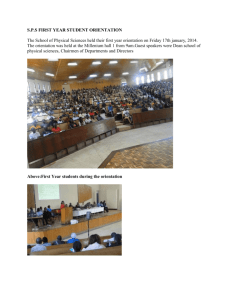
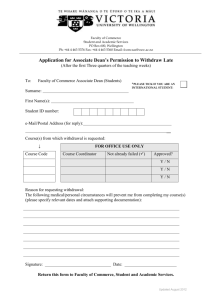
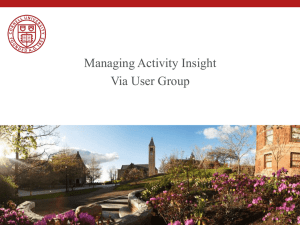
Resident Program Directors' Assessment of 2006 Graduates
advertisement

SOURCES OF OUTCOME DATA • Internal measures – End of course & clerkship surveys – End of year surveys – Faculty survey – Universal Student Rating of Instruction (USRI) – Certifying exam scores – Canadian Graduate Questionnaire • External measures – MCC – Resident program directors’ evaluation of graduates – NBME-Comprehensive Basic Science Exam – CaRMs – Alumni – LCME report – Alberta Universities/Colleges Graduate Employment Survey A Jones, Associate Dean – University of Calgary Overall Rating of First Year Courses Excellent 5 4.5 V.Good 4 3.5 Good 3 2.5 Fair 2 1.5 Poor 1 POM 2000 Blood 2001 MSK 2002 CV Resp 2003 Renal 2004 Endo 2005 Integr 2006 RMEBM 2007 Mean Scores on Certifying Evaluations (System Courses-Yr 1; SB vs CP) 85 Mean Score 80 75 SB (93-96) CP (97-07) 70 65 60 POM Blood MSK Card Resp Renal A Jones, Associate Dean – University of Calgary Endo Mean Scores on Certifying Evaluations (System Courses-Yr 2; SB vs. CP) 85 Mean Score 80 75 SB (93-96) CP (97-06) 70 65 60 Neuro Mind Repro A Jones, Associate Dean – University of Calgary GI ALBERTA LEARNING GRADUATE EMPLOYMENT SURVEY 2004 GRADUATES FROM 2002 MEDICINE Usefulness of Your Education in Achieving: • Research Skills • Working with Others • A Desire to Learn More93% • Learn Independently 97% • Awareness of Ethical Issues 97% 80% 97% A Jones, Associate Dean – University of Calgary ALBERTA LEARNING GRADUATE EMPLOYMENT SURVEY 2004 GRADUATES FROM 2002 MEDICINE • Satisfaction with the quality of teaching in your program? 100% • Satisfaction with overall quality of your educational experience 100% • University of Alberta 83% A Jones, Associate Dean – University of Calgary ALBERTA LEARNING GRADUATE EMPLOYMENT SURVEY 2004 GRADUATES FROM 2002 MEDICINE • I would recommend the same program of study to someone else. • Satisfaction with Relevance of Courses 100% 96% A Jones, Associate Dean – University of Calgary Overall Quality of Education at U of C by Faculty: % Satisfied or Very Satisfied 100 90 80 70 60 50 40 30 20 10 0 FA HU SS CC SC HA ED KN EN NU SW LA MD Data Source: 2002 Alberta Universities/Colleges’ Graduate Employment Survey re: 2000 Grads Strongly Agree Agree 5 4.5 4 3.5 No Opinion U of C 05 All Schools 05 3 2.5 Disagree 2 1.5 Strongly Disagree 1 1 2 3 4 5 6 1: I am confident that I have acquired the clinical skills required to begin a residency program 2. I have the communication skills necessary to interact with patients and health professionals 3. I have basic skills in clinical decision making and the application of evidence based information to medical practice 4. I have the fundamental understanding of the issues in social sciences of medicine 5. I have the ethical and professional values that are expected of the profession 6. I have the fundamental understanding of the basic disease mechanisms, clinical presentations and principles of diagnosis and management for common conditions Data Source: Canadian Graduate Questionnaire 2005 “I AM SATISFIED WITH THE QUALITY OF MY MEDICAL EDUCATION” 70 60 Percent 50 U of C 03 All Achools 03 U of C 04 All Schools 04 U of C 05 All Schools 05 40 30 20 10 0 Strongly Agree Agree No Opinion Disagree Strongly Disagree A Jones, Associate Dean – University of Calgary Data Source: Canadian Graduate Questionnaire 2003, 2004 & 2005 MCC TOTAL SCORE: 1992-2005 580 Mean Total Score 560 540 520 U of C