Title Goes Here - North Carolina Public Health Association
advertisement

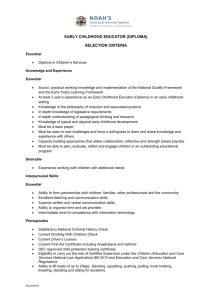
The Early Learning Challenge in North Carolina January 23, 2014 Marshall Tyson, MPH NC Division of Public Health Oscar Fleming, MSPH National Implementation Research Network Jeannine Sato Center for Child and Family Health NC Early Childhood Advisory Council Race to the Top--Early Learning Challenge (ELC) Grant Program Joint program US Dept. of Health and Human Services US Dept. of Education 37 applicants; 9 states selected, including NC NC’s award: $69,991,121.00 4-year grants—Jan. 1, 2012–Dec. 31, 2015 NC Early Childhood Advisory Council ELC Focus Bold action to improve early learning and development Supports states that demonstrate “commitment and capacity to build a statewide system that raises the quality of early learning and development programs so that all children receive the support they need to enter kindergarten ready to succeed.” NC Early Childhood Advisory Council NC’s Implementation Strategy Lead Agency: Early Childhood Advisory Council—responsible for overall coordination and specific projects Participating State Agencies—responsible for specific projects: Division of Child Development and Early Education Division of Public Health Department of Public Instruction, Office of Early Learning Contracts and MOUs with other state and local agencies and organizations, such as NC Partnership for Children and the National Implementation Research Network, FPG, UNC-CH NC Early Childhood Advisory Council NC’s Plan: Four Areas of Focus Strengthen the state’s early childhood system and build its capacity to foster positive outcomes for young children Enhance the quality of programs to serve young children and their families and improve access to high-quality programs Strengthen the early childhood workforce to increase staff and system effectiveness and sustain change Target high-intensity supports and community infrastructurebuilding efforts to turn around poor outcomes for young children in the state’s highest-need counties (Transformation Zone) NC Early Childhood Advisory Council NC’s Plan: Transformation Zone Strategy • Focus intensive effort in selected high-need counties in northeastern North Carolina • Increase capacity for effective collaboration and implementation to gain desired and sustainable results • Provide comprehensive set of services and supports offered when and where needed—existing services and selected additional services (e.g., Family Strengthening services) NC Early Childhood Advisory Council NC’s Plan: Transformation Zone Strategy • Help achieve dramatically improved outcomes for all young children • Lessons learned through concentrated approach used to hone early childhood strategies improve outcomes for young children across the state NC Early Childhood Advisory Council NC’s Transformation Zone • 17 northeastern Tier 1 counties eligible CAM-CURRITUCK ALLEGATES NORTHWARREN DEN HERTGHANY SURRY STOKES ROCKING-CASWELL PERAMPTON PERSONGRAN-VANCE PASQUOFORD HALIFAX HAM WATAUGA WILKES QUIMANS CHO- TANK VILLE YADKIN FORSYTH ORANGE BERTIE MITCHELL FRANKLIN GUILFORD AVERY WAN YANNASH EDGECALDWELLALEXALADURHAM DAVIE MADISON CEY WASHANDERIREDELL DAVIDMANCE MARTIN COMBE TYRELL DARE WAKE INGTON WILSON SON RANDOLPHCHATHAM BUN- McDowellBURKE CATAWBA HAYBEAUPITT ROWAN SWAIN WOOD COMBE HYDE JOHNSTON FORT LINCOLN GREENE RUTHERLEE GRAHAM HENDERCABARRUS JACKWAYNE FORD CLEVE- GASTON HARNETT MONTTRANLENOIR MOORE SON POLK STANLY CHEROKEE MACON SON CRAVEN PAMLAND GOMERY MECKLENSYLVANIA CLAY BURG LICO JONES SAMPSON CUMBERRICHHOKE DUPLIN UNION ANSON LAND MONDSCOTCARTERET ONSLOW LAND ROBESON BLADEN PENDER ASHE NEW HANOVER BRUNSWICK COLUMBUS • After exploration and RFA process, 4 counties selected: Beaufort Chowan Bertie Hyde NC Early Childhood Advisory Council NC’s Transformation Zone Three streams of work in Northeast • Statewide projects • Transformation Zone projects and activities (4 counties) • Additional work in 15 surrounding counties 13 counties which were eligible through the grant Nash and Pitt--closely linked to those 13 counties; home to many services Division of Public Health projects Family strengthening Family Connects Triple P (Positive Parenting Program) NC Early Childhood Advisory Council Family Connects (A.k.a. NorthEast Connects Family Connects Oscar Fleming Use of implementation science principles Jeannine Sato Replicating the Durham Connects model as Family Connects in the TZ NC Early Childhood Advisory Council An Overview of the Active Implementation Frameworks