Clinical Trial Protocol
advertisement

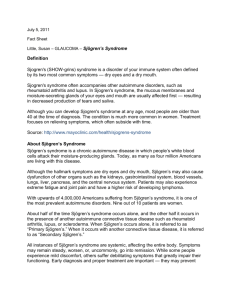
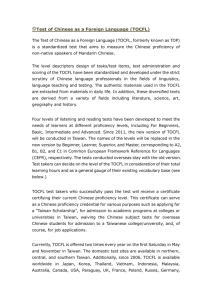
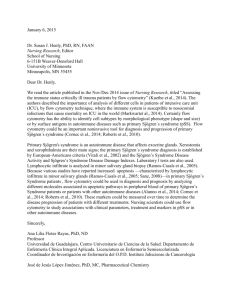
Title: From the Core Pattern Analysis on Chinese Herbal Medicine for Sjögren's Syndrome to A Protocol of Randomized Control Trial: A Nationwide Population-Based Study in Taiwan from Year 2002 to 2011 Running head: Nationwide Survey of CHMs for Sjögren's Syndrome and a SS-1 Clinical Trial Protocol Authors: Ching-Mao Chang 1,2, Hsueh-Ting Chu 3,4,d, Yau-Huei Wei 5,6, Fang-Pey Chen 2, Shengwen Wang 7, Po-Chang Wu 8, Hung-Rong Yen 9,a,d, Tzeng-Ji Chen b,c,*, Hen-Hong Chang 1,9,a,d,* Grants/Financial Support: This study was supported by the National Science and Technology Program for Biotechnology and Pharmaceuticals, Ministry of Science and Technology [MOST 103-2325-B-039-009], Taiwan, and it was also supported by China Medical University under the Aim for Top University Plan of the Ministry of Education, Taiwan, R.O.C. Corresponding author: Prof. Hen-Hong Chang, M.D., Ph.D. School of Chinese Medicine, China Medical University, Taichung 404, Taiwan, R.O.C E-mail: tcmchh55@gmail.com Co-corresponding author: Prof. Tzeng-Ji Chen Department of Family Medicine, Taipei Veterans General Hospital, Taipei 112, Taiwan, R.O.C. Email: tjchen@vghtpe.gov.tw Conflict of interest: The authors declare that they have no competing interests. Word count: 3657 Abstract Objectives. This large-scale survey aimed to evaluate frequencies and patterns of Chinese herbal medicine (CHM) used for Sjögren's syndrome (SS) in Taiwan by analyzing the National Health Insurance Research Database (NHIRD) while CHM has been another alternative therapy of conventional western medication for improving patients’ discomforts. Methods. We analyzed the SS primary diagnosis (ICD-9:710.2) with catastrophic illness certificate (CIC) in Traditional Chinese Medicine (TCM) outpatients’ clinics from three cohorts of Longitudinal Health Insurance Database (LHID) in the NHIRD between years 2002 and 2011. CHM prescription patterns for SS were evaluated from claimed visiting files and corresponding prescription files. Results. There were 15,914 SS patients with CIC (SS/CIC), only 683 SS/CIC in LHID2000, 678 in LHID2005 and 635 in LHID2010 respectively. We found 130 SS/CIC visiting the TCM clinics in LHID2000, 133 in LHID2005 and 126 in LHID2010, and duplicating data were removed. Hence, 366 SS/CIC and 4,867 visits were performed in our study, and the ages between 50 and 59 years had the highest ratio (29.51%) in both female and male. Qi-Ju-Di-Huang-Wan and Xuan-Can (Scrophularia ningpoensis Hemsl.) was the most commonly-used formulae and single herb. Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Mai-Men-Dong (Ophiopogon japonicus (L. f.) Ker-Gawl.) and Sheng-Di-Huang (raw Rehmannia glutinosa Libosch) were the core pattern prescriptions in treating with SS/CIC. Conclusions. Higher CHM utilization rates of SS/CIC were investigated in this large-scale NHIRD in Taiwan from years 2002 to 2011. We also initiated a well-defined, randomized, double-blind, placebo-controlled and crossover clinical trial (Clinicaltrials.gov NCT02110446) to provide evidence-based clinical data in TCM. Keywords: Sjögren's syndrome, Traditional Chinese medicine, National Health Insurance Research Database, Qi-Ju-Di-Huang-Wan, Xuan-Can, SS-1 Significance and Innovations The utilization-patterns of CHMs for Sjögren's syndrome with catastrophic illness certificate were evaluated with a large-scale survey in Taiwan. The CHMs descripting may have some potential effects on antioxidant capacity, anti-inflammation and immune