Federal and State Pharmacy Law Update, May, 2015
advertisement

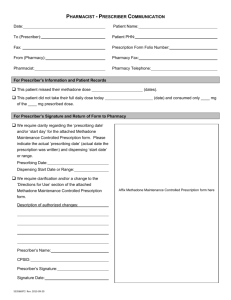
Pharmacy Law Update Jesse Vivian, RPh, JD Department of Pharmacy Practice 2144 Applebaum Direct Phone: 313-577-5389 jessevivian@wayne.edu http://jessevivian.com Detroit Medical Center April 14, 2015 Goals & Objectives Provide current information on federal and state statutes and regulations pertaining to: – Controlled Substances Prescribing, dispensing, labeling, records – Practice of Pharmacy Technicians, community & institutional – Compounding Controlled Substances Who can prescribe what from where under what circumstances? – Institutional Rules – Community Rules – Distinguish Policies, 3rd party requirements from regulations Validity of CS Scripts C-2 – 90 days from date issued – Note: No limit on number of days supply (Unless insurance posts limits 3 scripts-30 days each with next fill date No post-dating – No refills (partial fill exceptions) C-3 & 4 – 6 months from date issued – Up to 5 refills C-5 – 1 year from date issued – No limit on refills (up to one year) RPh Corresponding Responsibility The Providers Dilemma: Balancing Good Care and Gatekeeper Duties Policy Goal Find way to Maximize Legitimate Medical Use of Abusable Drugs minimal intrusion on those with need to access these drugs While Minimizing Ability of Abusers to Obtain These Drugs keep the “bad guys” off drugs “Corresponding Responsibility” 21 CFR § 1306.04: The purpose of a prescription: To be effective, the CS Rx must be issued for a legitimate medical purpose by a practitioner acting in the usual course of professional practice. The pharmacist has a “corresponding responsibility” with the prescriber for proper prescribing and dispensing. An order purporting to be a “prescription” is not a “prescription” if not issued in the usual course of professional treatment The Pharmacists Manual The dispensing pharmacist must maintain a constant vigilance against forged or altered prescriptions. The law holds the pharmacist responsible for knowingly dispensing a prescription that was not issued in the usual course of professional treatment. The Pharmacists Manual The quantity of drugs prescribed and frequency of prescriptions filled are not alone indications of fraud or improper prescribing especially if the patient is being treated with opioids for pain management. Pharmacists should also recognize that drug tolerance and physical dependence may develop as a consequence of the patient’s sustained use of opioid analgesics for the legitimate treatment of chronic pain. The Pharmacists Manual The following criteria may indicate that a prescription was not issued for a legitimate medical purpose. The prescriber writes significantly more prescriptions (or in larger quantities) compared to other practitioners in your area. The patient appears to be returning too frequently. Prescription which should last for a month in legitimate use, is being refilled on a biweekly, weekly or even a daily basis. The prescriber writes prescriptions for antagonistic drugs, such as depressants and stimulants, at the same time. Drug abusers often request prescriptions for "uppers and downers" at the same time. Patient appears presenting prescriptions written in the names of other people. A number of people appear simultaneously, or within a short time, all bearing similar prescriptions from the same physician. Numerous "strangers," people who are not regular patrons or residents of your community, suddenly show up with prescriptions from the same physician. The Pharmacists Manual 1. 2. 3. 4. 5. 6. 7. Characteristics of Forged Prescriptions Prescription looks "too good"; the prescriber’s handwriting is too legible; Quantities, directions or dosages differ from usual medical usage; Prescription does not comply with the acceptable standard abbreviations or appear to be textbook presentations; Prescription appears to be photocopied; Directions written in full with no abbreviations; Prescription written in different-color inks or written in different handwriting. Apparent erasure marks Prevention Techniques 1. 2. 3. 4. 5. 6. 7. 8. Know the prescriber and his/her signature; Know the prescriber’s DEA registration number; Know the patient; Check the date on the prescription order. Has it been presented to you in a reasonable length of time since the prescriber wrote it? When there is a question about any aspect of the prescription order, call the prescriber for verification or clarification. Should there be a discrepancy, the patient must have a plausible reason before the prescription medication is dispensed. Any time you are in doubt, require proper identification. Although this procedure isn’t foolproof (identification papers can also be stolen/forged), it does increase the drug abuser’s risk. If you believe that you have a forged, altered, or bogus prescription--don’t dispense it--call your local police. If you believe that you have discovered a pattern of prescription abuses, contact your State Board of Pharmacy or your local DEA office. Both DEA and