Patient Interval 2
advertisement

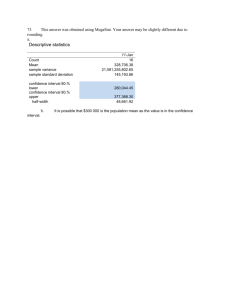
Individual Task Variability: Linking Process Improvement to Patient and Hospital Outcomes Susan Meyer Goldstein & Rachna Shah Cincinnati Innovations in Healthcare Delivery 2006 4/11/2020 Scenario… Treatment of ST-elevation mycardial infarction (STEMI) in Greater Minnesota 4/11/2020 Current Evidence Medical Science Balloon angioplasty (PCI) is preferred treatment for heart attack (based on numerous global studies) Practice Less than half receive primary balloon treatment; often delayed 4/11/2020 Pilot Study Source: Henry et al., American Heart Journal Vol 150, Issue 3, 2005 4/11/2020 Standardized Protocol 95 minutes Community hospital MHI Every patient, every time (24/7 coverage); no exclusions. Source: Henry et al., American Heart Journal Vol 150, Issue 3, 2005 4/11/2020 Patient arrives at rural hospital with STEMI symptoms Arrive at MHI Security holds elevator and escorts patient to cath lab Give 2 more doses of metoprolol during transport Remove patient shirt; put on gown Load patient into ground or air ambulance Perform ECG within 5 min. of arrival A cardiologist explains procedure to patient; another cardiologist preps patient Give sedation yes Is STEMI diagnos ed? yes Activate team (MD, nurse, technician) no End of process Is patient anxious ? Attach defibrillation pads Contact transport Start second IV no Perform angiogram (image the blockage) Does angiogr am confirm blockag e? yes Contact MHI Perform chest x-ray Perform PCI Locate prestocked kit Start IV and monitors, draw blood for testing (all in kit) 4/11/2020 Give aspirin, clopidogrel, nitroglycerin, heparin, metoprolol (all in kit) MHI’s Standardized Treatment Protocol for STEMI Move patient onto imaging table Complete procedure and transfer patient to recovery room no Outcomes – Patient Mortality 4/11/2020 Research Problem Practitioners’ questions: ·Can we further improve an already well-performing system? · Are the community hospitals doing everything they can? Researchers’ questions: · Are there systematic factors within process-level activities that can be improved? What is the impact of hospital-level task activity on the outcomes of interest? Patient-level task activity? 4/11/2020 Research Propositions Is the impact of variability in task activity on process performance (cost, quality) observable? What is the relative importance of hospital-level versus patient-level task activity in predicting performance? What are the impact of process handoffs? 4/11/2020 Literature Base Service process variability Frei et al. (1999), Management Science Tsikriktsis & Heineke (2004), Decision Sciences Field et al. (2006), Decision Sciences Process improvement Zantek et al. (2002), Management Science Rust & Metters (1996), EJOR Process handoffs Hammer (re-engineering) Shingo (set-ups) 4/11/2020 Sample Characteristics 27 Minnesota community hospitals Average 81 miles from MHI (range 17-149 miles) Data collection period: March 2003 – Feb. 2006 Total 720 patients Exclusions: 54 false positives, 4 extreme time outliers (2 for weather delay; 1 for diagnostic dilemma; 1 for LOS), 11 intentional protocol deviations/missing partial data Final data set for analysis: 651 patients 4/11/2020 Outcomes of Interest Patient hospital length of stay – proxy for cost Sample mean = 3.8 days (range 0-34) Mortality cases excluded due to truncation Skewed distribution; 90% of patients hospitalized 6 days or fewer Logarithmic function used in analysis Patient in-hospital mortality – proxy for quality Sample mean = 3.2% 21 deaths in sample 4/11/2020 Data Structure Patient i Patient i Community Hospital j Patient i etc. Community Hospital j Community Hospital j etc. i = 1, … 651 4/11/2020 j = 1, … 27 MHI Process Description 0. Pt arrives at CHosp 1. EKG started 