modulation. “Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Mai-Men-Dong and Sheng-Di-Huang (raw Rehmannia glutinosa Libosch) were the core pattern prescriptions in treating with SS from the network analysis. A randomized, double-blind, placebo-controlled clinical trial (Clinicaltrials.gov NCT02110446) was initiated to provide EBM in TCM. Introduction Sjögren's syndrome (SS) is an auto-immune disease which is mainly involved with exocrine gland such as lacrimal and salivary glands, and it also causes gland dysfunction through the manifestation of dry mouth and dry eye (1). SS can be divided into primary and secondary types (2, 3). The former, primary Sjögren's syndrome (pSS), presents SS alone, and the latter, secondary type, combines other autoimmune diseases like rheumatoid arthritis (RA) (4), systemic lupus erythematosus (SLE) (5) or systemic scleroderma (6). In Taiwan, the incidence of pSS from year 2005 to 2007 was 6.0 (per 100,000 inhabitants) with a female/male ratio of 9.9 (7). And the prevalence and incidence of SS was the third autoimmune rheumatic diseases in Taiwan form 2000 to 2008(8). The pathogenesis of pSS is still unclear, but some clues support the thesis of dysfunction of B cells and T cells, which lead to autoimmune epithelial cell inflammation and maybe the mainstream concept of pathogenesis for pSS (9, 10). The type I interferon and B-cell-activating factor were an important issue according to the current point of view (11-13). Because some SS patients treated with conventional western medication had discomforts such as pain (14) and fatigue (15, 16), some SS had a high risk of developing non-Hodgkin's lymphoma (17). Complementary and alternative medicine (CAM) was another choice for improving the symptoms and signs. Chinese herbal medicine (CHM) (18) and acupuncture (19) were common CAM therapies widely accepted by SS patients, and many randomized control trials were performed in treating SS (20). These studies had poor methodological quality of included trials and high heterogeneity and complexity of interventions; no recommendation for specific CHMs could be used in the clinical. National Health Insurance (NHI) covers both western medicine and Traditional Chinese Medicine (TCM) medical care records in Taiwan since 1995 till this day (21). Most of the general populations (98%) in Taiwan were covered in the NHI program at the end of 2012. A recent large-scale investigation about TCM usage for SS in Taiwan showed Qi-Ju-Di-Huang-Wan was the most commonly prescribed Chinese herbal formula for SS (22). However, the report included only one cohort LHID (one million random sample subjects) and the results may be overestimated in patient recruited for TCM visiting and the average daily dose of Chinese formula for the patients to take. Hence we conducted a national population-based study from three cohorts LHID in Taiwan for Chinese herbal medicine (CHM) utilization of SS from year 2002 to 2011 and focused on the SS patients with CIC and SS primary diagnosis in TCM visits. Methods Data Sources The National Health Insurance (NHI) program was a unique database which implemented in Taiwan from 1995 and covered almost entire population. Nationwide medical information was recorded as an electronic claim data in National Health Insurance Research Database (NHIRD) that contains genders, ages, dates of encounters, disease diagnosis of patients, and prescription of all beneficiaries (23). Scrambling cryptogram was performed on these data for protecting patients and institutional privacies. The study population with the diagnosis of diseases was defined according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Since this