Document

Cosmetic Dermatology
Digital Lecture Series : Chapter 26
Dr. Shehnaz Arsiwala
MD, DDV
Consultant Dermatologist Prince Aly Khan Hospital,
Saifee Hospital, Mumbai India
Email Id : drshenaz@gmail.com
Introduction
Cosmetics
Topical therapies
• Moisturizers
• Sunscreens
• Antiaging cosmeceuticals
• Cosmetic camouflage
• Adverse reactions
CONTENTS
Procedures
• Chemical Peels
• Microdermabrasion
• Fillers
• Botulinum toxin
• Platelet rich plasma
• Lasers
MCQs
Photo Quiz
Introduction
Cosmetic dermatology is a rapidly developing field of medicine.
Various therapies and procedures are used to enhance one’s aesthetic looks and appearance.
Common cosmetic problems include acne, pigmentation, agerelated, hair and nail problems.
Various topical therapies and interventional procedures are used to address these cosmetic problems.
Cosmetics and Cosmeceuticals
Cosmetic : Any article intended to be rubbed, poured, sprinkled, or sprayed on, introduced into, or otherwise applied to the human body for cleansing, beautifying, or altering the appearance.
Commonly used cosmetics : Soaps, shampoos, moisturizers, antiaging products, eye and lip cosmetics, bleaching and hair products.
Cosmeceutical agents : Pharmacological agents which have an effect intermediate between cosmetics and drugs.
Cosmeceutical botanicals, retinoids, skin lightening agents, sunscreens.
Adverse reactions to cosmetics and cosmeceuticals can occur.
Moisturizers
Moisturizers are agents which hydrate the stratum corneum by either providing water or helping to draw water from the deeper layers of the skin.
Oil-in water or water in oil preparations.
Sunscreens, anti-ageing products like retinols, alpha or beta hydroxy acids and skin-lightening agents may be added to moisturizers.
Moisturizers - types
Oil-in-water :
More cosmetically acceptable by patients
Not very effective for very dry skin conditions
Cream or lotion formulations
Water-in-oil :
Create an occlusive film on the skin surface; reduce water loss and traps moisture in the skin
Stickier, less cosmetically acceptable
More effective for dry skin and ichthyotic conditions
Moisturizers – cosmeceutical agents
Contents of moisturizers :
Stearic, linoleic, linolenic, oleic, and lauric acid, fish oil, petrolatum, shea butter, and sunflower seed oil Petroleum jelly, lanolin, mineral oil, and silicones.
Glycerol, pyrrolidine carboxylic acid , Urea, lactic acid, glycolic acid.
Sesame oil, wheat germ oil and Vit E.
Bisabolol, squalane.
Sun and Ultraviolet index
Ultraviolet index :
Informs about amount of harmful effects of UVL on earth on a particular day.
0-2 - minimal-sunburn occurs over an hour
3-4 - low-sunburn in 30-60 mins
5-6 - moderate-sunburn in 20-30 mins
7-9 - high-sunburn in 10-20 mins
10-15 - v high-sunburn in<10 mins
Sunscreens
Organic agents that block the penetration of UV agents by acting as filters and by absorbing and reflecting UVL.
Sunscreens protect from UVA and UVB rays and reflects, absorbs or scatters harmful rays.
Sun protection factor (SPF) : ability of a sunscreen to delay suninduced skin erythema.
Most sunscreens have a SPF label.
Types of sunscreens
Physical : Form an opaque layer which totally blocks out the sunrays e.g zinc oxide, titanium dioxide and calamine.
Chemical : Absorb the rays and convert the energy to heat which is diffused. These may selectively protect against UVA or UVB.
UVA blockers : Benzophenones, dibenzoylmethanes, Mexoryl.
UVB blockers : P-aminobenzoic acid (PABA) derivatives, salicylates, cinnamates.
FDA Protocol
For effectiveness sunscreen should be layer of 0.5mm thickness.
Reapplication every 20-90 mins depending on activity and lifestyle.
AAD recommendation is sunscreen with atleast SPF 15 to be worn round the year.
Water resistant means sunscreen mantained after 2-20 mins immersions in water.
Very water resistant means lasts upto 4-20 mins immersions in water.
