Conslidated Sub-District Change Package for Teaching
advertisement

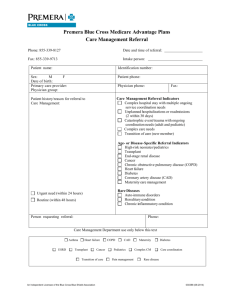
Wave 4: Consolidated Sub District Change Package Through Pictures PRIMARY SYSTEM DRIVERS OF IMPROVED HEALTH Seeking and obtaining care early Accelerate reduction of Under-5 mortality in Ghana by 60% before 2015 using QI methods HEALTH SYSTEM DESIGN FEATURES COMMUNITY Risk Awareness/Management Enhanced Value of Lives Financial /NHI Subscription Proximity to Health Services Attractiveness of Health Services Providing prompt, appropriate, adequate & client-centred care HEALTH FACILITY Staff Attitude & Behaviour Staff Clinical Knowledge & Skills Protocol Adherence Staff Availability Reliable Referral System CULTURE OF QUALITY Develop culture of and capacity for continuous improvement using reliable health data Use of Local Data to Drive Performance Improvement Regular Supervision, Coaching & Mentoring Appropriate Data Capture & Transmission Tools CHANGE INTERVENTIONS S Aides Client Self-Management & Family Education Emergency Preparedness Community Education & Mobilization Outreach & Domiciliary Services Client-centred Design Acuity-oriented Design Staff Training, Practice & Monitoring Reminder Systems Supply Chain Management Staff Re-scheduling, Reassignment & Taskshifting Communications & Transport System Application of QI methods at Local Level Longitudinal Data Quality Assessments Longitudinal Facilitative Supervision Development & Use of Client Registers, Reporting Forms, Databases etc. Outcome Complexity of problem? Primary Drivers Individual & Family Barriers Secondary Drivers Delay in decision to seek skilled care (recognition, permission, financial etc.) Delay in acceptance of referral Low risk awareness & management of obstetric/neonatal complications Sociocultural Barriers Preference for home/TBA deliveries and self-medication (hospital as last resort) Negative perceptions about health facilities as places to “go and die” Insufficient funds for transport & telephone credits (both family & staff) Maternal and Neonatal Mortality Due to Faulty Referral Processes Transportation & Communication Barriers Unavailability of local transportation Inadequate ambulance services Unreliable telecom services Long distances, poor or no roads/bridges Late/no identification of high-risk clients Failure to stabilize client before referral Inadequate Clinical Skills & Management Lack of readiness of receiving facility Poor hand-off management processes Poor documentation of indications for referral & interventions to date Delay in providing care Governance & Accountability Unreliable use of referral protocols Inadequate supervision, monitoring Antenatal Care MNH Danger Sign Recognition at the Community: Training and health education of pregnant women and community-based health providers on danger sign recognition: • The midwife attended monthly meetings of TBAs and trained them on: – a. recognition of maternal & newborn danger signs – b. the need for prompt referral on recognition of any of these danger signs • During ANC sessions the midwife also educated pregnant women on danger signs and encouraged early care seeking • Midwife and other QI team members educated LCS and spiritualists on MNH danger signs Care-Seeking Behavior for ANC Health education for identifiable community groups: • Health staff hold monthly talks with spiritualist, MTMSGs, women’s group meetings and pregnant women on: – – – danger signs in pregnancy importance of early care seeking address fears of early ANC registration • Health staff identified pregnant women at home visits and registered them, followed by registration for NHIS by NHIA ANC Registration in 1st Trimester: • Community stakeholder meetings with opinion leaders and other influential groups about the importance of early and regular ANC • Community stakeholder meetings followed by registration of pregnant women by community volunteers on monthly basis At Least Four ANC Visits Before Delivery: • Increase the number of days ANC is offered at static site AND re-design clinic processes to reduce visit duration per client to <1 hr • Offer ANC as outreach service as well as at static site AND re-design clinic processes to reduce visit duration per client to <1 hr Skilled Delivery Care Seeking Behavior for Skilled Delivery Mobilizing Transport: • Engagement of motor-bike owners within specific communities to assist with transporting women in labour and sick newborns to the clinic Engaging Men: • Men engaged to accompany their wives to ANC in order to be present for discussion on BPP: – The Imam, during prayers at the mosque, encouraged men to attend ANC with their wives. – For those men who did the ANC visit with their wives, the health staff used the visit as a means for reinforcing the referral aspect of the BPP (Birth Preparedness Planning). • Male advocacy group in communities to promote skilled delivery Care Seeking Behavior for Skilled Delivery • Motivate TBAs with half bar soap and the other half to the mother who delivered at the facility Redefinition of TBAs role: • Chief threatened to fine those who delivered at home • Educated community members on obstetric complications and announced that TBAs will be allowed to support deliveries in the clinic • TBA directing clients to CHPS and supporting CHNs in the delivery. Clinic motivates the TBA with half bar of soap Care Seeking Behavior for Skilled Delivery TBAs /community engagement: • Health staff held interactive meetings with TBAs & spiritualist on benefits of early care especially for neonates & labour and explained the dangers of unskilled delivery. • Using community durbars the midwife and other QI team members explained benefits of facility delivery. • Using daily home visit and personal carers approach, a pregnant woman was assigned to a health worker to encourage them and take personal responsibility for the woman to deliver at the facility • Health staff hold monthly family conversation involving mother-in-laws, husband and other family members to agree on facility delivery Care Seeking Behavior for Skilled Delivery • Video show in communities on the risks of labor & delivery • TBA engagement on risks of unskilled delivery and provide incentives Skilled Delivery & Immediate Postnatal Care • Provide domiciliary delivery if, upon notification by mobile phone, labor too advanced, woman has no means of transport from community or health staff cannot arrange transport from clinic or hospital • Use ANC register to identify women at 36+ weeks gestation for home visits to remind them & family members about skilled delivery • Create a welcoming, patient-friendly environment in health facility for labouring women Skilled Delivery & Immediate Postnatal Care • Create systems to ensure consistent and correct use of partographs • Create systems for reliable neonatal resuscitation Postnatal Care Postnatal Care on Day 1 & 2 • If facility skilled