to 30 for PaCO2 hfjv Case One • 26 wk 700 g BG-Intubation and surfactant in DR • Initial ventilator settings TV = 12 mL,rate = 60/min, FIO2 = 60%; PEEP = 6 cm H2O - couldn't wean FIO2’More surfactant - no changes (RDS)Over 36 H, PIP increased from low 30s to 55 cm H2O - CXR after CMV • Click to see CXR after 36 H on CMV Case Two 41 wk, 3500 g BB Delivered with meconium in amnion and in upper airways,Intubated, suctioned through ETT Lavaged with surfactant,Placed on nCPAP = 6; FIO2 = 35%; SpO2 = 89% then to NICU-6 H later, SpO2 decreased and RR increased to 80/min Case Two Placed on volume-control ventilator with FIO2 = 50%; TV = 22 mL; rate = 40/min; PEEP = 6 cm H2O; PIP = 48 cm H2O; MAP = 18 cm H2O ABGs: PaO2 = 45 mm Hg; SaO2 = 81%; PCO2 = 76 mm Hg; pH = 7.18 Changed to jet ventilator Settings?? Case Two • • Initial settings for jet ventilation companion FIO2 = 60%; PEEP = 8 cm H2O for MAP = 18 cm H2O;rate = 5/min jet FIO2 = 60%; rate = 360/min; • PIP = 46 cm H2O-it=0/02 seconds • ABGs: PaO2 = 42 mm Hg; PaCO2 =75 mm Hg; pH = 7.10 • Click to see a chest radiograph of RDS • http://img.medscape.com/pi/emed/ckb/radiology/336139- 410756-9164.jpg Case Two • • • Ventilator adjustments-companion PEEP increased to 10 cm H2O for MAP = 20 cm H2O; rate decreased to zero jet rate decreased to 240/min ABGs: PaO2 = 59 mm Hg; SaO2 =91%; PaCO2 = 55 mm Hg; pH = 7.27 • CXR - less hyperinflation • Note: increased PIP might decrease • PaCO2; but decreased rate worked • by decreasing I:E Case Two Over two days, CXR improved and patient stable on FIO2 = 38%; PIP =22 cm H2O; PEEP = 8 cm H2O PIP weaned to zero; FIO2 weaned to 30% with patient stable Patient extubated to nCPAP Radiographs during the first day of life with increasing with small amount of MAP with the danger of silent recruitment • For a 30-week premature infant with RDS managed with HFOV to achieve mean lung volume(MVL). • A=initial PAW=10 cmH2O,fio2=1 • B=at 12 hours of age,with PAW=15 cmH2OFIO2=0/45 • C=at 24 hours of age,PAW=12cmH2O,FIO2=/ 28.silent recruit has occured Radiographs of a 2-day-old preterm ON HFOV • With pulmonary intersticial emphysema(PIE) • A=,paw=16 cmH2O,FIO2=0/65. • B=six hours later,paw=8 cmH2O,FIO2=1 • C=twelve hours later,settings were unchanged. • D=thirty-six hours later,reinflation was beginning,paw=12cmH2O,FI O2=0/45 Reductions in MAP would usually be made when the FiO2 is < 40% The Optimal Lung Volume Strategy recruits alveoli and lung segments and once an optimal lung volume is achieved recruitment, lung volume and oxygenation can be maintained with a lower MAP. The repeated stretch group received 15-sec sustained inflations at 30 cm H2O mean airway pressure every 20 mins, with maintenance mean airway pressure sufficient to keep PaO2 > 350 torr (46.7 kPa) Chest wiggle frequency ƒneonates from nipple line to umbilicus ƒadults • In neonate from nipple line to umbilicus Ventilation Ventilation is primarily determined by the stroke volume (Delta-P) or the frequency of the ventilator. Alveolar ventilation during CMV is defined as: F x Vt Alveolar Ventilation during HFV is defined as: F x Vt 2 Therefore, changes in volume delivery (as a function of pressure-amplitude, frequency, or % inspiratory time) have the most significant affect on CO2 elimination HFV: Start MAP(PEEP): 2-5-(8) mbar above MAP of conventional ventilation; if necessary, increase MAP until pO2 () after 30 min: X-ray: 8-9 rib level IMV rate: 3bpm pressure: 2 to 5 mbar below conventional ventilation HFV frequency: 10 Hz HFV amplitude: 100% watch thorax vibrations HFV volume: about 2 to 2.5 ml/kg • Troubleshooting during HFOV • Low PaO2 : Consider: • • ET tube patency • • check for chest movement and breath sounds • • check there is no water in the ETT/T-piece • • Air leak/pneumothorax • • chest moving symmetrically? • • transilluminate • • urgent chest x-ray • Sub-optimal lung volume recruitment Over-inflated lung • Sub-optimal lung volume recruitment • • increment MAP • • consider chest x-ray • • Over-inflated lung • • check blood pressure • • reduce MAP; does oxygenation improve? • • consider chest x-ray High PaCO2: Consider: • • ET tube patency and air leaks (as above) • • Insufficient alveolar ventilation • • Increase amplitude, does chest wall movement increase? • • Increased airway resistance (MAS, BPD) or non-homogenous lung disease: Is HFOV appropriate? • • Under-inflated lungs, amplitude being delivered on non compliant part of the pressure(volume curve ie point A in figure 2) • • Over-inflated lungs, amplitude being delivered on non compliant part of the pressure(volume curve ie point