Ultraviolet protection factor
Is the sun protection achieved by wearing fabrics.
Tighter weaves, darker colors, synthetic and loose fit- greatest protection.
Loose woven, light color, tight fit, natural fibres- least protection
Wet clothes offer increased SPF.
UPF recommendation is >30.
Method of sunscreen use
Select a sunscreen SPF 15-30 with UVA and UVB protection.
Apply 15-30 mins before exposure.
Reapply generously after swimming or sweating.
Select water resistant one for beach/outdoor activity associated with perspiration.
To avoid eye stinging, avoid sport gel formula and avoid benzophenones.
To maximize eye protection appropriate sunglasses, polarizing lenses.
Lipsticks sunscreens-useful.
Antiaging cosmeceuticals
Cosmetics formulations with pharmaceutical actions.
Cosmetics with drug like advantages and have ingredients that influence biologic function of skin.
Products are formulated with ingredients of pharmaceutical strength.
Topical antioxidants, cosmeceutical botanicals and retinoids are important ingredients.
Topical retinoids
Tretinoin, adapalene, tazarotene, isotretinoin.
Retinaldehyde and retinol esters.
Used in :
Acne
Photoaging
Pigmentation
Adverse effects :
Retinoid dermatitis : redness, burning, dryness
Post inflammatory pigmentation
Acne flare up
Classification of Antioxidants
Fat Soluble Antioxidants
Vitamin E
Carotenoids
CoQ10/Idebenone
Lycopene
Water Soluble Antioxidants
Glutathione
Vit C
Green Tea- Polyphenols
Silymarin
Coffeberry Extract
Polypodium Leucotomos
Resveratrol
Grape Seed Extract
Pomegranates
Fat And Water Soluble Antioxidants
Alpha Lipoic Acid
Miscellaneous
Genistein
Pycnogenol
Dehydroepiandrosterone
Selenium
Carotenoids
Vitamin A derivatives
Exfoliation, keratin regulation, epidermopoesis, collagen remodelling and angiogenesis , anti-acne actions.
Improves photodamage, pigmentation, texture, fine lines and wrinkles.
Retinoid dermatitis, sun sensitivity and irritation are common problems.
Short contact, night use and low strength is recommended while starting.
Oral carotenoids are used for photoprotection and anticancer actions.
Topical Vitamin E and Vitamin C
Vitamin E
Photoprotection, reduces photoaging.
Improves skin roughness and reduces wrinkling.
Anti-inflammatory and immunostimulatory.
Wound healing, emollient properties.
Vitamin C
Water-or lipid-soluble forms.
Photoprotective and anti-inflammatory.
Reduces photoaging and wrinkles.
For effective topical application, vitamin C must be non-esterified, acidic and optimally at 20% concentration.
Green tea-polyphenols
Green tea belongs to polyphenolic catechin group.
Green tea is one of the most studied antioxidants.
GTPs include extracts such as epicatechin, epigallocatechin, epicatechin-3-gallate, and epigallocatechin 3-gallate (EGCG); the anticarcinogenic effects of green tea are attributed to these extracts and particularly to EGCG.
EGCG is the main and most potent antioxidant compound in green and white tea.
The polyphenols in green tea are excellent antioxidants, antiinflammatory and anticarcinogenic agents. They prevent UV-induced oxidative damage and induction of matrix metalloproteinases.
Idebenone
A synthetic analogue of coq10.
Reduces the photodamage and also reduces fine wrinkles, roughness and dryness in the aged skin.
Contact dermatitis is the most popular side effect noted.
Alpha lipoic acid (ALA)
Fat and water soluble Antioxidants.
Organosulfur compound obtained from octanoic acid.
It is an important network antioxidant and an essential cofactor in mitochondrial dehydrogenases.
Antioxidant effects are due to bioactive form of LA which is strong anti inflammatory agent.
Useful for preventing UVB induced erythema, photodamage and cancer.
Supplement used primarily as a "weight loss" and "energy" supplement.
Cutaneous benefits of ALA Include accelerated chronic wound healing.
Antioxidants : Clinical perspectives
The clinical use of antioxidants is increasing. The use for these cosmeceuticals is either as single agent or in combinations
Correction - fine lines, pigmentation, texture.