delivery: detain for observation for 24hrs if possible. If not, discharge after minimum of 6 hrs and follow-up on Day 2 with facility or home visit • If domiciliary skilled delivery: followup on Day 2 with facility or home visit • If unskilled delivery: ask family members or volunteers to notify health staff immediately by mobile phone/bicycle/motorbike. Woman comes to facility on Day 1 if possible or health staff follow-up with home visit on Day 1 or 2 Postnatal Care on Day 6 & 7 • During Day 1 & 2 visit, make appointment for Day 6/7 visit at facility or home. Use reminder systems at community, clinic/hospital to improve reliability • If a woman lives in different sub-district or distant community within CHPS Zone, refer to other sub-district or CHO for Day 6/7 visit. Contact CHO to follow up if no show. • If woman lives in distant community without CHO AND return facility visit not possible AND health staff home visit not possible, train IMCI volunteers to provide Day 6/7 care Referral Compliance Referral Compliance Focused ANC: • A health worker is assigned to take personal responsibility for a pregnant woman or a group of women to specifically ensure they have a skilled delivery. • Midwife and other QI members educated community on importance of referral compliance, early care seeking and facility delivery. The midwife also used monthly TBAs meeting to explain importance of early care seeking • Using MOTECH (mobile messaging service) facility the midwife+ CHN sent reminders to pregnant women about facility delivery and contingency plan in case of referral • Health staff conducted home visits twice a day to discuss the importance of referrals and benefits of facility delivery Socio-cultural Barriers Referral Compliance Community mobilization: (1)Health talks in churches & mosque, to groups of men playing games, men on farms, men’s fun club on: • • • the importance of male involvement in health care barriers to referrals referral compliance wrong perceptions about facility delivery and general maternal and newborn health issues (2)Used community information center, to educate the community on importance of referrals and benefits of early care seeking Referral Compliance Birth Preparedness Plan with Motivation: • Health staff at ANC educated pregnant mothers on the importance of BPP. • Pregnant women engaged, individually, on the various items on BPP at home and facility explaining the need & use for each item • Health staff inspect various items prepared by family from the BPP list during home visit and emphasizes the need to save for transport in case of referral and talk with husbands to support • Welcome package (baby dresses) is also presented to mothers who delivered at the health facility as a way of motivating women to have skilled delivery Transportation Transportation Community-based emergency transport solution: • Influential QI team members led a meeting with transport owners to discuss the need to provide emergency transport for maternal and neonatal cases. • Phone numbers of drivers distributed to pregnant women during ANC, TBAs & CBV during community meetings • To complement the efforts of health staff, volunteers are coached and tasked to talk to pregnant women in the community to put money aside for emergency transport. • QI team then used community durbars to educate the community about referrals and disseminated information about the transport arrangement with GPRTU for emergency referrals Transportation Community-based transport solution: • QI team met with GPRTU to reactivate MOU and reached an agreement to provide emergency transport services for maternal and newborn cases • At community meetings and durbars, QI team explained why patients should accept referrals. The community chief then announced the availability of community transport for mothers and neonates in case of emergency. • QI team mobilize funds from churches to support mothers who cannot pay for transport. • Team dialogued with the police to use their vehicle in case of emergency and to allow a quick pass for taxis carrying maternal emergency cases at night Transportation Community-based transport solution: • MA & Midwife engaged GPRTU with baseline performance on emergency transport response time & agreed to reduce delay of emergency referrals reaching the next level. • Updated drivers’ phone numbers to be contacted for emergency transport. Phone numbers were pasted on a wall of the health facility for easy access by all staff. • Quarterly meetings held with the drivers to discuss progress and give feedback for improvement. Communication Communication Feedback & Pre-Referral Communication Methods: • Midwife or any health worker referring calls the receiving facility to obtain information about the condition of patient • Health staff do a follow up (face to face ) with patients families to ascertain condition and then document feedback in referral register • DDHS provided resources (phone & credit) and then mandated health staff to call referral facility for feedback Communication Documentation: Stock and Supplies • DHMT photocopied referral & feedback forms for all facilities • Health system printed and distributed triplicate referral forms + feedback forms to all facilities Communication Referral documentation: • Using sub district review meeting and LS, the medical superintendent educated health workers on how to fill the referral form whenever they are referring a patient to the hospital • Using mortality audit sessions, the medical superintendent educated health professionals on proper referral documentation Communication Feedback Verbal feedback: • Names of referred clients are picked by health staff according to community before departing for outreach. • Staff conducts follow up visits to the homes of those referred to check compliance and final diagnosis during the outreach. Communication Feedback Verbal feedback: • The midwife or any health worker referring called the receiving facility to obtain information about the condition of patient. • Health staff followed up to patient’s family to ascertain the patient’s condition and documented feedback in referral register. Communication Feedback Verbal & written feedback: • The hospital's HIO collected feedback forms every week and put them in the respective pigeon holes of referring facilities at the DHMT. • Facilities referring without the necessary documentation on the referral form are notified on phone and feedback given to them during LS/performance review meeting to improve Communication Feedback Electronic & written feedback: • Using social media such as WhatsApp, the HIO sent feedback to referring facilities weekly • Focal person at the hospital later sent written feedback to the DHMT for onward collection by health facilities • District director gives directive for sub district facilities to procure Vodafone landline so that the hospital can send verbal feedback