Antiviral agents
advertisement

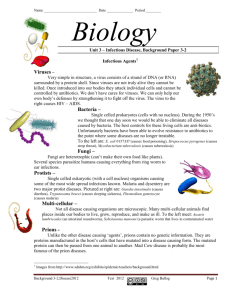
In vivo control of microorganisms Antiviral agents Virology; the study of viruses (or, lifestyles of the small and nasty) Viruses have one major characteristic in common: they are obligate intracellular parasites. Viruses are UNABLE to grow and reproduce outside of a living cell. No virus is able to produce its own energy (ATP) to drive macromolecular synthesis. However, in many other respects, they are a highly diverse group. The size of viruses Strategies for virus survival • Finding and getting into a host cell. As viruses are obligate parasites they must find the right type of cell for their replication, they must invade that cell and get their genome to the site of replication. • Making virus protein. All viruses are parasites of translation. The virus must make mRNA (unless it has a + sense RNA genome already). Strategies must exist to synthesize mRNA. • Making viral genomes. Many viral genomes are copied by the cell’s synthetic machinery in cooperation with viral proteins. • Forming progeny virions. The virus genome, capsid (and envelope) proteins must be transported through the cell to the assembly site, and the correct information for assembly must be pre-programmed. • Spread within and between hosts. To ensure survival the virus must propagate itself in new cells. • Overcoming host defences.The host defends itself against “nonself”. Viruses have evolved ways to fight back. Three problems every virus must solve • 1 • 2 • 3 How to reproduce during its “visit” inside the cell. How to a) copy its genetic information and b) produce mRNA for protein production How to spread from one individual to another How to evade the host defenses. This need not be complete. • Viral diseases are the (usually unintended) consequences of the way each virus has chosen to solve these three problems. How are viruses named? • Based on: - the disease they cause poliovirus, rabies virus - the type of disease murine leukemia virus - geographic locations Sendai virus, Coxsackie virus - their discovers Epstein-Barr virus - how they were originally thought to be contracted dengue virus (“evil spirit”), influenza virus (the “influence” of bad air) - combinations of the above Rous Sarcoma virus Virus Classification Taxonomy from Order downward (three orders now recognized) •Family often the highest classification. Ends in -viridae. •Many families have subfamilies. Ends in -virinae. •Bacterial viruses referred to as bacteriophage or phage (with a few exceptions). Examples family Myoviridae genus T4-like phages type species Enterobacteria phage T4 family Herpesviridae, subfamily Betaherpesvirinae genus Muromegalovirus type species Murine herpesvirus 1 The Baltimore classification system Based on genetic contents and replication strategies of viruses. According to the Baltimore classification, viruses are divided into the following seven classes: 1. dsDNA viruses 2. ssDNA viruses 3. dsRNA viruses 4. (+) sense ssRNA viruses (codes protein) 5. (-) sense ssRNA viruses 6. RNA reverse transcribing viruses 7. DNA reverse transcribing viruses directly for where "ds" represents "double strand" and "ss" denotes "single strand". RNA viruses From Principles of Virology Flint et al ASM Press DNA viruses From Principles of Virology Flint et al ASM Press Structural Classes •Icosahedral symmetry •Helical symmetry •Non enveloped (“naked”) •Enveloped Icosahedral capsids a) Crystallographic structure of a simple icosahedral virus. b) The axes of symmetry Enveloped helical virus Enveloped icosahedral virus Typical infectious cycle 1. Attachment 2. Penetration 3. Uncoating 4. Transcription and/or translation 5. Replication 6. Assembly 7. Release Virus recognition, attachment, and entry •Specific viral receptor •Co-receptor •Receptor-mediated endocytosis •Fusion of the viral membrane at the cell surface RECEPTOR VIRUS ICAM-1 polio CD4 HIV acetylcholine rabies EGF vaccinia CR2/CD21 EpsteinBarr herpes HVEM Sialic acid Influenza, reo, corona Receptor-mediated