Prevention - Maintenance of correction obtained and true prevention.
Added in formulations for photoprotection.
Antiinflammatory, lightening , immunoprotection and anticancer actions antimicrobial, and wound healing properties.
Orally or topically used.
Fine lines, texture and photodamage improvement after 12 weeks of antioxidant cosmeceuticals
Cosmetic camouflage
Concealing of unsightly marks on the skin with specially matched opaque creams and powders.
Contents :
Calamine, zinc oxide, bentonite
Colour pigments
Setting powder
Indications :
Vitiligo
Freckles
Melasma, post inflammatory pigmentation
Hemangiomas, Nevi
Scars
Adverse reactions to cosmetics and cosmeceuticals
Soaps : Repeated use may strip the skin of its protective lipid layer.
Shampoos : Daily washing with harsh shampoos can dry the shaft and make it brittle.
Fragrances : May cause photocontact dermatitis.
Hair colors : Frequent hair lightening or coloring can cause irreversible damage to the hair shaft. Cosmetic alopecia may follow.
Adverse reactions to cosmetics and cosmeceuticals
Moisturizers : Comedogenic ingredients like isopropyl myristate irritate the pilosebaceous follicles.
Sunscreens : Vehicle may exacerbate or induce acne; contact folliculitis may occur.
Skin lightening agents : Excessive and prolonged use may cause exogenous ochronosis.
Interventional procedures
Chemical Peels
Microdermabrasion
Microneedling
Injectables - botulinum, fillers, PRP
Lasers and other technologies
Chemical Peels
Mechanism
Epidermal and part of dermal tissue replacement by –
• Destruction
• Elimination
• Regeneration and remodelling
Controlled stage of inflammation
Classification of Peeling : Depth of Injury
Superficial Wounding (Light peel)
Stratum granulosum, papillary dermis
Medium Depth Wounding
(Medium peel) Upper reticular dermis
Deep Depth Wounding (Deep peel) Mid reticular dermis
Depth of peels
Depth of peel is dependent upon
Chemical applied
Concentration of chemical
Skin type
Preparation of skin
Technique of application
Superficial and mild medium depth peels most popular, moderate medium depth and deep peels are now replaced by laser resurfacing techniques.
Peel Chemicals
Alpha hydroxy acids (AHAs) : Glycolic, lactic, mandelic, pyruvic
Beta hydroxy acids : Salicylic acid
Trichlorocetic acid, phenol
Combinations - AHA cocktails - phytic peel
Newer peels - retinol, arginine peel, azelaic acid peel, acetic acid, phytic, etc.
Indications
Pigmentary conditions - Melasma, photodamage, post inflammatory hyperpigmentation, freckles, lentigenes.
Early Acne scars with residual active acne, Truncal acne.
Acne scars without active acne; with/without pigmentary changes.
Improving fine lines - early wrinkles.
Improving texture and glow.
Contraindications
Unrealistic expectations
Keloid tendency
Active severe acne
Active herpes simplex or bacterial infections.
Isotretinoin recipient in last 6 months.
Unstable vitilligo and psoriasis.
Associated photo aggravated skin diseases.
Salicylic peels during pregnancy, lactation and those sensitivity to aspirin.
Phenol peels in cardiac patients.
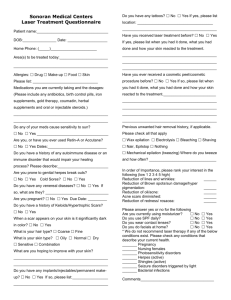
Chemical peels for acne scars
Pre-treatment After 35% glycolic acid peels, 4 sessions
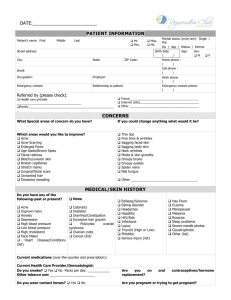
Glycolic acid peels along with topical treatments in Melasma
Common
Erythema
Hyperpigmentation
Irritation
Dryness
Bacterial Infections
Reactivation Of Herpes
Acneiform Eruptions
Complications
Less common
Persistent Erythema
Hypopigmentation
Contact Dermatitis
Milia
Photosensitivity
Hypertrophy/Keloids
Microdermabrasion
Causes resurfacing by mechanical micro-abrasion of skin and is a non- invasive office procedure.