Canadian 500 480 460 440 92 93 94 95 96 97 98 99 0 1 2 3 Class A Jones, Associate Dean – University of Calgary 4 5 Performance on national exams Performance on LMCC – Clinical Reasoning: 1994-2002 560 550 Mean Score 540 530 520 U of C Canadian 510 500 490 480 470 94 95 96 97 98 99 0 1 Class A Jones, Associate Dean – University of Calgary 2 720 – U of C 888 - Canadian Grads/Canadian Trained A Jones, Associate Dean – University of Calgary 328 – U of C 111 - Canadian Grads/Canadian Trained MCC Subscale & Final Scores– Class 2003 Canadian (84), International Students (7), Total (91) 560 540 520 Mean Score 500 480 U of C Can International 460 U of C Total MCC Mean 440 420 400 380 360 Cleo Med O & G Peds Phello Psy Surg MCQ CRS A Jones, Associate Dean – University of Calgary Final Percent CaRMS: PERCENT OF MATCHED STUDENTS MATCHING TO FIRST CHOICE DISCIPLINE IN 1ST ITERATION CLASSES 2001- 2005 100 95 90 85 80 75 70 65 60 55 50 Mem Dal McG Ott Qu 1 TO 2 McM 3 4 West Man Sk AB Cal BC 5 A Jones, Associate Dean – University of Calgary Data Source: CaRMS RESIDENT DIRECTORS’ ASSESSMENT OF GRADUATES (PGY1) “Overall Performance - ability to function as a resident with a full workload” 100 90 80 Percent 70 64 62 60 62 60 56 50 44 40 32 30 37 32 40 20 10 6 4 1 0 2000 2001 Weaker than most 2002 Similar to most residents 2003 2004 Stronger than most Class 2000 N = 50 (71%); Class 2001 N = 45 (68%) Class 2002 N = 40 (57%); Class 2003 N = 79(90%) Class 2004 N = 76 (82%) A Jones, Associate Dean – University of Calgary Data Source: Program Directors’ Survey Cl in ic al an ag em en t Pr of Sk es ill si s on al De m ea Hu no m ur an is tic Q ua lit Pr ie s es en ta tio n Sk ill s Se lfAw Ps ar en yc es ho s so ci al Se ns iti Pe vi rfo ty rm an ce O ve ra ll Pa tie nt M Ju dg m en t Cl in ic al Kn ow le dg e 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% M ed ic al Percent Resident Program Directors’ Assessment of 2006 Graduates Weaker Similar Stronger Data Source: Program Directors Survey A Jones, Associate Dean – University of Calgary Resident Program Directors’ Assessment of 2005 Graduates 100% 90% 80% 60% 50% 40% 30% 20% 10% an ce O ve ra ll vi ty oc ia l os Ps yc h Pe rfo rm Se ns iti es s w ar en Se lfA n nt at io st ic an i al Hu m Similar Sk ill s ie s Q ua lit ea no De m ic al Pr of es si on Cl in Weaker Pr es e ur s Sk ill en t an ag em M Pa tie nt ic al Cl in ed i ca lK no Ju d w le d ge gm en t 0% M Percent 70% Stronger Data Source: Program Directors Survey A Jones, Associate Dean – University of Calgary Resident Program Directors’ Assessment of 2004 Graduates 100% 90% 80% 60% 50% 40% 30% 20% 10% an ce O ve ra ll vi ty oc ia l os Ps yc h Pe rfo rm Se ns iti es s w ar en Se lfA n nt at io st ic an i al Hu m Similar Sk ill s ie s Q ua lit ea no De m ic al Pr of es si on Cl in Weaker Pr es e ur s Sk ill en t an ag em M Pa tie nt ic al Cl in ed i ca lK no Ju d w le d ge gm en t 0% M Percent 70% Stronger Data Source: Program Directors Survey A Jones, Associate Dean – University of Calgary UNDERGRADUATE MEDICAL EDUCATION ALUMNI SURVEY CLASSES of 1992-2002 A Jones, Associate Dean OVERALL OPINION OF THE UNDERGRADUATE MEDICAL EDUCATION PROGRAM ALUMNI SURVEY CLASSES 1992-2002 • 97% Satisfaction with the UME program at University of Calgary • 90% Felt prepared or very prepared for Post Graduate Training • 98% Would advise their child or child of a relative or friend interested in Medicine to apply to the University of Calgary A Jones, Associate Dean – University of Calgary OPNION OF ALUMNI 1992 – 2002 