spina bifida - School of Medicine
advertisement

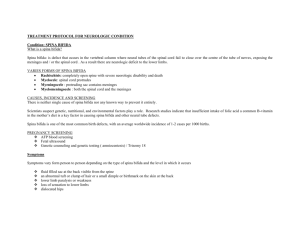
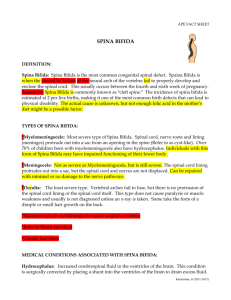
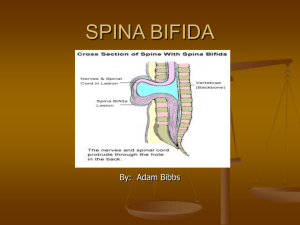
SPINA BIFIDA SPINA BIFIDA Failure of fusion of the vertebral arches. This mesodermal defect may be associated with a defect of ectoderm and neuroectoderm. SPINA BIFIDA First described by Nicholas Tulp 1593 Morgagni linked Hydrocephalus with Spina Bifida 1761 TYPES 1. Spina Bifida Occulta 20% of N. Child 2. Spina Bifida Cystica 2.5 / 1,000 Meningocoele - Protrusion of Meninges Myelomeningocoele - Protrusion of Meninges plus neural tissue Spina Bifida Occulta 1. 2. 3. Midline defect of Vertebral Bodies. Hair, Lipoma, dermal sinus, discolouration of skin. Occasionally associated with Diastematomyelia, Syringomyelia and Tethered Cord. Encephalocele Cranial Meningocoele – Meningeal Sac only Cranial Encephalocele – Sac plus Cerebral cortex, Cerebellum, Brain Stem Anencephaly Absent cerebral hemispheres and cerebellum Incid. 1/1000 live births Neuronal Migration Disorder Lissencephaly (Agyria) Schizencephaly Porencephaly Dandy Walker Malformation 1. Cystic Expansion of 4th Ventricle in Post Fossa. 2. 90% have hydrocephalus. 3. Shunting the cystic cavity. Proposed Aetiologies for Spina Bifida Multi-factorial inheritance. Potato blight. Vitamin deficiencies/folate. Maternal fever. Zinc deficiency. High sound intensity. Viral infection. Alcohol. Mineral deficiency. Medication – Phenytoin, Epilim, etc. Spina Bifida Incidence 2 – 2.5 / 1,000 births Genetic Predisposition 10% incidence of positive family histories 5% incidence of Spina Bifida / Encephalocele in sibling of an affected child 10-15% incidence if two siblings affected Adverse Criteria 1. 2. 3. 4. 5. 6. Gross paralysis of the legs. Thoraco-lumbar or thoraco-l/sacral lesions. Kyphosis or scoliosis. Hydrocephalus. Intracerebral birth injury. Other gross congenital anomalies. Types of Lesions in Spina Bifida Type I (1 / 3) Complete loss of spinal cord function below a certain segmental level. = ATONIC BLADDER Type II (2 / 3) Associated with interruption of corticospinal tract. = SPASTIC BLADDER. Expectations of Lower Urinary Tracts 1. 2. 3. 4. That bladder should fill to good capacity. Should empty to completion. Emptying should be under voluntary control. That filling and emptying should not be detrimental to renal function. Failure to Fill Bladder 1. 2. 3. Rise in intravesical pressure = low compliance. Detrusor hyperreflexia. Incompetence of bladder neck and distal sphincter mechanism = sphincter weakness incontinence Failure to Empty Bladder 1. 2. 3. No Detrusor Contraction. Detrusor – Sphincter Dyssynergia. Failure of bladder neck to open when the detrusor contracts. Aims of Treatment 1. 2. 3. To preserve renal function. To obtain efficient bladder emptying. To achieve continence. Anocutaneous reflex = Contractile Detrusor Anal Tone Normal = No significant sphincter weakness Normal Perianal Sensations = If all above present = Normal bladder and urethral sensations 25% who will have normal control Videourodynamic Study Bladder outline, size and capacity. Detrusor pressure at rest and during filling and voiding. State of bladder neck and urethra. Presence or absence of vesico-ureteric reflux. Management of Urinary Incontinence 1. 2. 3. 4. 5. 6. Manual expression of bladder. Time training. Indwelling catheterisation (silastic balloon catheter). Urinals – disposable penile sheaths. Pads and napkins. Clean intermittent catheterisations. Investigations in Spina Bifida 1. 2. 3. 4. 5. 6. 7. Regular urine checks q 1-3 / 12. Urea and creatinine q 6 / 12. I.V.U.’S q 2 years. Renal function tests and renogram. Measurement of residual urine. Videourodynamic studies and micturating cysto-urethrogram. Renal ultrasound. Management of Bowel Incontinence Bowel Training. 1. 2 x 10 min periods/day Diet. Physical Assistance. 2. 3. a) b) c) Pressure Manual evacuation Suppositories Laxatives e.g. Isagel & Senokot Enemas Problems of Management of Spina Bifida 1. Shunt Complications : Blocked shunts Infected shunts Shunt nephritis Seizures 1 / 3 Upper limb weakness Problems of Management of Spina Bifida 2. Orthopaedic Management : Hip dislocation Knee flexion deformities Foot deformities Spinal deformities Fractures Problems of Management of Spina Bifida 3. Urinary problems. 4. Intellectual Development. 40-60% have learning disability 5. Visual Defects. 6. Endocrine dysfunction. Problems of Management of Spina Bifida 7. Obesity. 8. Skin care. 9. Psychological and psychosexual problems. 10. School placement. Arnold Chiari Malformation Malformation of the lower brain stem and cerebellum and herniation of these structures through the foramen magnum. HYDROCEPHALUS 1 Communicating - most common Congenital/Acquired 2 Non Communicating • • • • • • Spina Bifida Aquaductal Stenosis Dandy-Walker malformation(cystic expansion of 4th ventricle in Post Fossa Tumours Aneurysmal Dilation of Vain of Galen Perinatal Haemorrhage Folic Acid Supplements 400 Microgram folic acid daily Continue for 1st three months of pregnancy