Aluminium crystals or abraded diamond tips can be used works on vaccuum suction principle.
Indications :
Improves mild acne scars
Improves skin texture, fine lines
Minimizes superficial pigmentation
Improves fine lines
Striae
Can improve open pore appearance
Microneedling
Non invasive procedure with an instrument dermaroller.
Creates micro injuries to the epidermis resulting in skin regeneration and collagen induction.
The micro needled tissue repairs by collagen stimulation and hence it is also called as collagen induction therapy .
Indications :
Acne scars, post surgical or traumatic scars
Wrinkle correction
Trans-epidermal drug delivery
Stretch marks
Microneedling
The procedure involves a series of sessions performed after applying an anesthetic cream.
The dermaroller is rolled into the skin over a few minutes. The post treatment skin appears slightly red and has minimal downtime as patient can get back to work on same day.
Absolute sun protection before the procedure and in the interim phase is recommended.
The results are visible depending on the type of problem that is to be corrected textural improvement is seen after first sitting and scar improvement is visible after a series of sessions.
Microneedling
Pre Treatment Post Treatment
Fillers
Botulinum toxin
Platelet rich plasma therapy
Injectables
Various therapeutic modalities in cosmetic dermatology, especially the injectables, laser and technology based devices are used to improve the appearance of ageing in the skin which may be due to chronological or extrinsic effects.
Intrinsic or Chronological
• Genetic makeup
Extrinsic factors
• Solar effects
• Smoking, Alcohol
• Malnutrition
• Gravitational effect
• Sleep lines
• Muscular action
Ageing
Mechanisms of skin ageing
With chronological ageing, skin begins to lose firmness and lift causes the skin to look older.
At molecular level, the connective tissue in the skin becomes weaker, the body produces less collagen and elastin, the key components of healthy, youthful looking skin. In women the breakdown of collagen and elastin is enhanced by exposure to external factors.
Sagging in the aging face occurs due to gravity and changes in the fat compartments.
The loss of fat pads in the upper and mid face and around the mouth, tightening of the central ligaments and loosening of the lateral ligaments- results in the “arc of aging” of the older faces.
Age related skin changes
Epidermis
Thinner, Flattening of DE junction
Slow multiplication of cells and delayed healing time
Dermis
Loss of dermal thickness
Disorganized collagen bundles, abnormal elastin
Changes in glycosaminoglycans – less water holding power
Changes in appearance
Dryness, Skin peeling
Roughness, Pallor
Loss of protective power, delay in recovery from surface damage
Delaying skin ageing - Tips
Avoid Sun Exposure - Exposure to UV light will increase the potential for fine line and wrinkle formation.
Stop Smoking - Smoking depletes the skin of critical moisture and predisposes you to wrinkle formation.
Get Plenty of Rest - Sleep provides a way for your body to relax and rejuvenate.
Maintain hydration of skin.
Use a Humidifier - Humidifiers provide moisture to the air preventing the skin from dehydrating.
Night use of retinol or hyaluronic acid or oligopeptide creams.
Antioxidants will also help to protect the skin throughout the day when applied in the morning.'
Fillers
Using dermal fillers is a treatment of wrinkles, folds or loss of facial volume through a minimally invasive technique.
Fillers are most popular and easy to perform.
Best option for deep folds and grooves in antiaging concepts so far.
Important to choose a right technique for different face areas.
Always fills 90 - 100% of deep wrinkles.
Dermal fillers
Types of fillers :
Temporary : gets absorbed in 3 to 6 months
Semi-permanent : absorbed within 2 years
Permanent : lasts longer than 2 years
Sources :
Heterograft/Xenograft : Bovine collagen, porcine collagen, hyaluronic acid
Allografts : Human-derived collagen
Autografts : Autologous fat, collagen,fibroblasts
Synthetic : Silicone, polytetrafluoroethylene
Classification of Dermal Fillers
Replacement Fillers :
Restore soft tissue volume lost in deep dermis or subcutaneous space.
Collagen.
Hyaluronic acids (HAs).
Stimulatory Fillers :
Restore volume by stimulating fibroblast activity, collagen synthesis and soft tissue growth.