endocytosis of poliovirus The two basic modes of entry of an enveloped animal virus Drugs that Prevent the Virus from Entering or Leaving the Host Cells • Amantadine – interferes with replication of influenza A by inhibiting the transmembrane M2 protein that is essential for uncoating the virus. - Has a narrow spectrum; so, flu vaccine is usually preferable. • Zanamivir – inhibits both influenza A and B neuraminadase. Decr duration of symptoms if given within 48 hr of the onset of symptoms. Prophylactic in healthy adults. • Immunoglobulins – Human Ig contains specific Abs against superficial Ags of viruses can interfere with their entry into host cells. Protection against hepA, measles, and rubellla (German measles). Drugs that Inhibit Nucleic Acid Synthesis Nucleoside and Nucleotide Analogs • Acyclovir- used to treat genital herpes • Cidofovir- used for treatment of cytomegaloviral infections of the eye • Lamivudine- used to treat Hepatitis B Antiviral Drugs Nucleoside and Nucleotide Analogs Figure 20.16a Acyclovir • HSV and VZV contain a thymidine kinase (TK) that acyclovir to a monophosphate phosphorylated by host cell enzymes to acycloguanosine triphosphate, which inhibits viral DNA pol and viral DNA synthesis. • Selectively toxic (TK of uninfected host cells activates only a little of the drug). • Viral enzymes have a much higher affinity than the host enzymes for the drug. • Effective against HSV, but does not eradicate them. • Need high doses to treat shingles. Ganciclovir • Quite toxic (neutropenia) –so, given only for severe CMV infections in immunosuppressed patients. • CMV is resistant to acyclovir because it does not code for TK. Other enzyme inhibitors • Zanamivir (Relenza) and Oseltamivir phosphate (Tamiflu)- inhibitors of the enzyme neuominidase – Used to treat influenza • Indinavir- protease inhibitors. Inhibit the synthesis of essential viral proteins (e.g., RT) by viral-specific proteases. Interferons • Cells infected by a virus often produce interferon, which inhibits further spread of the infection • Alpha-interferon - drug for treatment of viral hepatitis infections Antiviral Drugs Enzyme Inhibitors • Protease inhibitors – Indinavir • HIV • Inhibit attachment – Zanamivir • Influenza • Inhibit uncoating – Amantadine • Influenza • Interferons prevent spread of viruses to new cells • Viral hepatitis Treatment of Herpesviruses Varicella-zoster, Cytomegalavirus, Herpes simplex Anti-metabolites • “False” DNA building blocks or nucleosides. A nucleoside consists of a nucleobase and the sugar deoxyribose. • In antimetabolites, one of the components is defective. In the body, the abnormal nucleosides undergo bioactivation by attachment of three phosphate residues • Acyclovir has both specificity of the highest degree and optimal tolerability, because it undergoes bioactivation only in infected cells, where it preferentially inhibits viral DNA synthesis. Acyclovir • A virally coded thymidine kinase (specific to H.simplex and varicella-zoster virus) performs the initial phosphorylation step; the remaining two phosphate residues are attached by cellular kinases. • Acyclovir triphosphate inhibits viral DNA polymerase resulting in chain termination. It is 30-fold more potent against the virus enzyme than the host enzyme. Acyclovir is active against herpes simplex and varicellarzoster virus. It is rapidly broken down in cells, is orally active and is relatively non-toxic systemically. Acyclovir Acyclovir is used to treat: • Herpes simplex infections (genital herpes, and herpes encephalitis). • Chickenpox in immuno-compromised patients. • Prophylactically in patients treated with immunosuppressant drugs or radiotherapy who are in danger of infection by reactivation of latent virus. • Prophylactically in patients with frequent recurrences of genital herpes. Vidarabine • Inhibits virally induced DNA polymerase more strongly than it does the endogenous enzyme. • Vidarabine is a chain terminator and is active against herpes simplex, varicella zoster, and vaccinia are especially sensitive. • Its