C in figure 2) • • If all the above seem OK try reducing oscillator frequency; lung impedance and airway • resistance fall, leading to increased VT. Persisting acidosis/hypotension: Consider: • • Over-distension • • reduce MAP; does oxygenation improve? • • consider chest x-ray Why are mean airway pressures higher on HFOV? • Mean airway pressure seem to be higher on HFOV because unlike conventional and jet ventilation, there are no conventional (tidal) breaths to recruit the lung. Optimal gas exchange occurs when the lung is at FRC. Depending on the severity of lung disease, the pressures required to recruit the lung to FRC may seem high. "Based on the relationships between MAP, compliance, functional residual capacity, and indexes of ventilation/perfusion matching, we conclude that increasing MAP to achieve normal FRC... is a simple method of optimizing lung volume in surfactant depleted subjects [during HFOV]." . The choice of strategy is specific for every disease: • 1=to inflate an underinflated lung • Recruitment maneuver • 2=to deflate an onerinflated lung • derecruitment Non-uniform inflation occurring in non-homogenous lungs CMV’s with high PIPs aimed at recruiting alveoli Those pressures are also transmitted to the healthiest regions of the the lungs Over-distention and over-pressurization produces volutrauma and barotrauma Inflammatory Cascade is triggered Three Words: Small Tidal Volumes Small Tidal Volumes allow gas exchange to occur using extremely small volume displacements of ventilatory gases Small Tidal Volumes < Anatomical Dead Space Small Tidal Volumes allow safer use of Optimal PEEP minimizing the risk of atelectasis and oxygen toxicity Often referred to as Lung Protective Ventilation/Strategy Physiologic Basis for Rapid, Small Tidal-Volume Breathing Henderson was intrigued by the shallow breathing of panting dogs in 1915. He wondered how dogs could pant indefinitely without becoming hypoxic or hypercapnic. So, he designed an experiment to find out. *Y Henderson, FP Chillingworth, JL Whitney - American Journal of Physiology, 1915 Henderson filled his mouth with tobacco smoke and blew it into a glass tube in one quick puff The smoke shot down the tube in a long spike He then stuck his tongue over the end of the tube to stop the flow. Diffusion took over as flow stopped, and the effect disappeared We call this phenomenon FLOW STREAMING, the type of flow we try to create with our HFJV inspirations *Y Henderson, FP Chillingworth, JL Whitney - American Journal of Physiology, 1915 The column of smoke shoots across the center of the bulb with very little contamination of the clear air surrounding the stream Again, if the flow is stopped, a complete mixing of smoke and air occurs almost instantaneously *Y Henderson, FP Chillingworth, JL Whitney - American Journal of Physiology, 1915 Henderson concluded that with the proper flow pattern, “a tidal volume even much smaller than the volume of dead space my thus afford a very considerable gaseous exchange” *Y Henderson, FP Chillingworth, JL Whitney - American Journal of Physiology, 1915 Evolved from studies of pulmonary physiology using mathematics, fluid mechanics, and other engineering principles. Facilitates gas exchange by sending a steady stream(bulk flow) of very small tidal volumes into the airways using relatively low PIPs (peak airway pressures). The further the gas goes into the airways, the lower those airway pressures are. Monitoring and controlling HFV with airway pressure instead of tidal volumes creates problems for many clinicians Pressure is a Dependent variable It depends on gas flow, tidal volume, airways resistance, and lung compliance High frequency ventilation • Techniques HFPPV HFJV HFOV HFFI VT >dead sp > or < ds > or <ds <ds Exp passive passive passive active triangular triangular Wave- variable wave sine form Entrai- none possible (/min) ment Freq. 60-150 none 60-600 none 300-900 Airway Pressures during HFV Trachea & Proximal Airways Distal Airways & Alveoli 20 P 15 HFJV 10 5 20 P 15 10 5 Paw Amplitude attenuates; PEEP stays constant, MAP declines HFOV Paw Amplitude attenuates; PEEP increases; MAP fixed when I:E = 1:1, less at 1:2 Conventional studies indicate that smaller tidal volumes are safer than larger tidal volumes * As Tidal Volumes are pushed smaller and smaller, two things must be raised: PEEP/MAP - to keep the lungs open Rate - to maintain an normal PaCO2 Once you get over 150 bpm, you’re in the domain of high frequency ventilation *Kacmaerk RM, Chiche J-D. Resp. Care 1998;43:724-727 & Lee PC, Helemoortel CM,Cohn Sm, Fink MP. Chest 