The National Personality Disorder Development Programme
advertisement

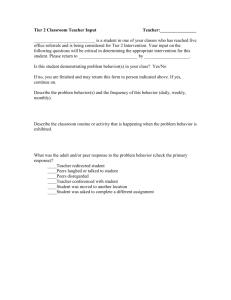
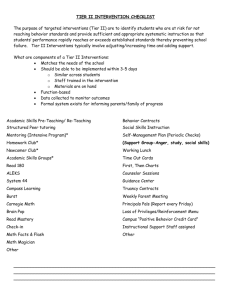
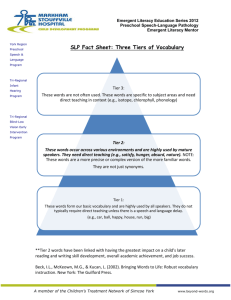
The National Personality Disorder Development Programme Personality People & Pathology 1 June 2005, Friends Meeting House, Oxford Rex Haigh & Steve Pearce The National Personality Disorder Development Programme Aims: • To develop new approaches to treatment and care of people diagnosable with PD • Strengthen the capabilities of the workforce through education and training • Reduce social exclusion Two Government publications National Institute for Mental Health for England (NIMHE) Government money: services • Deliberate variety of approaches • All involve many stakeholders • Working together to provide new type of service • Service users help in planning • Care pathways approach • Very strong control over finances & governance • Emphasis on evaluation, outcome & dissemination • Results in 2005-7 The National Personality Disorder Development Programme Rex Haigh Consultant Psychiatrist in Psychotherapy, Berkshire Healthcare NHS Trust Personality Disorder Development Consultant, NIMHE South East Personality Disorder Service User Consultation Lead, Department of Health Two Government publications National Institute for Mental Health for England (NIMHE) New Government Money • Started as “crumbs from the DSPD table” • Personality disorder: the “DSPD” units – £128m (£100m capital + £28m revenue) – For a few hundred people – eg £0.5m per patient per year at Broadmoor • Personality disorder: community programme – £18m – For ~5% of the population (3,000,000 people) – Equals £6.60 each case per year (or 33p per head of population) • Intention to coordinate across 4 “silos” Four “silos” • New pilot projects – 2 years funding thence PCT • National specialist commissioning – Henderson, Main House and Webb House • DSPD units – 4 in prisons, 6 in forensic and 4 womens units • Training initiatives – Divided amongst 8 NIMHE regions What “No Longer a Diagnosis of Exclusion” is funding: the 11 new community pilot services • Deliberate variety of approaches • All involve many stakeholders • Working together to provide new type of service • Service users help in planning • Care pathways approach • Very strong control over finances & governance • Emphasis on evaluation, outcome & dissemination • Results in 2005-7 What “No Longer a Diagnosis of Exclusion” means www.publications.doh.gov.uk/mentalhealth/personalitydisorder.pdf • 2004-2007 • 11 new pilot projects • Learning from diversity – – – – – 4 “big ones” 2 managed networks 2 predominantly SU-led 1 early intervention Different therapeutic models, some mention none The 11 pilots • A quick tour, giving: – Who submitted bid – Who manages it (=owns it?) – Clinical model – Distinguishing features Leeds • Submitted by Tom Mullen, Leeds Mentally Disordered Offender Development Coordinator, Leeds MHTT • Provider: Leeds MHTT • Managed clinical and service network • Core team working across agencies • Providing – Assessment – Clinical Services – Care coordination • Largest urban project Nottinghamshire • Submitted by Helen Scott, Executive Director, Nottinghamshire Healthcare NHS Trust (MHT) • Provider: Nottinghamshire Healthcare NHS Trust (MHT), and local advocacy groups • Coordinated network with new clinical services • 3 levels of provision – L1= advice and information – L2= “stop and think” CBT – L3= therapeutic community • • • • With satellite services across the county Integrated team Wide range of stakeholders Large population (>1m) and budget Coventry • Submitted by Coventry PCT • Provider: Coventry PCT • New clinical services – “community psychotherapy team” – group-based programmes for simple, complex, & severe PD • Integrated with new NSF-aligned psychiatric services • New building • Most favourable funding to population ratio Thames Valley • Submitted by Drs Rex Haigh & Steve Pearce, consultant psychiatrists in psychotherapy • Providers: 3 MHTs - Berks, Bucks & Oxon • Hub and spokes – 3 hubs – Approx 10 spokes • New 4 tier clinical services – – – – Assertive assessment (XBX) Local treatment provision 3 day TCs Recovery tier (XBX-led) • Multiple agencies involved • Integrated with training • Largest area & population (>2m) Camden & Islington • Submitted by Stephen Pilling, Consultant Clinical Psychologist, Camden and Islington Mental Health and Social Care Trust • Providers: Charitable Trust (“Umbrella Ltd”), two PCTs and the MH/SC Trust • Provision of two services: – Primary care: early recognition and brief treatment, DBT-based – Voluntary sector: helping people to reengage in work and be active citizens • Small project • Small population • Inner city NE London • Submitted by Dr Janet Feigenbaum, Consultant Clinical Psychologist • Provider: NE London MHT • Dual Diagnosis Assessment and response Team: “DDART” • Dual diagnosis – PD & substance misuse • Provision of – Assessment – Interventions • DBT based • group & individual • with outreach – Case management SW London • Submitted by Dr Steve Millar, Consultant Psychiatrist in Psychotherapy • Provider: SW London & St Georges MHT • Service User Network (SUN) • To set up 4 local networks to – Support SUs – Improve access to services • Large urban population • Small staff numbers Colchester • • • • The Haven Project Ltd Voluntary sector Drop-in day services Features of therapeutic community • Also short term crisis beds Cambridge & Peterborough • Submitted by Annette Newton (Area Director and MH Policy Lead, MHT), Prof Geoff Shepherd (Director of Partnerships and Service Development, MHT) and Dr Chess Denman (Consultant Psychotherapist) • Provider: Cambridge & Peterborough Mental Health Partnership Trust • No theoretical approach specified in bid • Services provided in two “hubs” – Assessment – Interventions – Case management • Development workers = spokes, to work across agencies and promote recovery model North Cumbria • Submitted by Dr Mike Rigby, Consultant Psychiatrist in Psychotherapy • Provider: North Cumbria MHT • “Itinerant therapeutic community” – – Intensive day service model Aspatria RC & Carlisle • Closely integrated with training programme • Large rural area • Low population Plymouth • Submitted by Phil Confue, Director MH & LD, Plymouth PCT • Provider: Plymouth PCT • Early intervention model • Young people (<25) engaged through youth enquiry service • Social inclusion focus: “to prevent career as psychiatric patient” • Delivered in partnership with voluntary agencies • Includes DBT treatment Evaluation of the 11 pilots • Local – as described in individual bids – cooperation emerging • National – Imperial College London • Mike Crawford, Dorothy Griffiths, Tim Weaver, Deborah Rutter, Peter Tyrer – Mental Health Foundation • Iain Ryrie, Jan Wallcraft – University College London • Anthony Bateman, Gerhart Knerer, Peter Fonagy – Institute of Psychiatry • Paul Moran – University of Liverpool • Jonathan Hill Multi-method evaluation – A macro-level organisational evaluation of the context, form, function and impact of pilot services – A micro-level cohort study examining changes in health, social outcomes and direct costs of care among a cohort of people using these services – A micro-level qualitative study of service quality from the perspective of service users – A Delphi exercise to examine the level of consensus among academics, service users and providers about lessons that can be learnt for future service development What do they cost? • Smallest – SUN - £254,000 • Largest – Thames valley - £1,006,335 – Full year effect – Including capital expenditure and management costs – Excluding local contributions Cost to NIMHE per project Leeds Notts 1000000 900000 Coventry TV Cam & Is 800000 700000 600000 DDART SUN 500000 400000 300000 Haven Camb & Pet N Cumbria 200000 100000 0 1 Plym How many new staff? • In original bid (possibly amended since) • Minimum: Carlisle = 6 • Maximum: Thames Valley = 30.5 Number of staff per project Leeds Notts 3 0 .1 30 2 7.0 2 3 .5 Coventry TV Cam & Is 2 2 .6 20 12 .2 11.5 10 8 .4 7.4 0 1 8 .5 6 .5 6 .0 DDART SUN Haven Camb & Pet N Cumbria Plym Population covered • Less than half a million – – – – – – Waltham Forest DDART Coventry North Cumbria Essex Haven Camden and Islington Plymouth • Over a million – Thames Valley (Berkshire, Buckinghamshire and Oxfordshire) – Nottinghamshire Population served by each project 2,500,000 Leeds 2,000,000 Notts Coventry 1,500,000 TV Cam & Is DDART 1,000,000 SUN Haven Camb & Pet N Cumbria 500,000 Plym 0 1 projects Calculation: money spent per “case” Assuming 5% of total population “have” PD: • • • • MAXIMUM – Coventry - £56 MINIMUM – SW London SUN - £6.52 MEAN - £17.75 REST OF ENGLAND in PCT baselines - £4.01 Spend per case for each project Leeds Notts 60 Coventry TV Cam & Is 50 40 30 DDART SUN 20 Haven Camb & Pet N Cumbria 10 0 1 Plym Calculation: “cases” per new staff member • MAXIMUM – SW London SUN – 7662 – (14 minutes each per year = 19 sec weekly) • MINIMUM – Coventry – 701 – (2hr 37mins each pa = 3 mins 25 sec weekly) • MEAN - 2311 “Caseload” per project 8000 7000 6000 5000 4000 3000 2000 1000 0 Leeds Notts Coventry TV Cam & Is DDART SUN Haven Camb & Pet N