use is now limited to topical treatment of severe herpes simplex infection. Before the introduction of the better tolerated acyclovir, vidarabine played a major part in the treatment of herpes simplex encephalitis. • Its clinically used in treatment of immunocompromised patients with herpetic and vaccinia keratitis and in keratoconjunctivitis. Treatment of respiratory virus infection Influenza A & B Respiratory suncytial virus (RSV) Attachment Inhibitors • The primary antiviral mechanism of Amantadine and Rimantadine is to block the viral membrane matrix protein, which function as an ion channel that is required for the fusion of the viral membrane with the cell membrane. • Their clinical use is limited to Influenza A infection. • They are very effective in preventing infection if the treatment is begun at the time of-or prior to- exposure to the virus. Attachment Inhibitors • Side effects of Amantadine are mainly associated with the CNS, such as ataxia and dizziness. • While Rimantadine produce little CNS effect because it does not penetrate the blood brain barrier. • Both should be used with caution in pregnant and nursing women. Neuroaminidase inhibitors Oseltamivir and Zanamavir Mechanism of action • Viral neuraminidase catalyzes cleavage of terminal sialic acid residues attached to glycoproteins and glycolipids, a process necessary for release of virus from host cell surfaces. •Neuraminidase inhibitors thus prevent release of virions from infected cell 40 Neuroaminidase inhibitors • Administration of neuraminidase inhibitors is a treatment that limits the severity and spread of viral infections. • Neuraminidase inhibitors are useful for combating influenza infection: zanamivir, administered by inhalation; oseltamivir, administered orally. • Toxicities – Exacerbation of reactive airway disease by zanamavir – Nausea and vomiting for oseltamivir Antiretroviral agents Antiretrovirals • Currently implies a drug used to treat HIV • Tenofovir- nucleotide reverse transcriptase inhibitor • Zidovudine- nucleoside analog – inhibits RT of HIV and is only used orally for AIDS. - Activated by triple phosphorylation and then binds RT (with100X affinity than for cellular DNA pols). - Incorporated into the DNA chain, but lacks a 3’OH; so another nucleoside cannot form a 3’-5’-phosphodiester bond DNA chain elongation is terminated. -Severe adverse effects: anemia, neutropenia, myalgia, nausea, and headaches. • Stavudine, didanosine, zalcitabine – among other NRTIs. • Nevirapine, efavirenz – Non nucleoside RTIs - denature RT. Life Cycle of HIV HIV gp41-mediated fusion and enfuvirtide (T-20) action – Prohibits HIV entry HIV Life Cycle Step 1: Fusion HIV Step 3: Integration reverse transcriptase Step 5: Packaging and Budding Step 2: Transcription Step 4: Cleavage Azidothymidine (Zidovudin(AZT)) • It is a potent antagonist of reverse transcriptase, It is a chain terminator. • Cellular enzyme phosphorylate AZT to the triphosphate form which inhibits RT and causes chain termination • It is widely use in the treatment of AIDS (The only clinical use). • AZT is toxic to bone marrow, for example, it cause severe anaemia and leukopenia In patient receiving high dose. Headache is also common Didanosine (Dideoxyinosine) • Didanosine act as chain terminators and inhibitors of reverse transcriptase because they lack a hydroxyl group. • is phosphorylated to the dideoxyadenosine triphosphate active metabolite of • It is used in the treatment of AIDS (second drug approved to treat HIV-1 infection). • They are given orally, • and their main toxicities are pancreatitis, peripheral neuropathy, GI disturbance, bone marrow depression. Abacavir • Abacavir is a guanosine analog (Figure 49–2) that is well absorbed following oral administration (83%) and is unaffected by food. The serum half-life is 1.5 hours. The drug undergoes hepatic glucuronidation and carboxylation. Cerebrospinal fluid levels are approximately one third those of plasma. • Abacavir is often co-administered with lamivudine, and a once-daily, fixeddose