is a retrospective analysis of the NHIRD and all the individual information data are de-identified, so we cannot get the inform consent form from the including patients. This study was approved by the Institutional Review Board of Taipei Veterans General Hospital (VGHIRB-2013-04-005E). Identification of Patients with Sjögren's Syndrome We designed a national population-based study to analyze three cohorts of one million random sample subjects selected from all the beneficiaries of the NHI program in Taiwan, and we surveyed the CHM usage rate and patterns to determine the utilization of the subjects with primary diagnosis of Sjögren's syndrome treated in TCM outpatients’ clinics. SS Primary diagnosis in TCM visits can reduce the statistical bias due to TCM visits for non-SS treatments. Sjögren's syndrome is one of the 31 categories of major illnesses or injuries that result in a patient holding a catastrophic illness certificate (CIC). Since Sjögren's syndrome and Sicca syndrome had the same ICD-9 code “710.2”, we identified the “true” Sjögren's syndrome from CIC holders between years 2002 and 2011. These populations were matched with three cohorts of one million random samples from the Longitudinal Health Insurance Database (LHID2000, LHID2005 and LHID2010), which LHID extracted 1-million random sampling from 26-million individuals of the NHIRD in the year 2000, 2005 and 2010. The SS subjects were included in this study after duplicating data were removed. Figure 1 is the flowchart of recruitment of subjects from the 3-million random samples for SS with CIC from the NHIRD in Taiwan. Data Analysis Data linkage analysis and processing were set up with the Structure Query Language (SQL server 2008, Microsoft Corp., Redmond, WA USA). Statistical Package for Social Science version 19.0 (SPSS Inc., Chicago, IL USA) was applied to analyze the frequency and patterns of formulae or single herbs and CHM utilization. In addition, we identified core patterns of CHMs used in treating SS/CIC patients through an open-sourced freeware NodeXL (http://nodexl.codeplex.com/), and all the selected combinations were applied for the network analysis (24, 25). The line width ranging from one to ten in the network figure was defined by counts of connections between a certain CHM and co-prescribed CHMs, and thicker widths of line connections indicated crucial prescription patterns. Top 5 core patterns of CHMs were clearly identified within the network analysis of the CHM utilization. Results There were 15,914 Sjögren's syndrome patients with CIC (SS/CIC) in Taiwan from year 2002 to 2011, but there were only 683 SS/CIC with primary diagnosis in LHID2000, 678 in LHID2005 and 635 in LHID2010, respectively. In these three LHID data, more than 90% SS outpatients had visited TCM clinics. However, not all the patients visited TCM clinics for the Sjögren's syndrome, so we only included the SS primary diagnosis in TCM visits. We found 130 SS patients in LHID2000, 133 in LHID2005 and 126 in LHID2010, and we removed the 23 duplicating data. There were 366 SS patients and 4,867 visits in total with the SS primary diagnosis in the TCM clinics from year 2002 to 2011. The flowchart of recruitment of subjects treated with CHM from the 3-million random samples for SS/CIC in the NHIRD in Taiwan was shown in Figure 1. There were 339 female and 27 male patients in 366 SS/CIC patients treated with CHM, and female patients preferred using CHM for SS more than male patients (Female: Male = 12.56: 1). The age-sex-specific frequency of CHM used in SS/CIC patients is illustrated in Table 1, and the age and sex of SS/CIC were performed only with the time of the first