Cumbria Plym Calculation: cost of each new staff member • MAXIMUM – North Cumbria – £70,883 • MINIMUM – Leeds – £31,852 • MEAN - £41,038 – Note: does not include contribution of volunteers, service users or ex-service users if unpaid. Cost per new staff for each project 80,000 70,000 60,000 50,000 40,000 30,000 20,000 10,000 0 Leeds Notts Coventry TV Cam & Is DDART SUN Haven Camb & Pet N Cumbria Plym Summary of “new money” • For 11 new pilot projects from NIMHE: – £6.8m for 7.5m population = £17.75 per case • Into PCT baselines 2004-5 – £8m (England only) = £3.20p per case • Into PCT baselines 2005-6 – £10m (England only) = £4.01 per case • For training programme 2004-5 & 2005-6 – £2m = £250K per NIMHE region More “new money”? • To bring England up to average level of pilot projects would cost • £868m • This represents increasing current funding by 52x • Or current funding is 1.93% of what is needed • Awaiting announcement from spending round (March 05?) • But most will need to come from service remodelling Forensic Service Developments DSPD services 2 new 70 bed units at Broadmoor and Rampton operational from 2005/6 Two new prison pilot sites at Frankland and Whitemoor are operational from 2004 Planned womens DSPD prison pilot at Lower Newton 6 pilot forensic services for people with PD who present a risk to others Women's high support community services (residential core and cluster services for women leaving high secure care) Forensic Service Developments Pilot services provided by: – – – – – – – South London and Maudsley Nottingham Healthcare Trust (Rampton) East London Mental Health Trust West London Mental Health Trust (Broadmoor) Oxleas Trust Newcastle, North Tyneside and Northumberland Trust Merseycare Mental Health Trust Forensic Service Developments Pilots include: • • • • Dedicated PD units within high secure services Dedicated PD units within medium secure services Associated hostels in three pilots Community Team in six Personality Disorder Capability Framework – Breaking the Cycle of Rejection • Comprehensive approach to improving capabilities of the workforce across many agencies responding to people diagnosable with PD • Total of £2m for 2004/5 allocated to 8 NIMHE Regional Development Centres for new initiatives to implement the framework. Personality Disorder Capability Framework – Breaking the Cycle of Rejection Training initiatives reflect partnership between WDDs, HEIs, NIMHE RDCs. National bodies (NHS University, Royal Colleges etc.), committed to joint work to establish training initiatives consistent with Capability Framework Learning networks will ensure dissemination of learning from pilot services. Training and education programme will be independently evaluated Personality Disorder Capability Framework – Breaking the Cycle of Rejection Current training and education initiatives include: • mapping/scoping exercises and training needs analyses • stakeholder consultation • “PD awareness cascade” courses • PD basic training modules to be incorporated in pre and post reg training • multi-agency modular training approaches • exploring training needs of commissioners. Local multi-agency training is also included in many of the service development pilots TRRT – training, research and recovery team • 4th team of TVi • TRAINING – to deliver this course and other events using XBXs and Agents • RESEARCH – to undertake national data collection and local evaluation of TVi • RECOVERY – to make service user, ex-service user and expert by experience partnerships essential • AND – external relations etc etc… TRRT: who, where, when? • 3.3 wtes: – – – – – – – • • • • • Sue Robinson Team Administrator 1.0wte Clare Stafford Project Manager 0.5wte Fiona Blyth Training Coordinator 0.5wte [vacant] Team Researcher 0.5wte Sheena Money Expert by Experience 0.3wte Yolande Hadden Expert by Experience 0.3wte Rex Haigh Programme Director 0.2wte Managed by OMHT through CS Located on Warneford site Phase 1 – setup – y1 Phase 2 – provide – y2 Phase 3 – the future – y3+? TRRT and training • To coordinate all training offered • To “capacity-build” SU, XSU & XBX involvement (STARS) for training and clinical function • To provide (very limited!) funding for training activities – alongside NIMHE funding • To provide (more substantial) funding for XBX input • To get it onto secure financial footing SE Training Plan – aka “network course” – aka “awareness cascade” Development of new services PD Treatment Facilities police Seminars, conferences, short courses, workshops, etc Qualification A&E 1 year PD network course Awareness cascade Further training housing police probation