CURRICULUM STRENGTHS AND WEAKNESSES Instruction Strength Neither Strength or Weakness Bedside Clinical Correlation 92% 8% 88% 11% Small Group Problem Solving 86% 12% Classroom Patient Presentation 83% 15% Learning Experiences Appropriate to Educational Objectives 80% 18% Lectures 63% 31% Integration of Basic and Clinical Sciences 53% 33% Clinical Instruction Overall Why Curriculum renewal is Important “A curriculum is like water. It has the tendency to seek the lowest level of energy it can reach, and without constant renewal, it will stagnate and become putrid. To avoid stagnation alone is justification for action.” Acad Medicine Sept 1998 A Jones, Associate Dean – University of Calgary Barriers to Medical School Curriculum Changes Listed by North American Academic Deans: • • • • • Already crowded curriculum Inadequate funding Faculty resistance Professional ‘turf’ issues Scheduling conflicts Graber et al. Acad Medicine 1997 A Jones, Associate Dean – University of Calgary Curriculum – A Planned Educational Experience • Define the outcome measures. • Create an evaluation system to be sure these outcomes are realized. • Develop the pathways to get to these outcomes. Allan R Jones, MD FRCPC, Associate Dean, Undergraduate Medical Education Goals for a Revised Curriculum A revised curriculum has to be consistent with available information on clinical problem solving and reflect basic principles of adult learning. A Jones, Associate Dean – University of Calgary Medical students don’t remember or can’t use the knowledge they learned in the traditional basic science courses because the knowledge is structured into mental organizations that are not useful in the clinic Barrows, 1985 A Jones, Associate Dean – University of Calgary Problem Based Learning – Benefits • • • • • Activate prior knowledge Learn in context of clinical problem Interest in learning stimulated Self directed learning encouraged Life long learning encouraged Schmidt - Norman A Jones, Associate Dean – University of Calgary Problem Based Learning Concerns • • • • Problem solving skills are not augmented Significant gaps in knowledge occur Incorrect integration of basic sciences Tendency to engage in backward reasoning Albanese; Mitchell Academic Medicine A Jones, Associate Dean – University of Calgary Clinical Reasoning • Clinical Reasoning and clinical knowledge are interdependent. • Effective problem solving requires a large store of relevant knowledge. • Clinical expertise is linked to depth and organization of clinical knowledge. A Jones, Associate Dean – University of Calgary Problem Solving Skills In Medicine Research has proven that experts in specific domains learn knowledge and problem solving skills for each problem simultaneously. That is, knowledge acquisition and clinical reasoning go hand-in-hand. Schmidt et al 1992 Efforts to Help Students Improve Clinical Reasoning Education must focus on the development of adequate knowledge structures. Teaching, coaching, supervising must strongly encourage and nurture actual knowledge organization of the students. Knowledge keeps no better than fish Alfred North Whitehead 1929 Clinical Reasoning and Small Group Cases It is useful to select one model of clinical reasoning and base the tutorial discussion on it. The precise model is less important than its generic use as a framework to structure the flow of discussion. It later serves as a fall-back strategy in complicated clinical situations. Structure of Medical Knowledge in Memory Categories and Prototypes Both medical textbooks