4th Floor Sherbrooke Centre Tel (604) 520
advertisement
 520")
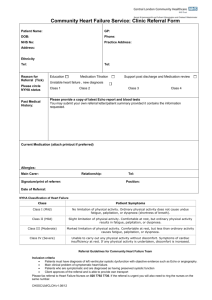
4th Floor Sherbrooke Centre New Westminster, BC V3L 3M2 Canada Tel (604) 520-4662 Fax (604) 520-4871 www.fraserhealth.ca REFERRAL FORM – NEUROPSYCHOLOGICAL ASSESSMENT SERVICES Date of Referral (dd/mm/yr): PHN: Last Name: First Name: DOB (dd/mm/yr): Address: City: Home Phone: Occupation Status: Please circle: Inpatient Outpatient Floor _____ First Language: Interpreter Needed: Y N If they cannot be seen as an inpatient, do you want them seen as an outpatient? Y N PLEASE PRINT LEGIBLY Referral Source (Name of Person and Site): Phone: Address: Fax CURRENT DIAGNOSIS: __________________________________________________________________________________________________ CURRENT MEDICATIONS: _______________________________________________________________________________________________ ______________________________________________________________________________________________________________________ REFERRAL QUESTION (Please be as specific): ______________________________________________________________________________ ______________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________ ______________________________________________________________________________________________________________________ PLEASE CHECK ALL APPLICABLE: Attention/Concentration Problems Memory Problems Problems with Orientation Seizures/Seizure-Like Symptoms History of Traumatic Brain Injury (TBI) Intellectual Functioning History of Loss of Consciousness (LOC) Significant Medical Problems – Specify______________________________________________________________________ Neurological Disorder – Specify ____________________________________________________________________________ Other Observed Cognitive Problems – Specify _______________________________________________________________ PLEASE ATTACH COPIES OF THE FOLLOWING IF AVAILABLE: MRI, CT Scan Report EEG Report Previous Intellectual/Learning/Neuropsychological Assessment Psychiatric Consultation Report DATE REFERRAL RECEIVED (dd/mm/yr): _______________REFERRAL NAME (PLEASE PRINT) _______________________________ Criteria for patients to be seen by the Neuropsychology Service at Royal Columbian Hospital: (1) patients who live within the Fraser Health Authority catchment area; (2) patients who are 18 years and older, and; (3) patients associated with a mental health team. Exclusion criteria include: (1) patients involved in litigation; (2) patients injured at the workplace, and; (3) patients who only need intelligence testing done.