1 - Detroit Medical Center
advertisement

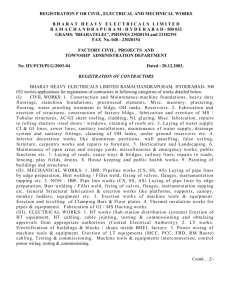
PHYSIOLOGY OF PENILE ERECTION AND PATHOPHYSIOLOGY OF ERECTILE DYSFUNCTION Campbell’s Chapter 21 Roc McCarthy, DO Physiology of Penile Erection • • • • • • Historical Aspects First description of erectile dysfunction dates from about 2000 BC types: natural - the man is incapable of accomplishing sex supernatural - evil charms and spells - Two Aristotle- three nerves carry spirit and energy to the penis, erection is produced by influx of air Leonardo da Vinci (1504) noted a large amount of blood in the erect penis of hanged men and cast doubt on the concept of the air-filled penis Many theories have since been added to explain the hemodynamic events during erection and detumescence. -In the 19th century, venous occlusion was thought to be the main factor in achieving and maintaining erections Much of the current understanding of erectile physiology wasn’t gained until the 1980s and 1990s Functional Anatomy of the Penis • • • 3 cylindrical structures - paired corpora cavernosa corpus spongiosum (which houses the urethra), covered by a loose subcutaneous layer and skin. Flaccid length is controlled by the contractile state of the erectile smooth muscle (varies considerably) - depending on emotion and outside temperature Neither age nor the size of the flaccid penis accurately predicts erectile length Tunica Albuginea • • • Tunica affords great flexibility, rigidity, and tissue strength to the penis Tunica covering of the corpora cavernosa- bilayered structure with multiple sublayers. - Inner-layer bundles support and contain the cavernous tissue and are oriented circularly. Radiating from this inner layer are intracavernous pillars that act as struts, provide support Outer-layer bundles are oriented longitudinally Corpus spongiosum lacks the outer layer and intracorporeal struts Tunica Albuginea • • • Emissary veins run between the inner and outer layers for a short distance, often piercing the outer bundles obliquely Variability in tunical thickness and strength 6-7 o'clock positions, thickness is 0.8 ± 0.1 mm -9 o'clock position, 1.2 ± 0.2 mm -11 o'clock position, 2.2 ± 0.4 mm The most vulnerable area is located on the ventral groove (between the 5 and 7 o'clock positions), where the longitudinal outer layer is absent; most prostheses tend to extrude here External Penile Support • 2 ligamentous structures: 1. fundiform ligament arises from Colles' fascia and is lateral, superficial, and not adherent to the tunica albuginea of the corpora 2. suspensory ligament arises from Buck's fascia and consists of two lateral bundles and one median bundle, which circumscribe the dorsal vein of the penis. Its main function is to attach the tunica albuginea of the corpora cavernosa to the pubis Corpora Cavernosa, Corpus Spongiosum, and Glans Penis • • • Septum between the two corpora cavernosa is incomplete Flaccid state, the blood slowly diffuses from the central to the peripheral sinusoids and the blood gas levels are similar to those of venous blood. Erect, the rapid entry of arterial blood to both the central and the peripheral sinusoids changes the intracavernous blood gas levels to those of arterial blood Arteries • • • Penile blood supply- the internal pudendal artery (off internal iliac artery) → common penile artery 3 branches- dorsal, bulbourethral, and cavernous Dorsal artery is responsible for engorgement of the glans during erection Veins Venous drainage from the three corpora originates in tiny venules leading (from sinusoids) exiting as the emissary veins Hemodynamics and Mechanism of Erection and Detumescence • • • Corpora Cavernosa In the flaccid state, these smooth muscles are tonically contracted, allowing only a small amount of arterial flow for nutritional purposes Phases of erection: (1) dilation of the arterioles and arteries by increased blood flow (2) trapping of the incoming blood by the expanding sinusoids (3) compression of the subtunical venous plexuses, reducing venous outflow (4) stretching of the tunica to its capacity, which occludes the emissary veins (decreases venous outflow to a minimum) (5) PO2 increases- 90 mm Hg (6) Intracavernous pressure increases to 100 mm Hg (7) Penis raises to erect state Blood flow and intracavernous pressure changes during the seven phases of penile erection and detumescence 0, flaccid; 1, latent; 2, tumescence; 3, full