state authorities consider retail-level diversion a priority issue. Health Care Providers’ Orientation: Health Care: taking care of patient needs to maximize “outcomes” recognizing CS Drugs have therapeutic value, pain is a legitimate disease and its treatment is necessary and appropriate “Gatekeeper” Function: keep “bad” people from getting “bad” drugs Health and Human Services Perspective: U.S. is NOT aggressive in pain control management. Fear of patient addiction and legal entanglement prevents practitioners from good pain control HHS Policy Manual February, 1992 Michigan CS Balancing Act How to insure ‘good guys’ get the CS drugs they need for legitimate medical need, But keep ‘bad guys’ from getting CS drugs for ‘wrong’ reasons The Good Faith Standard “Please Dear God, let this prescription be legitimate and valid and I promise to be your faithful servant for the rest of my life OxyContin #10,000 Legislative Intent The legislature finds that the treatment of pain is an appropriate issue for the legislature to consider, and that the citizens of this state would be well served by the enactment of legislation that accomplishes all of the following: (a) Provides more and better information to health care consumers regarding the medical treatment of pain, health care coverage and benefits for the treatment of pain, and the education of health professionals in pain and symptom management (b) Provides for the appointment of an advisory body to study and make recommendations on model core curricula on pain and symptom management for the institutions in this state providing health care education, continuing education for health professionals on pain and symptom management, and the integration of pain and symptom management into the customary practice of health care (c) Educates health professionals about the disciplinary process for state licensees and registrants, including, but not limited to, how the department of [community health] processes allegations of wrongdoing against licensees and registrants Legislative Intent (1) The legislature finds that the use of controlled substances is appropriate in the medical treatment of certain forms of pain, and that efforts to control diversion or improper administration of controlled substances should not interfere with the legitimate, medically recognized use of those controlled substances to relieve pain and suffering. (2) The legislature finds that some patients in this state with pain are unable to obtain from their health care providers sufficient pain relief through the prescription of controlled substances, especially controlled substances included in Schedule 2 under § 333.7214. (3) It is the intent of the legislature to permit and facilitate adequate treatment for pain by licensed health professionals, including, but not limited to, the prescription or dispensing of controlled substances included in Schedule 2 under section 7214, when medically appropriate, and to enable regulatory and law enforcement agencies to prevent the abuse and diversion of controlled substances by creating an electronic monitoring system. [1] §16204c Point Practitioners should avoid ‘knee-jerk’ response when confronted with treatment of pain issues – Fear of Legal Quagmire should not take priority over good pain control and patient care issues – The key is BALANCE The ‘standard of care’ is “Good Faith” Statutory ‘Good Faith’ Sec. 7333 ‘good faith’ means the prescribing or dispensing of a controlled substance by a practitioner licensed under section 7303 in the regular course of professional treatment to or for an individual who is under treatment by the practitioner for a pathology or condition other than that individual's physical or psychological dependence upon or addiction to a controlled substance, except as provided in this article.” Cf: 21 CFR § 1306.04(a) § 7333 (2) a practitioner, in good faith, may dispense a controlled substance included in schedule 2 upon receipt of a prescription of a practitioner licensed under section 7303 on a prescription form. (4) A practitioner, in good faith, may dispense a controlled substance included in schedule 3, 4, or 5 that is a prescription drug upon receipt of a prescription on a prescription form or an oral prescription of a practitioner. Good Faith Application of ‘good faith’ to a pharmacist means the dispensing of a controlled substance pursuant to a prescriber's order which, in the professional judgment of the pharmacist, is lawful ‘Good Faith’ Standards The pharmacist shall be guided by nationally accepted professional standards including, but not limited to, all of the following, in making the judgment: (a) Lack of consistency in the doctor-patient relationship. (b) Frequency of prescriptions for the same drug by 1 prescriber for larger numbers of patients. (c) Quantities beyond those normally prescribed for the same drug. (d) Unusual dosages. (e) Unusual geographic distances between patient, pharmacist, and prescriber Michigan Version of the Feds “Pharmacist Manual” Changes to face of (all) CS Scripts With