Poly-L-lactic acid (PLLA).
Polymethylmethacrylate (PMMA) - Permanent.
Calcium hydroxylapatite (CaHA).
Target zones that are commonly treated
Nasolabial folds – smile lines
Lip rhytides – upper lip lines
Marionette lines – lines around mouth
Volume enhancement – sunken cheeks
Lip filling and contouring
Chin and cheek augmentation
Tear trough treatment – under eye
Back of hands
Neck and chest
How are they placed under the skin : Injection techniques
Hyaluronic acid
Commonly used filler.
Naturally occurring linear polysaccharide found in extra cellular matrix of connective tissue and serves as a ground substance.
Exhibits no species or tissue specificity.
It is cross-linked for stability in tissues.
Are superior to collagen fillers with minimal allergy and immunogenicity reports.
Fillers : Nasolabial fold correction
After linear threading nasolabial folds
Botulinum toxin (BTX)
BTX is natural, purified protein relaxes wrinkle-causing muscles creates a rejuvenated and more youthful appearance.
Produced by the bacterium clostridium botulinum (Serotype A).
Inhibits release of acetylcholine at the neuromuscular junction causing temporary flaccid paralysis of muscle.
Resultant effects of BTX
• BTX effect takes 2-3 days, full effect seen 7-15 days post treatment.
• The effect lasts
• 4-6 months or longer, patient dependent.
• May last longer with repeated treatments.
• Result will wear off progressively (not sudden).
Recommendations for Reconstitution and Handling
Diluent
Concentration
Storage
Before reconstitution
After reconstitution
Handling
0.9% non-preserved sterile saline ratio of 100 U/ 2.5cc
2C to 8C for up to 24 mo
Up to 6 wks at 4C
Special precautions not required
Cosmetic indications of BTX
Frown lines BETWEEN THE EYEBROWS
Crow’s feet on outer part of eyes.
Forehead lines horizontal lines on forehead seen when eyebrows are raised.
Bunny lines or nasal scrunch are seen at sides of nose while scrunching the nose.
Marionette lines Where the muscles pulling the corners of the mouth down are stronger than those pulling it up.
Popply chin this results from the contraction of the mentalis muscle.
Platysmal bands are vertical neck bands that appear with age.
Facial sculpting Square to lean jaw is to relax the hypertrophic masseters muscles which give most of the asian patients a square jaw look.
Global correction upper half of face
Platelet rich plasma therapy (PRP)
A tool of the modern era of regenerative processes.
Preparation of an autologous platelet concentrate suspended in plasma, also known as platelet-rich plasma, contains growth factors and it is administered to wound sites for wound healing, tissue repair.
Growth factors released from activated platelets initiate and modulate wound healing in both soft and hard tissues.
Indications
Hair growth
Antiaging
Rejuvenation
Scar healing
Technique
The injections are performed using very small needles after numbing the skin with a surface anesthetic cream over one hour.
A recovery period involving transient swelling; and in some cases, bruising which is mild and transient.
PRP evokes an inflammatory response which is desired.
The results are normally seen within 2-3 months and may require 3 to 5 separate sessions.
In general, usually over a 3 to 4 week interval, patients should be able to see improvements in: skin texture; complexion; and tone.
These improvements can continue for up to a year.
L - Light
A - Amplification by
S - Stimulated
E - Emission of
R - Radiation.
LASER
Principle : Chromophore
Action of lasers is through the chromophores.
Chromophores absorb energy and are destroyed.
Oxyhemoglobin, hemoglobin, melanin and water are the main skin chromophores.
Lasers may lead to damage of the collateral structures -
PHOTOTHERMOLYSIS.
Principle : Selective photothermolysis
Only wavelengths of light absorbed by the target tissue than the surrounding tissue are selected.
Light is delivered in pulses to prevent diffusion and thermal damage to surrounding tissue.
Energy is delivered to target in less time than required for heat diffusion to surrounding tissue.
Thermal Relaxation Time
Time taken by the chromophore to loose 63% of its heat after being heated up.
Different chromophores have different thermal relaxation times depending upon their size.
TRT predicts the PULSE WIDTH to be used for a particular chromophore.