erection; 4, rigid erection; 5, initial detumescence; 6, slow detumescence; 7, fast detumescence. Corpus Spongiosum and Glans Penis During erection, the arterial flow increases in a similar manner - however, the pressure in the corpus spongiosum and glans is only one third to one half that in the corpora cavernosa - No outer longitudinal tunic layer (no venous occlusion) Neuroanatomy and Neurophysiology of Penile Erection • • • • Peripheral Pathways Innervation of the penis is both autonomic (sympathetic and parasympathetic) and somatic (sensory and motor) Sympathetic and parasympathetic nerves merge to form the cavernous nerves - effect the neurovascular events during erection and detumescence Somatic nerves- 1° responsible for sensation and the contraction of the bulbo/ischio-cavernosus muscles Autonomic Pathways • • • Sympathetic pathway originates from the 11th thoracic to the 2nd lumbar spinal segments Parasympathetic pathway arises from S2-S4 Cavernous nerves are branches of the pelvic plexus that innervate the penis cavernous nerves are easily damaged during radical excision of the rectum, bladder, and prostate Autonomic Pathways • • • Stimulation of the PNS cavernous nerves induces erection, whereas stimulation of the sympathetic trunk causes detumescence Sacral spinal cord injury retain psychogenic erectile ability even though reflexogenic erection is abolished No psychogenic erection occurs in patients with lesions above T9 Somatic Pathways The somatosensory pathway originates at the sensory receptors in the penile skin, glans, and urethra and within the corpus cavernosum The free nerve endings are derived from thin myelinated Aδ and unmyelinated C fibers Nerve fibers from the receptors converge to form bundles of the dorsal nerve of the penis, which joins other nerves to become the pudendal nerve Onuf's nucleus in the second to fourth sacral spinal segments is the center of somatomotor penile innervation Contraction of the ischiocavernosus muscles produces the rigiderection phase. Rhythmic contraction of the bulbocavernosus muscle is necessary for ejaculation Neurotransmitters α-Adrenergic nerve fibers and receptors norepinephrine has generally been accepted as the principal neurotransmitter to control penile flaccidity and detumescence Endothelin, a potent vasoconstrictor produced by the endothelial cells, has also been suggested to be a mediator for detumescence Flaccidity and Detumescence Intracorporeal smooth muscle in a semicontracted (flaccid) state results from three factors: 1) Intrinsic myogenic activity 2) Adrenergic neurotransmission 3) Endotheliumderived contracting factors such as angiotensin II, PGF2α, and endothelins Detumescence after erection may be a result of cessation of NO release, the breakdown of cyclic guanosine monophosphate (cGMP) by phosphodiesterases, or sympathetic discharge during ejaculation Erection NO released from nonadrenergic, noncholinergic neurotransmission and from the endothelium is the principal neurotransmitter mediating penile erection NO increases the production of cGMP, which in turn relaxes the cavernous smooth muscle VIP Central Neurotransmitters and Neural Hormones A variety of neurotransmitters (dopamine, norepinephrine, 5hydroxytestosterone [5-HT], and oxytocin) and neural hormones (oxytocin, prolactin) have been implicated in regulation of sexual function. Dopamine- Apomorphine, which stimulates both D1 and D2 receptors, induces erection that is unaccompanied by sexual arousal Serotonin- 5-HT pathways inhibit copulation but that 5-HT may have both facilitory and inhibitory effects on sexual function Norepinephrine- Central norepinephrine transmission seems to have a positive effect on sexual function γ-Aminobutyric acid (GABA), Opioids, Oxytocin, Nitric Oxide, Melanocortins, Prolactin Molecular Mechanism of Smooth Muscle Contraction Molecular Mechanism of Smooth Muscle Relaxation KEY POINTS: SMOOTH MUSCLE RELAXATION CAUSES ERECTION Relaxation of the cavernous smooth muscle is the key to penile erection. Nitric oxide release initiates the erection process, and helps maintain erection. Upon entering the smooth muscle cells, NO stimulates the production of cGMP. Cyclic GMP activates protein kinase G, which in turn opens potassium channels and closes calcium channels. Low cytosolic calcium favors smooth muscle relaxation. The smooth muscle regains its tone when cGMP is degraded by phosphodiesterase