1990;97:430-434 Conventional Ventilation Alveolar Ventilation = Rate x Tidal Volume High Frequency Ventilation Alveolar Ventilation = Rate x Tidal Volume 2 During CV gas exchange occurs mostly from Bulk Transport (convective flow) of the O2 and CO2 molecules between the central (conducting) airways and the peripheral airways The volume of inhaled gas must exceed the volume of dead space. Image Source:www.homehealth-uk.com/ image/lungs.jpg Bulk Axial Flow - Convection Interregional Gas Mixing - Pendelluft Effect Asymmetric Velocity Profiles Axial and Radial Augmented Dispersion - Taylor Dispersion Convective Dispersion Augmented Molecular Diffusion HFV gas distribution is more affected by the resistance of the lungs than the compliance. Normal, tidal ventilation gas delivery is more affected by the compliance of the lungs than resistance. Gas transport mechanisms during HFOV Bouchut JC et al. Anesthesiology 2004; 100:1007-12 • “Often the most critical factor in determining optimal gas exchange (oxygenation) as it correlates with lung volume.” • Neonatal/Pediatric Respiratory Care: A Critical Care Pocket Guide - Dana Oakes The “Essentials” of HFV Lungs inflation is essential to adequate oxygenation Maintenance of airway patency is essential to adequate ventilation Minimizing mechanically delivered VT is essential to prevention of lung injury PEEP/ MAP issues MAP & HFJV Don’t let the MAP fall when initiating HFJV !! CV = larger tidal volumes • HFJV = Gentle Ventilation MAP * PEEP Time *You must raise PEEP to maintain MAP for Stabilization / Oxygenation. When HFV rate approaches the natural or Resonant Frequency of the lungs, then the airway pressure needed for proper ventilation can be minimized. The natural frequency of premature infant lungs is around 40 Hz, which is far beyond the capability of any mechanical ventilator. The most basic differences between HFOV and HFJV are: HFJV squirt gas into the lungs faster than Oscillators Oscillators get the gas back out faster than Jets by actively sucking it out Oscillators with their I:E ratio of 1:2 use symmetrical pressure waveforms that are very effective in treating homogenous lung disorders like RDS HFOV typically uses higher Mean Airway Pressures than either HFJV or CV because its baseline pressure has to be raised to counteract the negative, sucking action of its expiratory mode to avoid airway collapse and gas trapping Tracer bolus limits Start of Inspiration Inspiratory Velocity Profiles End of Inspiration Start of Exhalation End of Exhalation Expiratory Velocity Profiles Tracer bolus tip in middle of airway has moved towards alveoli Modified from Haselton et al., Science, 1980 Initial position of tracer bolus Deformation of bolus after a few HFOV cycles Modified from Haselton et al., Science, 1980 HFJV uses high velocity gas inspirations of short time duration (0.02 sec) Set, Fixed I-Time = Wide Variety of I:E Ratios These inspirations create substantial momentum which enable adequate oxygenation using less Mean Airway Pressure Allows HFV to use tidal volumes smaller than anatomic dead space volume because gas in the terminal airways gets replenished so rapidly that a substantial Partial Pressure difference is established with alveolar gas. This partial pressure difference facilitates Diffusion, and good gas exchange results HFJV is especially good at creating flow streaming because it squirts gas into the lungs with a great deal of Velocity. Amplitude (ΔP or power) • (Choose an Amplitude) • Although you can choose an amplitude between 0% and 100%, the amplitude delivered depends on the MAP – the lower the MAP, the lower the amplitude before the maximum is reached. • The amplitude is calculated the pressure fluctuation as a percentage of the difference between MAP and 60 mbar. • For example, if the MAP is 15, then 100% amplitude would be 45 mbar. Therefore, the pressure would be from -7.5 to 37.5 mbar • However, the airway pressure is limited to –4 mbar. Therefore, this limits the maximum effective MAP – you can set it at 100% but in the example above it will only deliver -4 to 34 mbar (total 38 mbar) which equals 84%! Therefore, the lower the MAP the lower the amplitude that will be effective. • The formula for this is: Maximum effective amplitude (%) = (2 x (MAP + 4))/(60MAP) x 100 HFV Ventilates so effectively that hypocarbia can easily be induced, especially when PEEP in inappropriately low. Inadvertent PEEP can develop when HFV rate is inappropriately high. And gas trapping can also occur when mean airway pressure is too low and airways become smaller thereby increasing