Target
Tatoo ink particle
Melanosome
Erythrocyte
Epidermis
Blood vessel
Ectatic bold vessel
Hair Follicle
1
1
7
50
50
100
200
Size
10 ns
1 us
20 us
1 ms
1 ms
15 ms
20-100 ms
TRT
Wavelength
KTP
Excimer x-rays cosmic rays
UV
400 nm
VISIBLE
700 nm
Holmium
Nd:YAG
Er:YAG
INFRARED
Microwaves
TV and radio waves
Lasers
Lasers for hair reduction
Pigmentary lasers
Resurfacing lasers
Vascular lasers
Other technology based devices include use of radiofrequency and high frequency ultrasound- used in skin tightening and body contouring.
Lasers for Hair Removal
Long pulse Ruby laser
Long pulse Alexandrite laser
Long pulse Diode laser
Long pulse Nd : YAG laser
Intense pulsed light
694 nm.
755 nm.
800 nm.
1064 nm.
400 – 1200 nm.
Pre Treatment Post Treatment
Diode- 28J/cm2,
100ms. 3sessions
Lasers for Pigmented Lesions
Q- switched lasers
Frequency doubled Nd : YAG laser 532 nm.
Ruby laser
Alexandrite laser
Nd : YAG laser
694 nm.
755 nm.
1064 nm.
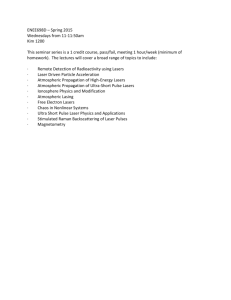
1064 Q Switched ND YAG Laser for Tattoo Removal
Pre treatment Immediate Post treatment
Post treatment
After 2 sessions
Ablative Lasers
Erbium YAG laser
2940 nm.
CO 2 laser
10600 nm.
Indications
Acne scars
Wrinkles
Rhinophyma, xanthelesma
Verrucous epidermal nevi
NON ABLATIVE LASERS and
Radiofrequency
Infrared lasers
• 1320 nm Nd : YAG laser
• 1450 nm Diode laser
• 1540 nm Erbium Glass laser
Broad band light
Intense pulsed light
Non ablative radio frequency
Indications
Wrinkles
Superficial atrophic scars
Laser resurfacing - Grade 2 rolling & superficial boxcar scars
Pre Treatment Post Treatment
Combination Therapy with Q switched ND YAG laser and fractional carbon dioxide laser :
Texture, pigmentation and acne scars improvement
Lasers for Vascular Lesions
Flash pumped pulse dye laser
Long pulse Alexandrite laser
Long pulse FD Nd : YAG laser
Intense pulsed light
Long pulse Nd : yag Laser
585 nm.
755 nm.
532 nm.
515 - 590 nm.
1064 nm.
Excimer Laser
Monochromatic light of wavelength 308 nm
Targeted treatment of :
Vitiligo
Psoriasis
Complications of Laser
Persistent erythema
Vesiculation and crusting
Hyperpigmentation
Hypopigmentation
Scarring
Good expertise → minimal complications
MCQ’s
Q.1) Ultraviolet index
A.
Informs about amount of harmful UVL on earth on a particular day
B.
Informs about SPF factor
C.
Informs about sunburn factor
D.
Informs about UV damage
Q.2) Chemical peels destroy
A.
Epidermis
B.
Dermis
C.
Oil glands
D.
Epidermis and part of dermis
MCQ’s
Q.3) This is not a chromophore for lasers
A.
Water
B.
Gas
C.
Oxyhemoglobin
D.
Melanin
Q.4) Thermal Relaxation Time predicts
A.
The pulse width to be used for a particular chromophore
B.
The fluence used
C.
The spot size
D.
Thermal damage time
MCQ’s
Q.5) Wavelength of diode laser for hair removal is
A.
810nm
B.
1064nm
C.
655nm
D.
786nm
Q.6) Botulinum toxin
A.
Inhibits release of acetylcholine at the neuromuscular junction
B.
destroys nerve axons
C.
causes myelin sheath denervation
D.
causes activation of neuromuscular junction
Photo Quiz
Q. What laser can be used to clear this tattoo?
Photo Quiz
Q. What interventions can be considered for this patient with acne scars, aging skin and melasma?