C23 ludbrook
advertisement

New Dimensions in Preoperative Assessment
G Ludbrook
University of Adelaide & S.A. Health
Disclosures and acknowledgements
Grant funds or commercial agreements:
Medibank Private
WA Health (SHRAC)
Medtel Australia
Member, Clinical Governance Committee, RDNS
Customer of O’Brien Glass
Business challenges
Cost escalation
Societal expectations (time)
Technology
Meeting the challenges of cost and quality
Remote, rapid access and communication
Information processing
Technology
Healthcare
Conflicting pressures Changing environment
Increased demand
Limited resources
Changing society
Technology
Australian population projections
our patient profile
Young population
“pyramid”
Ageing population
“middle-aged spread”
Old population
“coffin shaped”
112 anaesthesia-related deaths
Inadequate preoperative assessment - 28% of cases
Inadequate preoperative management - 21% of cases
Processes of current preoperative workup
Elective surgery
Anaesthetic OPD / Rooms
Processes
DSU / DOSA
Surgeon decides on operation
Patient comes to clinic
Input from multiple clinicians
Nursing
Anaesthetist
Pharmacist
Surgical intern
Further testing +/- specialist
referral off site
Possible repeat clinic visit
Exchange of
data
History
Examination
Surgeon decides on operation
Some work up may occur
Seen on DOS by anaesthetist
Testing
Data integration
and analysis
Management
decisions
Resource
Fit 17 yrexpensive
old girl
Time expensive
Dental work
– staff/patient
Mother and
High
daughter
quality lost a day
Efficient?
off work
70 yr
Resource
old repeat
inexpensive
colonoscopy
Defibrillating
Time inexpensive
pacemaker
inserted Quality?
since last ‘scope
Efficient?
Processes of current preoperative workup
Windscreen repair / replacement
Themes across industries
Process analysis
New technologies
Early triage and streaming to best care pathways
Remote communication
Specific elements
Early triage and streaming
•Data exchange
/ communication
Computer
decision support
•Data management & integration
•Data analysis / Decision making
•Management pathways
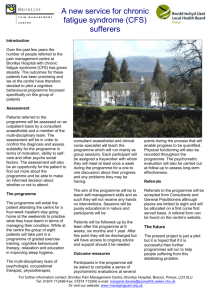
Virtual Hospital
Telehealth Service
Medication Management via a videophone
Drivers for New Service
•
•
•
•
•
An aging population
Increased incidence of chronic diseases
Increased pressure on existing health services…
Need to increase client access ….
Maximise workforce efficiencies
New technologies + creative health services
= innovative service delivery
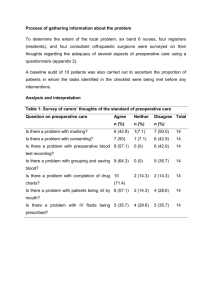
Formal evaluation
Cost Effectiveness
o Time reduction - 7 minutes vs 19 minutes
o Cost reduction - 40% decrease
Risk and Safety
o Vast reduction in reported medication incidents –
pharmacy delivery
Client satisfaction
o Less intrusive for client
o Increased client control over medication
management
Telemedicine versus telephone for remote
emergency stroke consultations: a critically
appraised topic.
Capampangan DJ, Wellik KE, Bobrow BJ, Aguilar MI, Ingall TJ,
Kiernan TE, Wingerchuk DM, Demaerschalk BM.
To determine the efficacy of telemedicine versus
telephone-only consultations for decision making in acute
stroke situations.
Neurologist. 2009 May;15(3):163-6
Audio-visual
(videoconference)
Telephone only
98%
(NNT 6)
82%
Specificity
98%
92%
Sensitivity
100%
58%
Thrombolysis eligibility
PPV
NPV
94%
100%
76%
84%
Correct acute stroke
treatment decisions
Neurologist. 2009 May;15(3):163-6.
Preoperative call centre pre-screening
Remote communication – phone or internet
Non-clinician delivered
Computer assisted ‘smart’ questionaire
Preoperative medical pre-screening
517 patients from two tertiary referral centres
Call centre pre-screening before elective surgery
Quality of data benchmarked against that collected in OPD
55 anaesthetists involved in assessment
Grant, Ludbrook, O’Loughlin, Corcoran et al., unpublished data
High quality data collected in 15 minutes
Would in theory allow 50-60% of these patients to
be seen on DOS
Grant, Ludbrook, O’Loughlin, Corcoran et al., unpublished data
Data summary and processing
Consistency
Legibility
Areas of concern highlighted
Pre-Admission Website: Patients are asked to complete an online
assessment.
Healthbank PreOp Anaes Tab: If a disease needs further exploration
the anaesthetist has a very powerful drilldown tool.
