Application for Associate Dean's Permission to Withdraw Late
advertisement

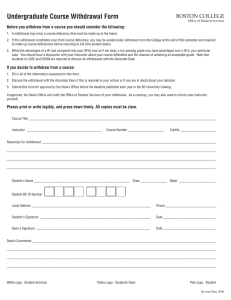
Faculty of Commerce Student and Academic Services PO Box 600, Wellington Ph: +64 4 463 5376 Fax: +64 4 463 5360 Email: fcom-sas@vuw.ac.nz Application for Associate Dean’s Permission to Withdraw Late (After the first Three quarters of the teaching weeks) To: Faculty of Commerce Associate Dean (Students) *PLEASE TICK IF YOU ARE AN INTERNATIONAL STUDENT: Surname: First Name(s): Student ID number: e-Mail/Postal Address (for reply): __ Course(s) from which withdrawal is requested: ↓ Course Code FOR OFFICE USE ONLY Course Coordinator Not already failed () Approved? Y/N Y/N Y/N Reason for requesting withdrawal: The following medical/personal circumstances will prevent me from completing my course(s) (please specify relevant dates and attach supporting documentation): Signature: Date: Return this form to Faculty of Commerce, Student and Academic Services. Updated August 2012