Applied Implementation Science State Health Directors Conference January 23rd, 2014 Oscar Fleming National Implementation Research Network FPG Child Development Institute University of North Carolina at Chapel Hill Agenda • Introduction/Purpose • Why Focus on Implementation? (5) • What are the Active Implementation Frameworks (15) • Fidelity and Outcomes Why Focus on Implementation? “Children and families cannot benefit from interventions they do not experience.” RESEARCH IMPLEMENTATION PRACTICE Active Implementation is defined as a specified set of activities designed to put into practice an activity or program of known dimensions. Formula For Success Effective Interventions Effective Implementation Socially Significant Outcomes Enabling Contexts Active Implementation Applied Implementation Science To effectively implement & realize the benefit of evidencebased and evidence-informed interventions, we need to know: • WHAT to do What is the usable intervention or package of strategies? (e.g. evidence-based home visitation programs) • HOW to do it Active and effective implementation and sustainability frameworks (e.g. strategies build competencies and create enabling contexts and conditions) • WHO will do it Organized, purposeful, & active implementation support from linked implementation teams Active Implementation Frameworks: The “What” The effective interventions and approaches that will improve outcomes for children, youth and families. Usable Intervention Criteria Clear description of the program Philosophy, values, principles (guidance) Inclusion – exclusion criteria (beneficiaries) Clear essential functions that define the program (core components) Operational definitions of essential functions (practice profiles; do, say) Practical performance assessment Highly correlated with desired outcomes Active Implementation Frameworks: Making It Happen The “How” • Implementation Drivers result in competence and sustainability • Improvement cycles support learning and change at multiple levels • Stage-related work necessary for successful change Implementation Drivers Reliable Benefits Consistent Uses of Innovations Performance Assessment (Fidelity) Systems Intervention Coaching Training Integrated & Integrated Compensatory & Selection Facilitative Administration Compensatory Leadership Drivers Technical Adaptive Decision Support Data System Improvement Cycles Rapid cycle (PDSA) problem solving Shewhart (1931); Deming (1986) Usability testing Rubin (1994); Nielsen (2000) Practice-policy communication loop Fixsen, Blase, Metz, & Van Dyke (2013) Implementation Stages Exploration • • • • Assess needs Examine intervention components Consider Implementation Drivers Assess fit Installation • • • • Acquire Resources Prepare Organization Prepare Implementation Drivers Prepare staff Initial Implementation • • • • 2-4 Years Strengthen Implementation Drivers Manage change Activate Data Systems Initiate Improvement Cycles Full Implementation • • Monitor & manage Implementation Drivers Achieve and improve Fidelity and Outcomes Active Implementation Frameworks: The “Who” Implementation Teams with specific competencies “make it happen” Minimum of three people with expertise in: Innovations Implementation Improvement Cycles Organization change Implementation Stages • Why Teams? – Letting it happen • Diffusion; networking; communication – Helping it happen • Dissemination; manuals; websites –Making it happen • Purposeful and proactive use of implementation practice and science Based on Hall & Hord (1987); Greenhalgh, Robert, MacFarlane, Bate, & Kyriakidou (2004); Fixsen, Blase, Duda, Naoom, & Van Dyke (2010) Implementation Teams Implementation Team Simultaneous, Multi-Level Interventions Practitioner/Staff Competence Organization/Agency Supports Management (leadership, policy) Administration (HR, structure) Supervision (nature, content) State MCH/Title V Leadership Federal and National Supports The Frameworks in Action • Eastern NC: Working with teams in Chowan, Bertie, Beaufort, Hyde counties • Purveyor Collaboration: Develop/enhance usable intervention criteria • State Agencies: Collaborative support for implementation informed policy A Final Word on Fidelity • Achieving fidelity if a shared responsibility among Providers, their Home Agency, and Program Purveyors, among others. • If the goal is worth achieving its worth spending time to build the required infrastructure • Programs like Connects that have evidence, well defined core components and operationalized essential functions make your work easier, if not