and classroom teaching abound in the limitless presentation of detailed lists of disorders. More often, both fail to provide a categorization scheme that is best suited for their retrieval in a clinical problem solving situation. Bordage Med Educ 1984 Types of Curricula • • • • Disciplinary Systems-based Problem-oriented Clinical Presentations based Clinical Presentation Curriculum Faculty Identify Identify Represented by Clinical Presentation Core Competencies for Clinical Presentation Curriculum Committee Develop Schematic Problem Solving Pathway For the Process of Enabling Basic Science Objectives Terminal Objectives Plans and Monitors Curriculum Course Content Together Represent Teaching Methods Clinical Reasoning Graduation Competencies Guidelines for Learning Content Evaluation Steps in Development and Dissemination of Clinical Presentation Objectives 1. Selection of clinical problem. 2. Classification system developed to help organize knowledge needed to solve the clinical problem. 3. Key Features; Discriminating features identified of prototypic prevalent disorders. Steps in Development and Dissemination of Clinical Presentation Objectives 4. Objectives and problem solving schemes developed. 5. Distribution to Faculty for balanced input from teachers generalists, specialists, and biomedical scientists. 6. Endorsements of objectives. Steps in Development and Dissemination of Clinical Presentation Objectives 7. Dissemination of objectives. 8. Encouragement of implementation of objectives in teaching, learning, clinical practice and problem solving 9. Monitor and evaluate the translation of objectives and problem solving schemes into practice. Clinical Reasoning Student Identifies Clinical Presentation Broad Classification of Problem Schematic Problem Solving Pathway Identify Causal Alternatives and Discriminating Key Factors Differential Diagnosis Diagnosis Management Plan The Scheme • Causal Categories - pre, post and renal causes of acute renal failure • Diagnoses - specific diagnoses for each causal category • Basic sciences - Integral part - Timely presentation of content “Ask any physician of 20 years standing how he has become proficient in his art and he will reply, by constant contact with disease; and he will add that the medicine he learned in schools was totally different from the medicine he learned at the bedside.” Wm. Osler 1932 Bleeding Tendency/Bruising Hx PE DDx Invest. NatHx Mgmt General Objectives Thrombocytopenia Disordered Platelet Function Congenital Coagulation Disorders Acquired Coagulation Disorders Vascular Abnormalities W Surgery Student U Radiology T Psychiatry S Physiology R Pharmacology Q Pediatrics O Pathology Oncology V a N M Office of Medical Education/Informatics/Culture, Health and Illness L Office of Medical Bioethics K Obstetrics & Gynecology J Neuroscience I Microbiology H Medicine G Immunology F Genetics E Family Medicine D Community Health Sciences/Nutrition/Prevention C Biochemistry B Anesthesia A Anatomy Natural History, Prevention, Bleeding Physical Differential Prognosis & Treatment & History Investigation Tendency/ Examination Diagnosis Complications Complications Bruising of Condition of Treatment b General Objectives c Thrombocytopenia d Disordered Platelet Function e Congenital Coagulation Disorders f Acquired Coagulation Disorders g Vascular Abnormalities 0 1 2 3 4 5 6 Schematic Problem Solving Pathway Clinical Presentations Bleeding Tendency/ Bruising Platelets Decreased Number Abnormal Function Coagulation Congenital Acquired Vascular