agreement of Prescriber, RPh may ADD or CHANGE – patient's address, dosage form, drug strength, drug quantity, directions for use, or issue date – Note changes on script or documentation kept with script NO Change to face of CS Scripts A pharmacist shall not change the patient's name, controlled substance prescribed (unless authorized to dispense a lower cost, genericallyequivalent drug product) or the prescriber's signature with regard to a prescription. In addition, a pharmacist shall not change the "do not fill until date." Communication of CS Script to Pharmacy Hard Copy Telephone (Not for C-2 unless “emergency”—72 hour rule) Electronically – Not Fax (1 exception) FAX C-2 Scripts For a resident of a long-term care (LTC) facility – may be transmitted by the practitioner or the practitioner's agent to the dispensing pharmacy by facsimile, provided that the original manually signed prescription (by the prescriber, not the "agent") is presented to the pharmacist for review prior to the actual dispensing of the prescription. The facsimile serves as the original written prescription. LTC facilities need to have documented "agent of the prescriber" arrangements with each nurse acting as a practitioner's agent. Facilities should utilize the approved Drug Enforcement Administration "agent of the prescriber" form for each nurse with every prescriber and have these forms updated routinely per facility protocol. Delegated CS Prescribing MD & DO only allowed to delegate PA, NP, Midwife Nurse – “mid-level practitioners” – Must have own DEA Registration Name & DEA # of delegating Physician must appear on script – MD/DO not need to “co-sign” PA CS Prescribing Physician assistants (PAs) working under delegated authority of an allopathic physician (MD) and/or osteopathic physician (DO) are allowed to prescribe controlled substance prescriptions, Schedules 25, without limitations to the quantity or location of prescribing. NP CS Prescribing No limits on C-3 to C-5 Are limitations for the prescribing of Schedule 2 controlled substances – for only those patients being discharged from the hospital setting, free-standing surgical outpatient facility or hospice for a quantity of no more than a seven-day supply. – NPs cannot prescribe Schedule 2 controlled substances for their ambulatory, every day patients. SB 68 (March 16, 2015) – Some Michigan nurses would be able to prescribe drugs without a doctor’s consent. – Address physician shortages in many rural areas of the state. RPh Prescribing There is nothing in the Public Health Code that prohibits a pharmacist from prescribing a non-controlled substance under delegated authority. A pharmacist would need to identify on a prescription the name of the prescriber who granted them delegated authority to prescribe. A pharmacist, however, cannot prescribe controlled substances since a pharmacist does not have authorization by the Public Health Code or the Administrative Rules of the Boards of Medicine or Osteopathic Medicine and Surgery nor are pharmacists able to obtain a Drug Enforcement Administration (DEA) registration number. The Code of Federal Regulations prohibits a prescriber from delegating the use of their DEA registration or their signature. While pharmacists may be granted authority under delegation to prescribe non-controlled substances, patients may have problems filling these prescriptions under their prescription health insurance coverage since many health plans do not recognize nor credential pharmacist prescribers. MAPS Reporting The patient identifier The name of the controlled substance dispensed The metric quantity of the controlled substance dispensed The National Drug Code (NDC) of the controlled substance dispensed The date of issue of the prescription The date of dispensing The estimated days of supply of the controlled substance dispensed The prescription number assigned by the dispenser The DEA registration number of the prescriber and the dispensing pharmacy The Michigan license number of the dispensing pharmacy” MAPS Reporting Patient Identifiers a) b) c) Driver's license number, State-issued identification number or the number zero. – A social security number is no longer an allowable identifier. – In the case of a child or pet, all zeroes are entered. – Not required for institutional patients Tamper-Proof Prescriptions Required for Medicare Part D eligible patients – Both Rx-only and CS Scripts In Michigan, no temper proof hardcopy prescription forms required CS Copy Transfers Schedule 3-5 controlled substances may be transferred once, if the pharmacies do not electronically share them on a real-time basis. The transfer of controlled substance prescriptions must be conducted between two licensed pharmacists, whether done verbally or electronically shared on a realtime basis. CS Copy Transfers Pharmacies that electronically share on a real-time basis may transfer online up to the maximum refills permitted by law and the prescriber's authorization. A Schedule 2 controlled substance prescription may not be copied from any pharmacy. CS