easy, and significantly increase your chances for Socially Significant Outcomes. Thank You! For More Information Oscar Fleming, MSPH – 919-962-7193 – oscar.fleming@unc.edu Frank Porter Graham Child Development Institute University of North Carolina Chapel Hill, NC http://nirn.fpg.unc.edu/ www.scalingup.org www.implementationconference.org Implementation Science Implementation Research: A Synthesis of the Literature Fixsen, D. L., Naoom, S. F., Blase, K. A., Friedman, R. M. & Wallace, F. (2005). Implementation Research: A Synthesis of the Literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, The National Implementation Research Network (FMHI Publication #231). HTTP://NIRN.FPG.UNC.EDU ©Copyright Dean Fixsen and Karen Blase This content is licensed under Creative Commons license CC BYNC-ND, Attribution-NonCommercial-NoDerivs. You are free to share, copy, distribute and transmit the work under the following conditions: Attribution — You must attribute the work in the manner specified by the author or licensor (but not in any way that suggests that they endorse you or your use of the work); Noncommercial — You may not use this work for commercial purposes; No Derivative Works — You may not alter or transform this work. Any of the above conditions can be waived if you get permission from the copyright holder. http://creativecommons.org/licenses/by-nc-nd/3.0 The “CONNECTS” Home Visiting Model Improving Child Well-Being by bridging new parent needs with community resources. Growing Healthy Babies Evidence-based Universal Home Visits for Parents of Newborns NC DPH January 23, 2014 Why Universal? Newborn nurse home visits should be normalized, much the way prenatal care has become the standard of care.” – Dr. Robert Murphy, CCFH • • • • Public health approach improves community health No stigma All parents have needs (94% in research) Short term triage (gateway) to more intensive services. The Connects model Feedback loop between hospitals, doctors, service agencies to strengthen community system of care. What we do All areas correlate to empirically based risks for child abuse. Nurses: • assess • quantify needs • resolve or • refer • follow up Who’s Involved? NC Early Childhood Advisory Council FACT: 99% of mothers surveyed say their DC visit was helpful to them and their baby. Local leaders How is it Funded? • • • • State and federal grants Private foundations Medicaid reimbursement (in some cases) Local government funds Who are Stakeholders? • • • • Health departments Hospitals Primary care providers Social service agencies Impact Evaluation Results Randomized Controlled Trial at age 6-month (in-home interview results): • More community connections • More mother-reported positive parenting behaviors • Higher quality mother-infant relationship • Higher quality home environment • Higher quality child care usage • Less clinical anxiety for mother Age 12-month administrative hospital record reviews: • 85% fewer hospital overnights • 50% less total infant emergency medical care Mean Cumulative Number of Emergency Care Episodes Birth - 24-Months 3 Cumulative Emergency Care Episdoes 2.5 2 1.5 Total ED Visits: Control Families Total ED Visits: DC Families 1 0.5 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Child Age in Months • 37% less infant emergency medical care through 24-month • Significant decrease from 0-12 months; decrease sustained through 24months Rural Replication • • • • • • • Race to the Top Early Learning Challenge Multiple interventions in Transformation Zone ~ 800 births High poverty High unemployment 5 birth main hospitals, some out of county Diversity among counties (not within) The Connects Offering • Universal home visits = no stigma • A triage system for entire community • A way to strengthen system of care • Technical support and certification for high fidelity, to replicate outcomes Model Requirements • Universal reach, RN staff • Partnered hiring, training & fidelity checks with Connects for certification • Adherence to the model (documentation and performance measures) • Exclusivity in program staffing, salary and work assignments • A regional/team approach to cover population What next? • Connects is ideal for: – – – – – Expand public health gateway Strengthen systems of care Track and ID service gaps and usage Reduce child abuse Save infant ER costs • Tool kit for adoption/sustainability plan • Lessons learned during replication • Goal to serve families & replicate outcome results Jeannine Sato Program Director j.sato@duke.edu 919-668-3295 www.durhamconnects.org Questions?