combination formulation is available. Abacavir is also available in a fixed-dose combination with lamivudine and zidovudine. • High-level resistance to abacavir appears to require at least two or three concomitant mutations and thus tends to develop slowly. • Hypersensitivity reactions, occasionally fatal, have been reported in up to 8% of patients receiving abacavir and may be more severe in association with once-daily dosing. • All NRTIs may be associated with mitochondrial toxicity, probably owing to inhibition of mitochondrial DNA polymerase gamma. Less commonly, lactic acidosis with hepatic steatosis may occur, which can be fatal. NRTI treatment should be suspended in the setting of rapidly rising aminotransferase levels, progressive hepatomegaly, or metabolic acidosis of unknown cause. The thymidine analogs zidovudine and stavudine may be particularly associated with dyslipidemia and insulin resistance. Also, some evidence suggests an increased risk of myocardial infarction in patients receiving abacavir or didanosine; this bears further investigation. Non-nucleoside Non-competitive RT inhibitors (1) bind to viral RT, inducing conformational changes that result in enzyme inhibition (2) Combination therapy with AZT (resistant mutants rapidly emerge, little use in monotherapy) (3) Resistance mutations will be at different sites Generic Name Nevirapine Trade Name Viramune Delavirdine Rescriptor Usual Dose 200 mg QD x14 days, then 200 mg BID 400 mg TID Efavirenz SustivaTM 600 mg QD 51 Non-nucleoside Non-competitive RT inhibitors Nevirapine Approved for AIDS patients, Good blocker of mother to child transmission (perinatal - breast feeding) • Single dose at delivery reduced HIV transmission by 50% • Single dose to baby by 72 hours NNRTI’s: Adverse Effects RASH!! CNS effects (e.g. sedation, insomnia, vivid dreams, dizziness, confusion, feeling of “disengagement”) 52 Rash Rash, usually a maculopapular eruption that spares the palms and soles, occurs in up to 20% of patients, usually in the first 4–6 weeks of therapy. Although typically mild and self-limited, rash is dose-limiting in about 7% of patients. Women appear to have an increased incidence of rash. When initiating therapy, gradual dose escalation over 14 days is recommended to decrease the incidence of rash. Protease Inhibitors • HIV Protease Inhibitors; have significantly alter the course of the HIV disease. • All are reversible inhibitors of HIV Protease-the viral enzyme responsible for cleavage of viral polyprotein into number of essential enzymes (reverse transcription, polymerase). • Examples are : Saquinavir, and Ritonavir. • They are orally active, side effects include GI disturbances and hyperglycemia, interact with cytochrome P450. buffalo hump Anti-Viral Chemotherapy GAG/POL polyprotein GAG Integrase Polymerase Protease Retrovirus --- HIV 55 Anti-Viral Chemotherapy GAG Integrase Polymerase Protease folds and cuts itself free 56 Anti-Viral Chemotherapy GAG Integrase Polymerase Protease cuts at a site between the integrase and polymerase 57 Anti-Viral Chemotherapy GAG Integrase polymerase 58 New targets • Agents that block fusion of HIV with the host cell by interacting with gp41 • Enfuvirtide is Peptides derived from gp41 can inhibit infection, probably by blocking the interaction of gp41 with cell membrane proteins during fusion. • Raltegravir (Integrase Inhibitor) targets integrase, an HIV enzyme that integrates the viral genetic material into human chromosomes, a critical step in the pathogenesis of HIV. • Maraviroc It blocks the interaction between chemokine receptor CCR5 and HIV gp120. (HAART) • Highly active anti-retroviral therapies • Combination therapies (triple drug cocktail, HAART) are very effective and can reduce viral load in the patient below detectable levels implying that HIV replication has ceased. examples (1) NNRTI–Based Regimens (1-NNRTI + 2NRTIs) (2) PI-Based Regimens (1 or 2 PIs + 2 NRTIs) • The trouble with all of these complicated drug regimens is compliance. The components of HAART must be taken at