PD agents Primary care Voluntary organisations Voluntary organisations mental health services A&E probation prison s Policy makers Dynamic teams Input into course philosophy, structure and content Primary care commissoners Service advocacy XBX pool mental health services MH managers prison s Social services Social services housing Interested recruits TRRT and research • Two serious attempts at recruitment July 04 and Feb 05 • Coordination with – National team – Nottingham – Coventry • Minimum dataset agreed across TV = National + SCID2 + CORE + • Awaiting ethical clearance • Other local research (eg qualitative and user-led) will need to await appointment of researcher TRRT and recovery • To make service user partnership (+XSU +XBX) essential – Writing bid together – Planning clinical policies together – Two paradoxes emerging • To administer fairly – Systems, administration, payment • Employment and life beyond – Examples – Other agencies STARS support, training and recovery system • • • • XSUs and XBXs Monthly meeting Last Friday afternoon Lunch - check-in – feedback – planning & allocation – open group – educational slot – check-out • Usual attendance about 20, with 25 on our books • In a central Reading nightclub owned by lottery winner, friend of an exservice user! • Requests for involvement taken through Sue • Agreed at TRRT • Includes Training, Clinical and Service Advocacy • Training and advocacy activities in TV – we pay XBX fees and expenses (if outside, we charge) • Agents would be welcome – especially if they come and tell us what they are up to, or with requests for involvement TRRT: other coordination • Initially – recruitment – eg polymorphous and nondisciplinary job profiles • • • • Team building In-house training structures Coordination between teams Annual Development Conference – 6 July Kindersley Centre • Organisational links – PCTs, MHTs, national team, learning network, ATC, CofC, NIMHE, BUK, RCPsych, multitude of others Morning session: TVi clinical pilot Professionals’ session: 10am – 12noon [Service user session running in parallel] Oxford • Presentation of case vignettes by Naomi Evans, Team leader – any questions. • Discussion of the current service and focus on commissioning arrangements from 2006/7 Berkshire • Presentation of case vignettes and research findings by Davey Rawlinson, Senior Psychotherapist. Any questions • Discussion of current service, funding and commissioning arrangements currently and from 2006/7. Buckinghamshire • Presentation of case vignettes by Marion Panchkowry and Alex Esterhuyzen, programme leads. • Discussion of the current service and focus on commissioning arrangements from 2006/7 TRRT • Presentation of TRRT development and activity by Rex Haigh, Programme Director and Fiona Blyth, Training Coordinator • Discussion of likely commissioning arrangements from 2006/7 Personality Disorder Capability Framework – Breaking the Cycle of Rejection • Comprehensive approach to improving capabilities of the workforce across many agencies responding to people diagnosable with PD • Total of £2m for 2004/5 allocated to 8 NIMHE Regional Development Centres for new initiatives to implement the framework. Personality Disorder Capability Framework – Breaking the Cycle of Rejection Training initiatives reflect partnership between WDDs, HEIs, NIMHE RDCs. National bodies (NHS University, Royal Colleges etc.), committed to joint work to establish training initiatives consistent with Capability Framework Learning networks will ensure dissemination of learning from pilot services. Training and education programme will be independently evaluated by NU (Peter Lewis is our link) Personality Disorder Capability Framework – Breaking the Cycle of Rejection Current training and education initiatives include: • mapping/scoping exercises and training needs analyses • stakeholder consultation • “PD awareness cascade” courses • PD basic training modules to be incorporated in pre and post reg training • multi-agency modular training approaches • exploring training needs of commissioners. Local multi-agency training is also included in many of the service development pilots Training in the South-East Developing a network of “PD Agents” AWARENESS TRAINING • Different staff groups • Geographical spread • Agent’s agency • Various formats • With service user input • Feedback SERVICE ADVOCACY NETWORKS • In localities • Involving all interested parties • Putting case where needed • Support from TV & NIMHE Four “network courses” in SE Thames Valley: Oxford base Kent: Maidstone base Hampshire and Isle of Wight: Southampton base Surrey & Sussex: Brighton base Courses spec: 1 - philosophy • Based on “Breaking the Cycle of Rejection” Capabilities Framework • Encourages patient/client autonomy and development of individual responsibility • Well-reflecting the views of users and carers • Non-threatening • Empowering learners to use what they already know • Finding common language • Focus on attitude change and stigma reduction Courses spec: 2 - structure • • • • • • • • • Starts September 2004, finish by June 2005 Between 20 and 40 course participants Variety of teaching methods Planned and run by multidisciplinary team, including contributions from all significant services in SHA area Service user or ex service user input to planning and delivery Inclusive and accessible (e.g. no disciplines excluded through use of jargon) Multi-professional Multi-agency Multi-sector Cont… • Mechanism for cascade of awareness training through course participants • Continuing support for course graduates wanting to undertake further PD work • Participation in SE-wide and national evaluation • Use of IT and NIMHE KC for dissemination of course material and widening reach of PD training • Commitment to continuation and further development beyond year 1 • Collaboration with other SE courses in annual development conference Courses spec 3 - content • • • • • • • • • • • • • • Minimum of seminars + work discussion + reflective component Evidence-based, where it exists Case formulation from different approaches Explains PD phenomenology an continuum Includes Aetiology Interventions and evidence Sociological and deviance perspectives Eclectic with regard to therapeutic or theoretical models Management principles: engagement, attachment and consistency Stigma and education Attend to team and organisational dynamics Models of supervision Skills: what to do and what not to do Service design discussions Courses spec 4 - admin • Pamphlet to include course aims, intended audience, dates and outline of content • With SEDC logo • Produced by end of June • Circulated widely within all MH trusts in SHA • Circulated to other agencies within SHA area (eg primary care, voluntary sector, social services etc) • Course outlines using pro-formas below to be received by SEDC by June 11 • Approval for funding by end of June • Supporting costs will be paid in three parts: £10,000 in July for setting up • Further £10,000 in December 2004 when evidence of course delivery, including course brochures, number of participants with their professional backgrounds, work settings and employing organisations is received • Final £10,000 in Summer 2005 when number completing the course, participants’ feedback and analysis, and plans for future development are received mental health services Primary care A&E probation prison s police 1 year PD network course Voluntary organisations Social services housing mental health services Qualification A&E probation prison s police 1 year PD network course Voluntary organisations Social services housing Further training PD agents PD Treatment Facilities (few and far between) XBX pool PD Treatment Facilities XBX pool mental health services Dynamic teams Input into course philosophy, structure and content Primary care Qualification A&E probation prison s police 1 year PD network course Voluntary organisations Social services housing Further training PD agents PD Treatment Facilities Service advocacy XBX pool mental health services Dynamic teams Input into course philosophy, structure and content Primary care Qualification A&E Awareness cascade probation prison s police 1 year PD network course Voluntary organisations Social services housing Seminars, conferences, short courses, workshops, etc Further training PD agents Development of new services PD Treatment Facilities Dynamic teams Primary care Qualification A&E Awareness cascade police 1 year PD network course Voluntary organisations Social services housing Further training PD agents Policy makers Seminars, conferences, short courses, workshops, etc Input into course philosophy, structure and content probation prison s commissoners Service advocacy XBX pool mental health services MH managers SE Training Plan – aka “network course” – aka “awareness cascade” Development of new services PD Treatment Facilities police Seminars, conferences, short courses, workshops, etc Qualification A&E 1 year PD network course Awareness cascade Further training housing police probation PD agents Primary care Voluntary organisations Voluntary organisations mental health services A&E probation prison s Policy makers Dynamic teams Input into course philosophy, structure and content