2. Transport called 3. Transport arrives 4. Pt departs CHosp 5. Pt arrives at MHI 6. Pt arrives at Cath Lab 7. Procedure begins 8. Normal blood flow 4/11/2020 Interval 1: arrive → EKG 2: EKG → call 3: call → arrive 4: arrive→depart 5: depart →MHI 6: MHI →Lab 7: Lab → begin 8: begin → flow CHosp Transpt MHI Independent Variables: HospitalLevel From ‘Know what’ to ‘Do what’ Proportion of 4 drugs given From ‘Know how’ to ‘Do how’ Hospital median time intervals 4/11/2020 Independent Variables: PatientLevel From ‘Know what’ to ‘Do what’ Proportion of 4 drugs given From ‘Know how’ to ‘Do how’ Difference from hospital median time intervals • Reduces multi-collinearity • Keeps VIFs below 2.0 Patient Interval 1ij 4/11/2020 = Median Hospital Interval 1j - Patient Raw Minutes Interval 1ij Control Factors – Patient Characteristics Systolic blood pressure Age Heart rate Killip class 4 Killip class 3 Killip class 2 4/11/2020 Hypercholesterolemia Diabetes Hypertension Prior congestive heart failure Anterior MI Regression Model: Length of Stay Baseline with control factors: ln(length of stay)ij = β0 + β1-3[Patient risk factorsij] + εij Full model: ln(length of stay)ij = β0 + β1-3[Patient risk factorsij] + β4-8[Hosp median intervalj] + β9Hosp drug scorej + β10-17[Pt intervalij] + β18Pt drug scoreij + εij 4/11/2020 Length of Stay Results Sample size Full Model Model 619 619 43.87 3.10 (p<.001) (p<.001) R2 0.18 0.24 Adjusted R2 0.17 0.21 F-change 4/11/2020 Baseline Hospital-Level Effects: LOS Hospital effects: Hosp median Interval 1 0.035 Hosp median Interval 2 -0.012 Hosp median Interval 3 -0.048 Hosp median Interval 4 -0.031 Hosp median Interval 5 -0.051 Hosp drug score 4/11/2020 -0.090** Patient-Level Effects: LOS Patient effects: Patient Interval 1 0.041 Patient Interval 2 -0.101*** Patient Interval 3 0.128** Patient Interval 4 0.142*** Patient Interval 5 0.014 Patient Interval 6 0.074** Patient Interval 7 -0.030 Patient Interval 8 0.031 Patient drug score -0.048 4/11/2020 Length of Stay Results Interval CHosp Transpt MHI 1 Patient ‘Do how’ 2 ? EKG → call transport 3 Transport call → arrive 4 CHosp → transport handoff 5 6 7 8 Hospital ‘Do what’ Drug score 4/11/2020 Transport → MHI handoff Logistic Regression: Mortality Results Sample size Full Model Model 651 651 63.32 31.37 (p < .001) (p < .01) Nagelkerke R2 0.09 0.14 Cox & Snell R2 0.37 0.55 Chi-square - change 4/11/2020 Baseline Hospital-Level Effects: Mortality Hospital effects: Hosp median Interval 1 0.554* Hosp median Interval 2 -0.470** Hosp median Interval 3 -0.122 Hosp median Interval 4 -1.013 Hosp median Interval 5 -0.064 Hosp drug score 1.718 4/11/2020 Patient-Level Effects: Mortality Patient effects: Patient Interval 1 0.004 Patient Interval 2 -0.005 Patient Interval 3 0.001 Patient Interval 4 0.011 Patient Interval 5 -0.110* Patient Interval 6 0.068** Patient Interval 7 0.126 Patient Interval 8 -0.014 Patient drug score -3.753 4/11/2020 Mortality Results Interval Hospital 1 ‘Do how’ 2 CHosp Transpt MHI Arrive CHosp → EKG EKG → call transport ? 3 4 Patient 5 ‘Do how’ 6 7 8 4/11/2020 ? Depart CHosp → arrive MHI Transport → MHI handoff Conclusions Is the impact of variability in task activity on process performance (cost, quality) observable? Length of Stay Mortality Hospital ‘Do what’ Drug score 1 2 3 4 5 6 7 8 4/11/2020 1 2 3 4 5 6 7 8 Conclusions What is the relative importance of hospital-level versus patient-level task activity in predicting performance? Length of Stay Mortality Hospital ‘Do what’ Drug score 1 2 3 4 5 6 7 8 4/11/2020 1 2 3 4 5 6 7 8 Conclusions What are the impact of process handoffs? Length of Stay Mortality Hospital ‘Do what’ Drug score 1 2 3 4 5 6 7 8 4/11/2020 1 2 3 4 5 6 7 8 Conclusions In practice… Length of Stay Mortality Hospital ‘Do what’ Drug score 1 2 3 4 5 6 7 8 4/11/2020 1 2 3 4 5 6 7 8