13-The anal triangle2008-03
advertisement

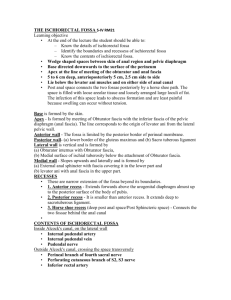
The Perineum The Perineum It is the region of the trunk inferior to the pelvic diaphragm (levator ani & coccygei) The Perineum In anatomical position it is a narrow area between the thighs When the thighs are abducted, it is a diamond-shaped area extending from pubic symphysis to the tip of the coccyx Boundaries of the Perineum Perineum is bounded by: Pubic symphysis Inferior pubic rami Ischial rami Ischial tuberosities Sacrotuberous ligaments Coccyx Divisions of the Perineum For descriptive purposes, divided by an imaginary transverse line joining the anterior ends of the ischial tuberosities, into two unequal triangles: Urogenital triangle anteriorly Anal triangle posteriorly The Anal Triangle Bounded: Anteriorly: by the imaginary line Behind: by the tip of coccyx On each side: by the ischial tuberosity and the sacrotuberous ligament Overlapped by the border of the gluteus maximus muscles Contains: anal canal, external anal sphincter & ischiorectal (ischioanal) fossa The Anal Triangle cont’d The perianal skin is: Pigmented Has many sweat and sebaceous glands Is thrown into folds Is supplied by inferior rectal nerve and vessels Its lymphatics drain into medial group of superficial inguinal lymph nodes The Anal Canal About 4cm long Passes downward and backward from the rectal ampulla (at the level of the sling formed by the puborectalis) to the anus Remains contracted and forms an antero-posterior slit, except during defecation The walls are kept in apposition by the levator ani muscle and the anal sphincter The Anal Canal: Relations Anteriorly: Perineal body Urogenital diaphragm Membranous urethra & bulb of penis in male, and lower part of vagina in female Posteriorly: Anococcygeal body Laterally: Ischiorectal fossa The Anal Canal: Origin Embryologically the anal canal is developed from two sources: • Upper half is derived from hindgut • Lower half is derived from the proctodeum The junction of the two parts is indicated by the pectinate line The part of anal canal superior to pectinate line differs from the part inferior to pectinate line in its: • Epithelial lining • Arterial supply • Venous drainage • Innervation • Lymph drainage The white line (below the pectinate line) indicates the site of mucocutaneous jnction Mucous Membrane Upper Half Lined by columnar epithelium Thrown into vertical folds called anal columns, which are joined together at lower ends by semilunar folds called anal valves (semilunar folds are remnants of the anal membrane) Lower Half: Lined by stratified squamous epithelium No columns Muscles Two distinct layers: outer longitudinal & inner circular layer of smooth muscle Thickening of the smooth muscles of the circular layer at the upper end of anal canal forms the involuntary internal sphincter The internal sphincter is enclosed by a sheath of skeletal muscle that forms the voluntary external sphincter External Anal Sphincter Voluntary Composed of skeletal muscle Surrounds the inferior 2/3rd of anal canal Divided into three parts: Subcutaneous part: encircles the lower end of the anal canal, has no bony attachment Superficial part: attached to perineal body anteriorly, and coccyx posteriorly Deep part: encircles the upper end of the anal canal, has no bony attachment Anorectal Ring A distinct muscular ring formed at the junction of rectum and anal canal Formed by the internal sphincter, deep part of the external sphincter and the puborectalis Can be felt at rectal examination Helps in increasing the anorectal angle Blood Supply Arteries: Upper half: superior rectal artery (continuation of the inferior mesenteric artery) Lower half: inferior rectal artery Venous Drainage: Upper half: superior rectal vein drained into the inferior mesenteric vein Lower half: inferior rectal vein drained into the internal pudendal vein • Important site of portal-systemic anastomosis Nerve Supply Mucous membrane Upper half: Sensitive only to stretching Supplied by inferior hypogastric plexus Lower half: Sensitive to pain, temperature, touch and pressure Supplied by inferior rectal nerve Involuntary internal sphincter supplied by inferior hypogastric plexus (sympathetic) & pelvic splanchnic nerves (parasympathetic) Voluntary external sphincter supplied by inferior rectal nerve (branch of internal pudendal nerve) and peineal branch of the S4 nerve Lymphatic Drainage Upper half: pararectal nodes & then to inferior mesenteric lymph nodes Lower half: medial group of the superficial lymph nodes The Ischiorectal Fossa Ischiorectal Fossa A large fascia-lined wedge-shaped space on each side of the anal canal Located between the skin of the anal region and the pelvic diaphragm The two fossae are communicated with each other behind the anal canal Ischiorectal Fossa: Boundaries Base of the wedge is superficial and formed of skin and fascia Apex lies superiorly, at the junction of medial and lateral walls Medial wall is formed by sloping levator ani muscle and the anal canal Lateral wall is formed by ischial tuberosity and the lower part of obturator internus muscle and its fascia Ischiorectal Fossa: Contents Dense fat Pudendal canal and its contents (internal pudendal vessels & nerves) Inferior rectal vessels & nerve Perforating branches of S2-S3 Perineal branch of S4 Pudendal Canal A fascial canal formed by the splitting of the obturator fascia Located on the lateral wall of the ischiorectal fossa, on the medial side of the ischial tuberosity Contains pudendal nerve and internal pudendal vessels Pudendal Nerve Branch of sacral plexus Leaves pelvic cavity through the greater sciatic foramen Enters perineum through the lesser sciatic foramen Passes forward in the pudendal canal Gives branches: Inferior rectal nerve Dorsal nerve of penis or clitorus Perineal nerve Internal Pudendal Artery Branch of Internal iliac artery Leaves pelvic cavity through the greater sciatic foramen Enters perineum through the lesser sciatic foramen Passes forward in the pudendal canal Gives branches: Inferior rectal artery Branches to penis or to clitorus and to labia Accompanied veins are tributaries of the internal pudendal vein CLINICAL NOTES Pudendal Block Pudendal nerve as it runs in the pudendal canal, is blocked by an anaesthetic to produce analgesia of the perineum in forceps delivery The anaesthetic can be injected around the nerve by: Transvaginal method Perineal method Rectal Prolapse Normally, the rectum is securely attached to the pelvis with the help of ligaments and muscles. This attachment firmly holds the rectum in place. Various factors (age, long-term constipation, the stress of childbirth) may cause these ligaments and muscles to weaken. This causes the rectum to prolapse (it slips or falls out of place) May be A. incomplete (mucosal) B. complete involving the rectal wall Hemorrhoids A condition in which the veins around the anus or lower rectum are swollen and inflamed. May result from straining to move stool, chronic constipation or diarrhea, pregnancy, aging Hemorrhoids are either inside the anus (internal) or under the skin around the anus (external). Internal Hemorrhoids Varicosities of the tributaries of superior rectal vein covered by mucous membrane Tributaries which lie in anal columns at 3, 7, 11 o’clock position are more prone to become varicosed. 3 degrees: – 1st degree: contained within the anal canal – 2nd degree: protrude out of anal canal during defecation but return back after it – 3rd degree: protrude in defecation and remain outside External Hemorrhoids Varicosities of the tributaries of inferior rectal vein covered by skin Varicosed tributaries may rupture due to coughing or straining and form a perianal hematoma in the subcutaneous tissue around anus Anal Fissure It is an elongated ulcer produced by tearing of anal valves due to passage of hard fecal mass Occurs most commonly in the midline posteriorly or anteriorly Is extremely painful condition and is usually examined under anaesthesia Anal fissure in the lower part of anal canal results in reflex spasm of external anal sphincter Perianal abcesses Produced by fecal trauma to anal mucosa May be: Submucosal Subcutaneous Pelvirectal Ischiorectal Spread or inadequate treatment of abscess may lead to the formation of anal fistula and anal sinus Ischiorectal Abscess Fossa is filled with fat Is poorly vascularized Is vulnerable to infection from anal canal Abscess of one side may spread to opposite fossa across the midline behind the anal canal