Copy Transfers Responsibility of the transferring pharmacist: – The pharmacist completing a transfer must write the word "VOID" on the face of the invalidated prescription. – On the back (reverse) of the invalidated prescription, the pharmacist needs to document the name, address and Drug Enforcement Administration (DEA) registration number of the pharmacy to which it was transferred to and the name of the pharmacist receiving the prescription. CS Copy Transfers Responsibility of the receiving pharmacist: – The pharmacist receiving the transfer must write the word "TRANSFER" on the face of the prescription and include all the required elements of the controlled substance prescription in addition to the date of issuance of the original prescription, the original number of refills authorized, the remaining number of refills and the date of original dispensing. – The pharmacist must also document the name of the transferring pharmacy, address, DEA number, the prescription number and the name of the transferring pharmacist. CS Scripts and Rx Techs A practitioner or the practitioner's agent may convey a prescription orally to a pharmacist (or intern), who promptly reduces to writing all information required. Techs NOT Allowed to take CS script orally “Tech check Tech” in hospitals In 1994, the Attorney General of the State of Michigan wrote a memorandum to the Bureau of Occupational and Professional Regulation (currently the Department of Community Health) regarding allowing technicians to check technicians and how it is in conflict with two statutes. Article 177 states in sections 17751(2) and 17763(a) and (b) that drugs may only be dispensed by pharmacists and those individuals specifically identified in Article 177. A pharmacist is not permitted to delegate the act of dispensing except as authorized in Article 177. However, section 16215 does provide the Board of Pharmacy authority to promulgate rules regarding delegation. Thus, according to the memorandum to allow pharmacy technicians to dispense prescription drugs in this manner, it would require the promulgation of administrative rules. To date, no rules have been promulgated. E-Scripts for CS Drugs Once the pharmacy's software has been certified to accept electronically communicated controlled substance prescriptions AND the prescribing physician's electronic prescribing system has also been certified by a Drug Enforcement Administration (DEA)-approved vendor. However, until you receive documentation from your software vendor that validates your system is compliant with the new DEA regulations you cannot receive prescriptions for controlled substances electronically, even if the prescription is written by a prescriber whose software system has been DEA certified. Once a prescription is created electronically, all records of the prescription must be retained electronically. Electronic Signature Electronically communicated prescriptions are valid with electronic signatures for noncontrolled substances and for controlled substances if the electronic prescriptions are created and signed using an application that has also been certified by a Drug Enforcement Administration (DEA)-approved vendor. The electronic signature can be a sound, symbol or process attached to the record (may or may not be a digital version of the prescriber's signature). Manual Signatures A manual signature is required on all paper prescriptions presented to the pharmacy or those prescriptions transmitted from a physician's fax machine to the pharmacy fax machine. The prescriptions may be computer-generated; – however, they must contain a manual or "wet" signature of the prescriber if they are printed out. – Electronically generated signatures on these paper or faxto-fax prescriptions are not valid. The prescriber is required to sign a written prescription in the same manner as (s)he would sign a check or legal document. Stamped Signatures are not valid Prescriptions Okay to combine CS and Non-CS on single blank (Rule 9b repealed 2014) Electronically communicated prescriptions are valid with electronic signatures for noncontrolled substances and for controlled substances if the electronic prescriptions are created and signed using an application that has also been certified by a Drug Enforcement Administration (DEA)-approved vendor. Number of Scripts on Single Hardcopy Six medications per computergenerated prescription, and a Four for a handwritten blank for noninstitutional pharmacy practice CS and Non CS on Same Prescription Hardcopy Allowed Rule 9(b)(5) Repealed In 2014 Out of State Prescriptions Non-CS Scripts – Pharmacies can fill non-controlled prescriptions written by prescribers (MDs, DOs, podiatrists, physician assistants, nurse practitioners, dentists, licensed veterinarians), outside of Michigan (state, district, territory, commonwealth or insular possession of the United States) as long as they fall within the prescriber's scope of practice. – Pharmacists may also accept prescriptions for non-controlled medications written by Canadian MDs or DOs. Out of