restriction/resistance. There is a tendency to overdue alveolar recruitment strategies With HFOV, MAP is often left inappropriately high which over expands alveoli and interferes with cardiac output With HFJV, the ease with which IMV breaths are implemented leads to not enough PEEP/MAP with inappropriate high CMV rates and large tidal volumes Irrational fear of barotrauma can develop even though HFV tidal volumes are many, many times smaller than CMV 2. Stabilization 1. Recovery 3. Weaning Recovery Again High frequency jet ventilation (HFJV) • high frequency ventilation with • delivery of a tidal volume (1-3 • mL/kg) at a high flow (jet) • originally used for short-term • ventilation during airway surgery • (1970s) because of capability to • ventilate in face of leaks Baby Judy was born at 27 weeks of gestational age by cesarean section. Two weeks earlier, her mother had a preterm premature rupture of membranes (PPROM). She had been started on antibiotics and tokolysis. However, she developed amnionitis and went into preterm labour. The babies APGAR score was 3 / 7 / 7 at 1, 5 and 10 minutes, respectively. Her umbilical artery blood pH was 7.27.Initially, she was treated with CPAP but soon developed severe chest wall distortion, apneic and bradycardic episodes, and required an FiO2 above 0.60 to maintain her arterial oxygen saturation above 85%. She was therefore intubated 21 minutes after birth and received exogenous surfactant. Thereafter, oxygenation improved and Judy was transferred to the NICU where she continued on conventional controlled mechanical ventilation. To keep her Pa CO2 between 45 and 55 mm Hg, she needed PIPs between 15 and 20 cm H2O with 5 cm H2O of PEEP. Initiation of HFOV At day 3 of life her respiratory gas exchange deteriorated. The FiO2 had to be at 0.8 in order to achieve an arterial oxygen saturation > 85%. Her tcp CO2 was 65 mmHg and rising at this point. A second dose of exogenous surfactant caused a moderate but transient improvement in gas exchange so that she was started on HFOV. Ventilatory settings on SIMV immediately before the initiation of HFOV: Rate: 60/min PIP / PEEP: 25 / 5 cmH2O MAP: 10 cmH2O FiO2: 0.8 Ventilatory Settings on HFOV: Rate: 10 Hz MAP: 12 cmH2O • FiO2: 0.6 About 30 minutes after changing over to HFOV, her gas exchange improved: The FiO2 came down to 0.4. The Pa CO2 fell quickly into a target range between 40 and 50 mmHg. 1. X-ray after initiation of HFOV Unexplained cardiorespiratory deterioration after 2 days on HFOV Figure 2. Chest X-ray, day of life #7. • Judy remained clinically stable for the next 2 days while on HFOV with unchanged settings. Towards the end of day 7, however, her urinary output decreased from 4 cc/kg/h to 1.5 cc/kg/h. She had gained 70 gms of body weight since birth. There was no obvious change in arterial blood pressure. Arterial oxygen saturation fell to below 90%. Raising the FiO2 up to 0.9 had little effect on arterial oxygen saturation. The Pa CO2 remained unaffected. • The clinical team decided to increase the mean airway pressure under HFOV. Oxygenation did not improve: if anything, it appeared to fluctuate more. Subsequent clinical management The attending clinician requested a cardiac echo because there was such a poor response in systemic oxygenation when changing the FiO2. The echo showed a bidirectional ductal shunt, a right-to-left atrial shunt, and good contractility of the heart, which had a normal anatomy. The working hypothesis was that the pulmonary circulation became compromised while lung compliance had improved (the chest appeared hyperinflated on X-ray, and lung fields had cleared to some extent). The applied positive airway pressure during HFOV was initially appropriate. However, it hyperinflated the chest when lung function improved. The baby was changed back to SIMV in an attempt to allow better pulmonary perfusion during expiration with lower expiratory pressures (4 cm H2O) and a longer expiratory time. This immediately resulted in higher systemic oxygenation. Urinary output came back to 4–5 cc/kg/h. There was less right-to-left atrial shunting and the ductal shunt became left-to-right only on echo. Reminder: Transmission of a positive mean airway pressure (MAP) onto the pulmonary circulation depends on lung and chest wall compliance (Figure 3). Relationship between MAP pleural pressure (Ppl). Chest wall compliance is high in preterm infants. A larger fraction of the MAP is transmitted onto the pleural pressure when lung compliance (CL) increases. Ppl is a determinant of the pulmonary vascular resistance. K, transmission factor.