PATHOPHYSIOLOGY OF ERECTILE DYSFUNCTION Incidence and Epidemiology Diokno and associates reported that 35% of married men aged 60 years and older suffer from erectile impotence MMAS study, between the ages of 40 and 70 years, the probability of complete ED increased from 5.1% to 15%, moderate dysfunction increased from 17% to 34%, and mild dysfunction remained constant at about 17%. Worldwide prevalence of ED, 24 international studies were reported between 1993 and 2003 - Before age 40 the rate was 1% to 9% - From 40 to 59 it ranged from 2% to 9% to as high as 20% to 30% Risk Factors for ED General health status Diabetes mellitus Cardiovascular disease Concurrence of other GU diseases Psychiatric or psychological disorders Chronic diseases Smoking Medications Hormonal factors also serve as well-defined risk factorassociated conditions Classification of Male Erectile Dysfunction Organic I. Vasculogenic, Arteriogenic, Cavernosal, Mixed II. Neurogenic III. Anatomic IV. Endocrinologic Psychogenic I. Generalized A. Generalized unresponsiveness 1. Primary lack of sexual arousability related decline in sexual arousability Generalized inhibition 1. Chronic disorder of sexual intimacy II. Situational A. Partner-related 1. Lack of arousability in specific relationship 2. Lack of arousability owing to sexual object preference 3. High central inhibition owing to partner conflict or threat B. Performance-related Associated with other sexual dysfunction/s (e.g., rapid ejaculation) Situational performance anxiety (e.g., fear of failure) Psychological distress- or adjustment-related negative mood state (e.g., depression) 2. AgingB. 1. 2. C. 1. Associated with Psychogenic Previously, psychogenic impotence was believed to be most common, thought to affect 90% of impotent men Two possible mechanisms have been proposed to explain the inhibition of erection in psychogenic dysfunction: 1) direct inhibition of the spinal erection center by the brain as an exaggeration of the normal suprasacral inhibition 2) excessive sympathetic outflow or elevated peripheral catecholamine levels Neurogenic 10% to 19% of ED is neurogenic MPOA, the PVN, and the hippocampus are important integration centers for sexual drive and erection, and pathologic processes in these regions, such as Parkinson's disease, stroke, encephalitis, or temporal lobe epilepsy, are often associated with ED. In men with a spinal cord injury, its nature, location, and extent largely determine erectile function Reflexogenic erection is preserved in 95% of patients with complete upper cord lesions Introduction of nerve-sparing radical prostatectomy has reduced the incidence of impotence from nearly 100% to 30% to 50% - Recovery of erectile function after radical pelvic surgery can take 6 to 24 months. Early treatment with intracavernous alprostadil or oral sildenafil has been shown to improve recovery Endocrinologic Hypogonadism is a not-infrequent finding in the impotent population Mulligan and Schmitt (1993) concluded that testosterone (1) enhances sexual interest (2) increases the frequency of sexual acts (3) increases the frequency of nocturnal erections but has little or no effect on fantasy-induced or visually stimulated erections Treatment with flutamide, estradiol, or a gonadotropin-releasing hormone antagonist in addition to castration further depresses the erectile response Hyperprolactinemia, whether from a pituitary adenoma or drugs, results in both reproductive and sexual dysfunction Arteriogenic Atherosclerotic or traumatic arterial occlusive disease of the hypogastriccavernous-helicine arterial tree can decrease the perfusion pressure and arterial flow to the sinusoidal spaces, thus increasing the time to maximal erection and decreasing the rigidity of the erect penis Common risk factors associated with arterial insufficiency include hypertension, hyperlipidemia, cigarette smoking, diabetes mellitus, blunt perineal or pelvic trauma, and pelvic irradiation Focal stenosis of the common penile or cavernous artery is most often seen in young patients who have sustained blunt pelvic or perineal trauma Long-distance cycling is also a risk factor for vasculogenic and neurogenic ED Hypertension Hypertension is an independent risk factor for ED Cardiovascular complications such as ischemic heart disease and renal failure are associated with even higher ED prevalence Mechanism of Vascular Erectile Dysfunction