State Prescriptions CS Scripts – Controlled substance prescriptions can only be accepted if issued by a physician prescriber (MD or DO) or dentist (DDS) prescriber who is authorized under the laws of that state to practice dentistry, medicine or osteopathic medicine and surgery and is authorized to prescribe controlled substances. and areas subject to lawful authority of the U.S. – Controlled substance prescriptions written by mid-level practitioners (physician assistants, nurse practitioners and certified nurse midwives). Script Record-Keeping Retain invoices, billing statements and Drug Enforcement Administration 222 forms, etc., for two years Pharmacy prescription records for five years. Michigan Medicaid requires records to be kept for seven years Medicare Part D regulations require all records to be kept for 10 years. Date of Last Refill Return to Stock Meds Community (outpatient) – Once meds leave “control” of pharmacy, they cannot be returned to stock Institutional – If the pharmacy "returns to stock" in an open bottle of the medication with the same lot number and expiration date from which the drug was originally filled from, it is not misbranding. If the lot number and expiration dates are different, or it is left in the vial without an expiration date or lot number, then it would be considered misbranding. It would also violate the rule of ensuring the strength, purity and quality of the medication dispensed. – Unit Dose Okay to return to stock Destroying CS Meds in an Institution A responsible individual must record the destruction of controlled substances in medical institutions. Destruction usually occurs after a substance has been dispensed and the patient expires or leaves the institution. The quantity destroyed and reason for destruction must be recorded in a manner that achieves accountability. Controlled Substance Rule 54(9) If the institution has a policy that reflects current practice standards and delineates the method of destruction, an explanation would only be required if policy is not followed. Mailing Scripts Law prohibiting Mail-Order Scripts was repealed several years ago If Mailing Meds through USPS, must follow federal labeling rules – Label container as required by Michigan law No “hazardous substances” may be mailed Vending Machines Vending Machines Must be approved by MI BoP Pharmacy cannot own a Vending Machine in a physician’s office Many Types of Machines – Dispensing in Pharmacy – Administering Drugs to Patient – Dispensing to Patient Vending Machines Crack pipe vending machines stir controversy in western Canada – An initiative by drug addiction outreach groups in Vancouver, the brightly colored vending machines sell crack pipes for 25 cents, a move advocates say will curb the spread of HIV and hepatitis. (2014) Emergency Drug Boxes Hospice – Each drug box under the control of the pharmacy shall be examined at least weekly to assure that the seal which designates that the box has not been opened is still intact and the expiration date has not been exceeded. – If the expiration date has been exceeded or the box has been opened, the box shall be returned to the pharmacy. – When written prescriptions are required, the prescriptions of the attending physician or hospice medical director shall accompany the drug boxes that have been opened when the drug boxes are returned to the pharmacy. Emergency Drug Boxes Hospice – The pharmacy shall maintain a permanent record of drug box exchanges on a drug box exchange log. The record shall contain all of the following information: (a) The number of the box. (b) The name of the hospice to which the box is released. (c) The date the box is released to the hospice. (d) The name and signature of the pharmacist who releases the box to the hospice. (e) The expiration date assigned. (f) The date the box is returned to the pharmacy for restocking. (g) The name and signature of the pharmacist who received the box for restocking. Emergency Drug Boxes Hospice – Upon return of the drug box to the pharmacy, the pharmacist shall reconcile the drugs dispensed from the drug box with the prescriptions of the attending physician or medical director of the hospice. The pharmacist shall note that the prescriptions were dispensed from the hospice drug box on the back of the prescriptions. – The prescriptions shall be filed in the same manner as other prescriptions are maintained at the pharmacy. Compounding Drugs New complex rules – STATE AND FEDERAL LAWS What is compounding? (Generic Definition) The Art and Science of Creating Personalized Medications – Preparing personalized medications for patients. – Compounded medications are made based on a practitioners prescription in which individual ingredients are mixed together in the exact strength and dosage form required by the patient. What is compounding? (Michigan Legal Definition) the preparation, mixing, assembling, packaging, and labeling of a drug or device by a pharmacist under the following circumstances: (a) Upon the receipt of a prescription for a specific patient. (b) Upon