different times. • Non-compliance with protease inhibitor therapy is of serious concern as the new virus that emerges is resistant to the inhibitor being taken and also resistant to other protease inhibitors. Figure 2. Timeline of evolution of HBV therapies, United States. Anti-Hepatitis B Virus Agents Interferons • Interferon Alfa • Endogenous proteins induce host cell enzymes that inhibit viral RNA translation and cause degradation of viral mRNA and tRNA . • Bind to membrane receptors on cell surface , May also inhibit viral penetration, uncoating, mRNA synthesis, and translation, and virion assembly and release. • Pegylated interferon Alfa • A linear or branced polyethylene gylcol (PEG) moiety is attached covalently to interferon • Increased half-life and steady drug concentrations Interferon, mechanism of action: • 1) binds to cell surface receptors • 2) induces expression of translation inhibitory protein (TIP) • 3) TIP binds to ribosome, inhibits host expression of viral proteins Interferons • a limited treatment course (ie, only 1 year of therapy), • lack of resistance development. • Disadvantages include a high rate of treatment-related adverse events. flu-like symptoms: increased body temperature, feeling ill, fatigue, headache, muscle pain. Anti-Hepatitis B Virus Agents • ……. • Entecavir and tenofovir have very strong resistance profiles in treatment-naive patients. • Disadvantages include the need to continue therapy indefinitely and the potential for resistance development. Anti-Hepatitis C Virus Agents • Approved – Interferon-alpha (pegylated) – Ribavirin • In development – Protease inhibitors – Polymerase inhibitors • In pregnancy , a regimen of oral zidovudine beginning between 14 and 34 weeks of gestation, intravenous zidovudine during labor, and zidovudine syrup to the neonate from birth through 6 weeks of age has been shown to reduce the rate of vertical (motherto-newborn) transmission of HIV by up to 23%. Kirby-Bauer Method for Determining Drug Susceptibility 1. Bacteria spread on surface of agar plate 2. 12 disks, each with different antimicrobial drug, placed on agar plate 3. Incubated- drugs diffuse outward and kill susceptible bacteria 4. Zone of inhibition around each disk 5. Compare size of zone to chart Figure 21.10 Resistance to Antimicrobial Drugs • Drug resistance limits use of ALL known antimicrobials • Penicillin G: first introduced, only 3% of bacteria resistant • Now, over 90% are resistant Mechanisms Responsible for Resistance to Antimicrobial Drugs Include the Following: 1. Inactivating enzymes that destroy the drug (e.g., β-lactamases). 2. Decreased drug accumulation (e.g., tet). 3. Altering the binding sites (e.g., aminoglycosides and erythromycin). 4. Development of alternative metabolic pathways (sulphonamides ( dihydropteroate synthease) and trimethoprim (dihydrofolate reductase). How do Bacteria Become Resistant? 1. Spontaneous Mutation: happen as cells replicate – Within a pop, there will be some bact with acquired resistance. The drug then elim the sensitive organisms, while the resistant ones proliferate. 2. Gene Transfer or Transferred resistance: Usually spread through conjugative transfer of R plasmid ( may be virally mediated). Slowing the Emergence and Spread of Antimicrobial Resistance 1. Responsibilities of Physicians: must work to identify microbe and prescribe suitable antimicrobials, must educate patients 2. Responsibilities of Patients: need to carefully follow instructions Slowing the emergence and spread of antimicrobial resistance 3. Educate Public: must understand appropriateness and limitations of antibiotics; antibiotics not effective against viruses 4. Global Impacts: organism that is resistant can quickly travel to another country - in some countries antibiotics available on non-prescription basis - antibiotics fed to animals can select for drugresistant organisms New Approaches to Antibiotic Therapy Are Needed • Scientists work to find new antibiotic targets in pathogens • Discovery of new and unique antibiotics is necessary