Decision making
Evidence-based
Consensus-based
Opinion-based
Eminence-based
Vehemence-based
Eloquence-based
Providence-based
Diffidence-based
Arrogance-based
Isaacs and Fitzgerald, BMJ 319 : 1618 1999
Lam BMJ. 2000 July 22; 321(7255): 239
Expert consensus on preoperative testing
http://www.nice.org.uk/nicemedia/live/10920/29090/29090.pdf
http://www.nice.org.uk/nicemedia/live/10920/29090/29090.pdf
Determinants of OSA
data modelling
Collect data on patient factors which might predict OSA
Benchmark against sleep studies
Mathematical models which predict likelihood of OSA
{
Model performance
Reasonable performance using history alone
Improvement adding other factors (eg neck circumference)
Positive
Predictive
Value
{
Determinants of preoperative decisions
data modelling
•
•
•
•
Preoperative clinical decisions without hard evidence
Obtained opinions from 55 anaesthetists on 517 patients
Identified predictive factors
Built predictive models which identify what the “group”
would do for specific cases
Grant, Ludbrook, O’Loughlin, Corcoran et al.
Decision support: pre-screening
Probability
Model ROC AUC
Lumbar discectomy
65 yr old male
BMI 35
Treated hypertension
Previous CVA
CBP
0.828
MBA
0.861
Coags
0.709
ECG
0.903
ICU
0.876
OPD
0.852
93%
93%
9%
99%
67%
90%
Grant, Ludbrook, O’Loughlin, Corcoran et al., submitted to BJA
Value of consensus in decision making
“..... a medical practitioner will not be found
negligent if they acted in a manner that was
widely accepted in Australia, by a significant
number of respected practitioners in the field…..”
Maher and Burke, Medical Journal of Australia,
194(5), 253-255, 2011
Processes of current preoperative workup
Elective surgery
Anaesthetic OPD / Rooms
Processes
DSU / DOSA
Surgeon decides on operation
Patient comes to clinic
Input from multiple clinicians
Nursing
Anaesthetist
Pharmacist
Surgical intern
Further testing +/- specialist
referral off site
Possible repeat clinic visit
Exchange of
data
History
Examination
Surgeon decides on operation
Some work up may occur
Seen on DOS by anaesthetist
Testing
Data integration
and analysis
Management
decisions
Processes of current preoperative workup
Elective surgery
Anaesthetic OPD / Rooms
Processes
DSU / DOSA
Surgeon decides on operation
Patient comes to clinic
Input from multiple clinicians
Nursing
Anaesthetist
Pharmacist
Surgical intern
Further testing +/- specialist
referral off site
Possible repeat clinic visit
Exchange of
data
History
Examination
Surgeon decides on operation
Some work up may occur
Seen on DOS by anaesthetist
Testing
Data integration
and analysis
Management
decisions
Processes of current preoperative workup
Elective surgery
Anaesthetic OPD / Rooms
Processes
DSU / DOSA
Surgeon decides on operation
Patient comes to clinic
Input from multiple clinicians
Nursing
Anaesthetist
Pharmacist
Surgical intern
Further testing +/- specialist
referral off site
Possible repeat clinic visit
Exchange of
data
History
Examination
Surgeon decides on operation
Some work up may occur
Seen on DOS by anaesthetist
Testing
Data integration
and analysis
Management
decisions
National E-Health Strategy
December 2008
E-Health will:
•Ensure the right consumer health information is electronically made available to the right person at
the right place and time to enable informed care and treatment decisions
•Enable the Australian health sector to more effectively operate as an inter-connected system
overcoming the current fragmentation and duplication of service delivery
•Provide consumers with electronic access to the information needed to better manage and control
their personal health outcomes
•Enable multi-disciplinary teams to electronically communicate and exchange information and
provide better coordinated health care across the continuum of care
•Provide consumers with confidence that their personal health information is managed in a secure,
confidential and tightly controlled manner
•Enable electronic access to appropriate health care services for consumers within remote, rural
and disadvantaged communities
•Facilitate continuous improvement of the health system through more effective reporting and
sharing of health outcome information
•Improve the quality, safety and efficiency of clinical practices by giving care providers better
access to consumer health information, clinical evidence and clinical decision support tools
•Support more informed policy, investment and research decisions through access to timely,
accurate and comprehensive reporting on Australian health system activities and outcomes.
Allscript
Emergisoft
Firstnet
Healthbank
etc
New models of care
OPD / Rooms
Processes
DSU / DOSA
Surgeon decides on operation
Patient comes to clinic for
workup
Input from multiple clinicians
Nursing
Anaesthetist
Pharmacist
Surgical intern
Further testing +/- specialist
referral off site
Possible repeat clinic visit
Exchange of
Surgeon decides on operation
information
Some work up may occur
Inspection and Seen on DOS by anaesthetist
auscultation
Testing
Decision making
Management
New models of care
Early triage
Call centre-based pre-screening
Computer smart questionnaire
Medicine
Nursing
Computer-generated guidelines
Call centre follow up
Remote lab testing
Data collection
Phone follow up
Informed consent
Streaming to:
Outpatients vs DOSA
Appropriate facility
“It is not the strongest of the species that survives,
nor the most intelligent that survives. It is the one
that is the most adaptable to change……”