Increased peripheral vascular resistance Enhanced basal and myogenic tone has been observed in arteries Cavernous (Venogenic) Failure of adequate venous occlusion has been proposed as one of the most common causes of vasculogenic impotence Veno-occlusive dysfunction may result from a variety of pathophysiologic processes: degenerative tunical changes, fibroelastic structural alterations, insufficient trabecular smooth muscle relaxation, and venous shunts. Degenerative changes (Peyronie's disease, old age, and diabetes) or traumatic injury to the tunica albuginea (penile fracture) can impair the compression of the subtunical and emissary veins Structural alterations in the fibroelastic components of the trabeculae, cavernous smooth muscle, and endothelium may result in venous leakage Loss of compliance of the penile sinusoids associated with increased deposition of collagen and decreased elastic fiber may be seen in diabetes, hypercholesterolemia, vascular disease, penile injury, or old age Antihypertensive Agents Diuretics- Thiazides showed a significant increase in ED when compared with placebo - Treatment of Mild Hypertension Study (TOMHS), in which the prevalence of ED at 2 years in men taking low-dose thiazide was twice that of those taking placebo or alternative agents (Grimm et al, 1997). (After 4 years of treatment, the prevalence of ED in the placebo group approached that of the thiazide group……may be that thiazide therapy, rather than causing ED directly, unmasks it at an earlier stage β-Adrenergic Blockers- 10% of adrenoceptors in the penile tissue are of the β type, and their stimulation is thought to mediate relaxation -β antagonists also exert an inhibitory effect within the CNS, perhaps leading to lowered sex hormone levels - nonselective drugs such as propranolol were associated with a higher prevalence of ED than placebo or ACE inhibitor. - Newer agents with higher selectivity for the β1 adrenoceptor, such as acebutolol, have shown a substantial reduction in ED Antihypertensive Agents α-Adrenoceptor Blockers- positive effect on erection for α antagonists, particularly those acting on the α1 receptor - drugs such as doxazosin were not associated with complaints of ED Angiotensin-Converting Enzyme Inhibitors- Lack any easily appreciated peripheral or central effect that would interfere with sexual function - ACE inhibitor captopril did not cause any significant adverse effect on sexual function Angiotensin II receptor antagonists, have a beneficial effect on existing sexual dysfunction at baseline Calcium Channel Blockers- no adverse effect on erection Antipsychotics- varies Antidepressants- neg Selective serotonin reuptake inhibitors (SSRIs)- SSRIs differ in their ability to cause ED. A high incidence has been observed in patients treated with paroxetine (Kennedy et al, 2000), and a lesser impact has been reported with citalopram Antiandrogens These drugs cause partial or near-complete blockade of androgen's action by inhibiting production of or antagonizing the androgen receptor (AR) The effects of androgen deficiency on sexual activity are variable, ranging from complete loss to normal function the 5α-reductase inhibitor finasteride (5 mg daily) for prostatic symptoms, approximately 5% complained of decreased desire and ED compared with 1% in the placebo group (Gormley et al, 1992). At the lower dose used to treat male-pattern alopecia (1 mg daily), no sexual dysfunction was seen Nonsteroidal antiandrogens when combined with an LHRH agonist, reduce sexual desire occurs in up to 70% patients Miscellaneous Drugs Digoxin Statins? Histamine H2 Receptor Antagonists Opiates Retroviral and Chemotherapeutic Agents Tobacco and Alcohol Diabetes Mellitus Common chronic disease, affecting 0.5% to 2% worldwide Prevalence of ED is three times higher in diabetic men (28% versus 9.6%) In 12% of diabetic men, deterioration of sexual function can be the first symptom Chronic Renal Failure Sexual dysfunction has been reported in 20% to 50% of men with chronic renal failure 45% prevalence of self-reported severe ED among men receiving hemodialysis Uremia decreases NO bioavailability Primary Erectile Dysfunction Primary ED refers to a lifelong inability to initiate or maintain erections, or both, beginning with the first sexual encounter Physical cause resulting from mal-development of the penis or the blood and nerve supply Micropenis- self explanatory The End