the receipt of a medical or dental order from a prescriber or agent for use in the treatment of patients within the course of the prescriber's professional practice. (c) In anticipation of the receipt of a prescription or medical or dental order based on routine, regularly observed prescription or medical or dental order patterns. (d) For the purpose of or incidental to research, teaching, or chemical analysis and not for the purpose of sale or dispensing. (4) "Compounding" does not include any of the following: (a) Except as provided in section 17748c, the compounding of a drug product that is essentially a copy of a commercially available product. (b) The reconstitution, mixing, or other similar act that is performed pursuant to the directions contained in approved labeling provided by the manufacturer of a commercially available product. (c) The compounding of allergenic extracts or biologic products. "Compounding" does not include any of the following: (a) the compounding of a drug product that is essentially a copy of a commercially available product. (b) The reconstitution, mixing, or other similar act that is performed pursuant to the directions contained in approved labeling provided by the manufacturer of a commercially available product. (c) The compounding of allergenic extracts or biologic products. Federal Compounding Laws The Drug Quality and Security Act (DQSA) of 2013 – FDA released several policy documents related to compounding as part of the agency’s implementation of DQSA in 2014. FDA Compounding Policies Draft interim guidance describing FDA’s expectations for compliance with current good manufacturing practice requirements for compounding facilities registered as outsourcing facilities with FDA A proposed rule that would revise FDA’s current list of drug products that may not be compounded due to withdrawal from the market or because they were found to be unsafe or ineffective Final guidance for pharmacies and individuals that intend to compound drugs under Section 503A, including FDA’s interim policies and a non-exhaustive list of potential enforcement actions against pharmacies or individuals that compound in violation of the Food, Drug, and Cosmetic Act Two Federal Register notices that reopen FDA’s request for nominations for the bulk drug substances lists for compounding in relation to Section 503A and Section 503B respectively https://www.nabp.net/news/fda-releases-dqsa-compounding-rulesand-guidance-documents FDA Guidance Policy “Pharmacy Compounding of Human Drug Products Under Section 503A of the Federal Food, Drug, and Cosmetic Act” http://www.fda.gov/downloads/Drugs/ GuidanceComplianceRegulatoryInform ation/Guidances/UCM377052.pdf Michigan Compounding Laws Passed in 2014 Effective September 30, 2015 Two Classes – Non-sterile – Sterile Sterile Compounders A pharmacy that that provides compounding services for sterile pharmaceuticals must be accredited by a national accrediting organization approved by the board, and be in compliance with USP standards in a manner determined by the board. Recordkeeping of Compounding Except for distribution within a hospital or another health care entity under common control, a pharmacist shall maintain a record of a compounded sterile pharmaceutical in the same manner and for the same retention period as prescribed in rules for other prescription records. The pharmacist shall include, but is not limited to including, all of the following information in the record required under this subsection: (a) The name, strength, quantity, and dosage form of the compounded pharmaceutical. (b) The formula to compound that includes mixing instructions, all ingredients and their quantities, and any additional information needed to prepare the compounded pharmaceutical. (c) The prescription number or assigned internal identification number. (d) The date of preparation. (e) The manufacturer and lot number of each ingredient. (f) The expiration or beyond-use date. (g) The name of the person who prepared the compounded pharmaceutical. (h) The name of the pharmacist who approved the compounded pharmaceutical. More Compounding Rules A pharmacist shall not offer excess compounded pharmaceuticals to other pharmacies for resale. A compounding pharmacy shall not distribute samples or complimentary starter doses of a compounded pharmaceutical to a health professional. A compounding pharmacy may advertise or otherwise promote the fact that they provide compounding services. Compounding Exception Based on the existence of a health professional/patient relationship and the presentation of a valid prescription, or in anticipation of the receipt of a prescription based on routine, regularly observed prescription patterns, a pharmacist may compound for a patient a non-sterile or sterile pharmaceutical that is not commercially available in the marketplace BoP Compounding Rules to Come The department (LARA), in consultation with the board, may promulgate rules regarding conditions and facilities for the compounding of non-sterile and sterile pharmaceuticals.