Primary care commissoners Service advocacy XBX pool mental health services MH managers prison s Social services Social services housing Interested recruits • 3 County clinical services • Plus “Umbrella” function including training • …called TRRT • In close partnership with STARS TRRT – training, research and recovery team • 4th team of TVi • RH, SM, YH, CS, SR and --just--- FB. “TR” yet to be appointed. • TRAINING – to deliver this course and other events using XBXs and Agents • RESEARCH – to undertake national data collection and local evaluation of TVi • RECOVERY – to make service user, ex-service user and expert by experience input essential ROLE IN TRAINING • To coordinate all training offered • To “capacity-build” SU, XSU & XBX involvement (STARS) for training function • To provide (very limited!) funding for training activities • To provide (more substantial) funding for XBX input • To get it onto secure financial footing STARS support, training and recovery system • • • • XSUs and XBXs Monthly meeting Last Friday afternoon Lunch - check-in – feedback – planning & allocation – open group – educational slot – check-out • Usual attendance about 20, with 25 on our books • In a central Reading nightclub! • Requests for involvement taken through Sue • Agreed at TRRT • Includes Training, Clinical and Service Advocacy • Training and advocacy activities in TV – we pay XBX fees and expenses (if outside, we charge) • Agents would be welcome – especially if they come and tell us what they are up to, or with requests for involvement Aims of today • To bring different parts of the training and service initiative together • To understand what we are all doing • To know where to get help and collaboration • To start planning what else we want to do • To get at least 3 useful new email addresses or phone numbers in our address books …! Thames Valley • 3 hubs – Reading, Oxford and Bucks • Various satellites • Numerous partners • 4 tier model • Working without county boundaries • TV-wide functions: recruitment, induction, training, staff support, evaluation, XBX input, awareness training, service advocacy Thames Valley Initiative service model: outline of tier 1 • Tier 1 is similar to assertive outreach in AMI services: not “office-bound”. • It needs to be organised with numerous agencies at locality level. • Individual and joint consultations • Includes weekly nonexploratory group, drop-ins, various formats AKA… • • • • Assertive Engagement Facilitated Engagement Active Assessment Engagement & assessment • What is the best name for it?... Thames Valley Initiative service model: choice & consent in tier 1 • • • • we will not take direct referrals in the traditional “passing on of responsibility” way the final common pathway to all coming into the services will be individuals’ choice (ie self-referral) that will be as informed as facilitated as possible with particular emphasis on employing ex-service users in full collaboration, as XBXs • To develop close liaison with all relevant other agencies, for example through “PD Agents” network • assessment and engagement will be a two-way and continuing process with certain stages and decision points • this will be related to sharing responsibility with other clinicians, then taking full responsibility in later part of the programme Thames Valley Initiative service model: activities and aims for tier 1 • Telephone advice to members of staff dealing with a potential PDPs. • Consultation and support regarding individual clients. • Support to clients who selfrefer • Liaison with all relevant agencies. • Staff education, by telephone or by TVi staff attending others’ staff meetings. • Drop-in sessions for potential PDPs. • Access groups, for PDPs to understand the service and to support them in engaging in further therapeutic work. • Providing care tailored to each individual that takes account of disabilities, gender, sexual orientation etc. • Ensuring that everyone can access the service by employing staff from a range of ethnic and cultural backgrounds • Helping PDPs disengage with other services they may be receiving, as appropriate Tier 1: Assertive engagement and active assessment Various combinations of different days for different referral groups, iin different locations Numerous activities in different settings with different agencies, statutory & voluntary. Tier 2: Outreach, inreach and “access to therapy” Could include weekend programmes for those in full time work or education Definitive therapeutic activities at different times in the week, for different populations, in different locations Tier 3: Day programme: therapeutic community Whole-time daily programme at service core, with different activities, therapies and groups. Admin centre, also training base. Tier 4: Leaving process – support & recovery Half day per week (or less), possibly with overlap into last weeks/months of tier 2 or tier 3 programme. In liaison with other agencies (eg college, employment). Normally thence back to GP care only. Tier 1: Assertive engagement and active assessment Numerous activities in different settings, one common weekly “drop-in” engagement group for informal meeting and information sharing Various combinations of different days for different referral groups, iin different locations Tier 2: Outreach, inreach and “access to therapy” Could include weekend programmes for those in full time work or education Different activities at different times in the week, for different populations, in different locations Tier 3: Day programme: definitive treatment Whole-time daily programme as service base, with different activities, therapies and groups. Considerable user-involvement. Also training base. Tier 4: Leaving process – graded disengagement Half day per week (or less), with overlap into last weeks/months of tier 2 or tier 3 programme. In liaison with other agencies (eg college, employment). Normally back to GP care only. Samaritan s NHS Direct Selfreferral CAMHS eg parents with PD SSD s Univ & College health & counselling Occupational health Liaison psychiatr y A& E Prisons HV MAPPPs PC GP SHs Young offender services Court divert schemes Probation Adult mental health: CMHTs, IP, crisis services, assertive outreach Forensi c stepdow n Drugs & Alcohol units Homeless services Housing MIND, RF , etc For those with specific issues, geographical or time limitations, or not best served by daily programme Unplanned discharge For those able to take sufficient degree of responsibility for themselves Planned discharge Unplanned discharge For those able, willing, and likely to be helped by going on to a more intensive treatment programme Planned discharge Referral to more suitable services: occasionally to out-of-area residential units (eg Henderson or Cassel Hospitals) or to outpatient psychology or psychotherapy, when suitable. PD service model: coordination between local services MIND Elmor e Social Services Grendon Prison Milton Keynes PCT / Local Authority CONNECTION Oxfordshire Local Strategy Forum Oxon Axis 2 Service Assessment Wing F Thames Valley Strategy Forum & ‘Axis 2 Institute’ -Training functions only (grey arrows) -Strategy fora to coordinate services AND training functions (blue arrows) -Includes administration of service user input (throughout) -located in one trust or as part of SEDC / TVSHA -strategic links with other regionwide agencies -liaison with other regions Therapy Wings A, B, C, D, G CONNECTION Buckinghamshire Local Strategy Forum Parenting Assessment Project Local MH services Bucks Axis 2 Service Local MH services REA P Berkshire Local Strategy Forum NC(? ) Berks Axis 2 Service Local MH services Broadmoor Hospital: Psychotherapy & DSPD units Thames Valley Initiative service model: XBX involvement • 2 employees are XBXs • Also use pool of ~20 with sessional rates • Tasks: training, planning and clinical – Training: almost autonomous, across agencies (details later) – Planning: local, regional, national – Clinical: mostly tier 1 and tier 4 – user-friendly introduction to services and supportive network and “getting a life” “We would all have completed a recognised treatment in order that we have moved on enough to achieve sufficient objectivity to be able to look beyond our own therapeutic needs. The support and social element of the group would be available to people immediately after treatment, but involvement in training, planning and other paid work would not occur until six months after the end of treatment, in order to support people to move on from therapeutic attachments.” Onwards and Upwards: Berkshire Group • Climate change • Central resources for education • Local radio • Need to get something concrete • Awareness of what we are doing – promotion & awareness • Getting involved in TVU nurse training • Work with CMHTs – events / day conference • Will work with next lot of agents • Using what else is within the agents’ group • NOW! • XBX activity will need more funding, non-NHS possibilities Onwards and Upwards: Buckinghamshire Group • Using agents to influence managers • Coming on course is more than just the one year itself • Invite managers into the course to see work being done in project groups • With TRRT help • XBXs – how involvement has benefitted • Central resource of training materials – off-the-pegs • PD agents y1 & y2 will meet quarterly • Need to get out to GPs to support and educate (mixed picture) Onwards and Upwards: Oxfordshire Group • Sarah’s shopping list • No we can’t do any more – but we did • How do we keep on meeting? • Need to connect up with this year’s PD agents • Pick up ones who have dropped off the radar • Rolling out training we have already planned • Getting help to do that from others • GPs, other key areas to involve • Rethink & Mind • Detailed planning involving TRRT & STARS • Conference – fuzzy time line – still intended • PCT roadshows • Reln agents-clin team • Still need to think about HOW to do it. The National Personality Disorder Development Programme Training plans for the South-East Sue Earley (TVi), Kevin Emrys (TVi), Rex Haigh (SEDC), Sheena Money (TVi), Sue Robinson (TVi) 14 February 2005 Wellshurst Golf Club, East Sussex Ten Essential Shared Capabilities • =update of CPF + mapping for WD • shift in culture in services towards Choice, personcenteredness and mental health promotion is a key imperative • were significant gaps in pre and post qualification training of all professional staff in their ability to deliver the MHNSF and the NHSP • Being rendered helpless rather than helped by service use • embedded in induction and continuing professional /practitioner development Essential Shared Capabilities 1 & 2 • Working in Partnership. Developing and maintaining constructive working relationships with service users, carers, families, colleagues, lay people and wider community networks. Working positively with any tensions created by conflicts of interest or aspiration that may arise between the partners in care. • Respecting Diversity. Working in partnership with service users, carers, families and colleagues to provide care and interventions that not only make a positive difference but also do so in ways that respect and value diversity including age, race, culture, disability, gender, spirituality and sexuality. Essential Shared Capabilities 3 & 4 • Practising Ethically. Recognising the rights and aspirations of service users and their families, acknowledging power differentials and minimising them whenever possible. Providing treatment and care that is accountable to service users and carers within the boundaries prescribed by national (professional), legal and local codes of ethical practice. • Challenging Inequality. Addressing the causes and consequences of stigma, discrimination, social inequality and exclusion on service users, carers and mental health services. Creating, developing or maintaining valued social roles for people in the communities they come from. Essential Shared Capabilities 5 & 6 • Promoting Recovery. Working in partnership to provide care and treatment that enables service users and carers to tackle mental health problems with hope and optimism and to work towards a valued lifestyle within and beyond the limits of any mental health problem. • Identifying People’s Needs and Strengths. Working in partnership to gather information to agree health and social care needs in the context of the preferred lifestyle and aspirations of service users their families, carers and friends. Essential Shared Capabilities 7 & 8 • Providing Service User Centred Care. Negotiating achievable and meaningful goals; primarily from the perspective of service users and their families. Influencing and seeking the means to achieve these goals and clarifying the responsibilities of the people who will provide any help that is needed, including systematically evaluating outcomes and achievements. • Making a Difference. Facilitating access to and delivering the best quality, evidence-based, values-based health and social care interventions to meet the needs and aspirations of service users and their families and carers. Essential Shared Capabilities 9 & 10 • Promoting Safety and Positive Risk Taking. Empowering the person to decide the level of risk they are prepared to take with their health and safety. This includes working with the tension between promoting safety and positive risk taking, including assessing and dealing with possible risks for service users, carers, family members, and the wider public. • Personal Development and Learning. Keeping up-to-date with changes in practice and participating in life-long learning, personal and professional development for one’s self and colleagues through supervision, appraisal and reflective practice. More info on 10 ESC • www.nimhe.org.uk/downloads/78582DoH-10 Essentials.pdf • Or Google “Ten Essential Shared Capabilities”