Congenital Acquired Broad Classification of Problem Causal Alternatives and Discriminating Key Factors Differential Diagnosis Pharmacology (ASA, Heparin) Histology (Bone Marrow) Anatomy (Spleen) Basic Science Objectives for Bruising and Bleeding Genetics (Hemophilia) Physiology (Hemophilia) Pathology Immunology (Vessels) (ITP, Vasculitis) Basic Science or Biomedical Knowledge in the Undergraduate Program The purpose of basic science teaching is to provide a scientific foundation for tasks of clinical practice such as diagnosis and therapeutics. The essential challenge of balancing depth of understanding with breadth of coverage remains. (See p. 35, Fig. 4.1) W Surgery Student U Radiology T Psychiatry S Physiology R Pharmacology Q Pediatrics O Pathology Oncology V a N M Office of Medical Education/Informatics/Culture, Health and Illness L Office of Medical Bioethics K Obstetrics & Gynecology J Neuroscience I Microbiology H Medicine G Immunology F Genetics E Family Medicine D Community Health Sciences/Nutrition/Prevention C Biochemistry B Anesthesia A Anatomy Natural History, Prevention, Bleeding Physical Differential Prognosis & Treatment & History Investigation Tendency/ Examination Diagnosis Complications Complications Bruising of Condition of Treatment b General Objectives c Thrombocytopenia d Disordered Platelet Function e Congenital Coagulation Disorders f Acquired Coagulation Disorders g Vascular Abnormalities 0 1 2 3 4 5 6 Fever Fever < 2 weeks > 2 weeks Infectious Bacterial Viral ACUTE VISUAL LOSS PreRetinal • Corneal edema (glaucoma) • Vitreous hemorrhage (Diabetes) Retinal • Acute Macular Lesion (hemorrhage) • Retinal Detachment (spontaneous) • Retinal Artery Occlusion (carotid emboli) Post Retinal • Optic Neuritis (MS) • Ischemic Optic Neuropathy (Temp. Arteritis) • Occipital Infarction/Hemorrhage Chrichton, Verstraton, Fletcher Fluctuating Altered Cognition Delirium and Confusional States In the Head •CNS Infections •Seizures •Hypertensive Enceph •Psychiatric Disorders Out of the Head •Toxins •Metabolic Derangements •Systemic Organ Failure •Physical Disorders Strengths of Year I-II Curriculum • Approaches to problem solving – clinical reasoning • Early clinical exposure • Small group teaching • Clinical correlation; patient presentations • Basic science integration with problem solving • IST • Medicine 440; elective time • Communication; physical examination Allan R Jones, MD FRCPC, Associate Dean, Undergraduate Medical Education Weakness of Year I-II Curriculum • Exams not always reflective of teaching ‘emphasis’ • Lack of pharmacology • Faculty not promoting core documents; teaching to objectives not always clear • Small group teaching variable • Problem solving with schemes course dependent Allan R Jones, MD FRCPC, Associate Dean, Undergraduate Medical Education The Curriculum First Year Courses Aug Jan.2 Oct Nov Dec 19 P FOR MBlood-GI (Course I) MSKDermOpthENT (Course II) H O L I D A Y 2 w ks CVRESP (Course III) Mar. 26 Mar. 29 RenalEndocrine (includes Obesity P for M) (Course IV) June -July 18 H O L I D A Y 2 w k s E L E C T I V E 2wk s MEDICAL SKILLS PROGRAM RMEBM-Health Promotions-Disease Prevention-Population Health Number of weeks for First Year = 45 weeks A Jones, Associate Dean R E W R I T E S The Curriculum Second Year Courses July 18 E L E C T I V E 4 wks Aug. 18 NeuroscienceAging (Course V) Oct. 10 XMAS H O L I D A Y Infant-ChildReproductionGenetics (Course VI) 2 wks A Jones, Associate Dean Jan. 3 MindFamily (Course VII) Feb. 6 Mar. 5 Integrative Course Introduction to Clerkship Teaching Methods • Lectures for rapid acquisition of key content • Small group case based learning - In depth self-directed (or guided) learning - Review, reinforcement, practice and feedback - Problem solving, motivation, pertinence • Clinical correlation - Bedside sessions Clinical Reasoning Clinical reasoning does not develop in isolation: it is associated with increasingly refined and elaborated medical knowledge. Problem solving is domain-specific and not generic, so the challenge for medical educators is not only to make explicit the process of reasoning but also to identify the necessary content. Schmidt et al 1990 Kassirer 1995 Usual Sequence of Instruction • Presentation and scheme shown - Case based or otherwise • Lectures or PBL sessions planned - In depth knowledge and acquisition - Basic and clinical sciences • Small group sessions for reinforcement - Shorter case scenarios for review - Clinical correlation Advantages of New Curricular Structure Curriculum • Courses will be linked to graduation objectives and UME program philosophy of teaching, learning and evaluation. • Linkage of courses will integrate CP better and reduce redundancies. Task Force Report Advantages of New Curricular Structure Curriculum • Clinical presentation list will be revisited and clerkships will adopt appropriate presentations. Task Force Report Scheme Use Reported by First & Second Year Students (Classes of 2007 and 2006) Strongly Agree 5 4.5 4 3.5 Neutral 3 2.5 2 1.5 Strongly Disagree 1 Learning Prob-Solving 1st Yr Often Referred 2nd Yr Integration Data Source: Classes 07 & 06 yr end CP curriculum evaluation MAP OF DEPARTMENT INVOLVEMENT IN UME CURRICULUM* COURSES IN YEARS I AND II Department I II III IV HPOP V Medicine X X X X X X Family Med X Pediatrics X X X VI Int. Intro Clerk MedSkills X X X X X X X X ? Psychiatry Surgery X X X X Neurosci Anatomy X Oncology X X X X X X X X ? X X X X X Medical Genetics Anesthesia X X Community Health ER X X X Obst-Gyn Pathology VII X X X X X X X X NUMBER OF HOURS TAUGHT IN THE UNDERGRADUATE MEDICAL PROGRAM YEARS I-II GFT and CLINICAL FACULTY Hours Relative Dept Size Average Teaching hrs per Member Medicine 1844 7 Family Med 1189 7 Pediatrics 694 5 Neuroscience 514 8 Psychiatry 458 4 Surgery 437 3 Pathology 257 4 Anatomy 252 10* Oncology 242 3 Obst-Gyn 155 6 Com Health 78 1 Med Genetics 51 4 LEARNING METHODS USED DURING YEARS I AND II UNIVERSITY OF CALGARY UNDERGRADUATE PROGRAM Small Groups/Bedside: 1/3 Large Groups/Classroom: 1/3 Self Directed Study: 1/3 A Jones, Associate Dean SUMMARY OF STRUCTURED TEACHING HOURS UNDERGRADUATE MEDICAL EDUCATION PROGRAM YEARS I AND II 2004-2005 Hours % Non-GFT 5316 68 GFT 2453 32 TOTAL 7769 100 *Medicine 440, Summer Elective not included A Jones, Associate Dean Ownership of the Curriculum "Faculty members own what is taught in the curriculum - they own the content. The Associate Dean and Curriculum Committee are responsible for the methods and the effectiveness. Faculty give the course, the Associate Dean has to give the degree.” Academic Medicine Vol. 73, Pg. 54 The Seven Most Dangerous Words in Medical Education “…but we’ve always done it this way” Allan R Jones, MD FRCPC, Associate Dean, Undergraduate Medical Education Prototype Timeline for a Major Educational Change 1. Decide what to do. 2. Build support for the idea. 3. Acquire resources. 4. Do it wrong the first time. 5. Do it wrong the second time. 6. Do it passably the third time. 7. Do it reasonably well the fourth time. Friedman Acad Medicine 1993