visit at TCM clinics. The ages between 50 and 59 years had the highest ratio (29.79% and 25.93%) in female and male groups, and the mean ± SD were 54.82 ± 13.00 in female and 57.96 ± 16.42 in male patients. The mean ± SD of TCM clinic visits among 366 SS/CIC patients was 13.30 ± 20.09, most of SS/CIC patients visited TCM clinic less than 10 times, and the maximum was 129. The mean ± SD of medical service provided from 472 TCM doctors was 10.31 ± 19.15. Most of TCM doctors diagnosed and treated SS patients for less than 10 times, and the maximum was 143. Table 2 was the visit distribution of patients and doctors of Sjögren's syndrome in Taiwan. Table 3 presents the top 10 formulae for treating SS among the total 26,733 CHM prescriptions. The most commonly-used formula was Qi-Ju-Di-Huang-Wan (9.08%), and the average daily dosage was 4.78 ± 1.62 gram (g). The following ones were Gan-Lu-Yin (8.16%), Jia-Wei-Xiao-Yao-San (6.02%), Zhi-Gan-Cao-Tang (2.06%), Xue-Fu-Zhu-Yu-Decoction (2.03%) with the average daily dosage of 4.37 ± 1.78 g, 4.70 ± 1.49 g, 3.65 ± 2.23 g and 4.50 ± 2.21 g respectively. The top 10 single herbs for SS/CIC are listed in Table 4. Xuan-Can (Scrophularia ningpoensis Hemsl., 2.98%) was the most commonly-used single herb, and the average daily dosage was 1.86 ± 0.41 g, followed by Mai-Men-Dong (Ophiopogon japonicus (L. f.) Ker-Gawl., 2.93%), Sheng-Di-Huang (raw Rehmannia glutinosa Libosch., 21.7%), Tian-Hua-Fen (Trichosanthes kirilowii Maxim., 2.04%), Huang-Qin (Scutellaria baicalensis Georgi, 1.95%) with the average daily dosage of 1.38 ± 0.58 g, 1.42 ± 0.52 g, 1.24 ± 0.46 g and 1.24 ± 0.46 g respectively. Figure 2 shows that a SS/CIC patient was given an average item of 6.24 ± 2.47 CHMs in a single prescription, and five items of CHMs (16.85%) was the most common prescription with the combination of formulae or single herbs. The following ones were 6 CHMs (16.71%) and 7 CHMs (13.77%). Some SS patients, only at a very low ratio (0.05%), were prescribed more than 20 CHMs. Among these prescriptions, we evaluated the co-prescription pattern of formula and single herb. Table 5 shows the most common prescription patterns of two formulae combination and two single herbs combination. The most common item of two formulae combination was “Qi-Ju-Di-Huang-Wan plus Gan-Lu-Yin”, followed by “Jia-Wei-Xiao-Yao-San plus Qi-Ju-Di-Huang-Wan”, “Jia-Wei-Xiao-Yao-San plus Ping-Wei-San”, “Jia-Wei-Xiao-Yao-San plus Zhi-Bo-Di-Huang-Wan” and “Gan-Lu-Yin plus Sang-Ju-Yin.” And the most common items of two single herbs were “Xuan-Can plus Mai-Men-Dong”, “Sheng-Di-Huang plus Mai-Men-Dong”, “Xuan-Can plus Sheng-Di-Huang”, “Gou-Qi plus Mai-Men-Dong” and “Sha-Can (Glehnia littoralis F. Schmidt ex Miq.)plus Mai-Men-Dong.” Table 6 shows the most common prescription patterns of two and triple formulae/single herbs combination. The most common combination of two formulae/single herbs combination was “Qi-Ju-Di-Huang-Wan plus Gan-Lu-Yin”, followed by “Xuan-Can plus Mai-Men-Dong”, “Sheng-Di-Huang plus Mai-Men-Dong”, “Xuan-Can plus Sheng-Di-Huang” and “Xuan-Can and Gan-Lu-Yin.” And the most common combination of triple formulae/single herbs combination was “Xuan-Can, Sheng-Di-Huang plus Mai-Men-Dong”, followed by “Nu-Zhen-Zi (Ligustrum lucidum Ait.), Jia-Wei-Xiao-Yao-San plus Gou-Qi”, “Nu-Zhen-Zi, Wu-Wei-Zi (Schizandra chinensis (Turcz.) Baill.) plus Jia-Wei-Xiao-Yao-San”, “Wu-Wei-Zi, Jia-Wei-Xiao-Yao-San and Gou-Qi” and “Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin plus Dan-Can.” The network analysis in Figure 3 demonstrated that “Qi-Ju-Di-Huang-Wan”, “Gan-Lu-Yin”, “Xuan-Can”, “Mai-Men-Dong” and “Sheng-Di-Huang” formed the core pattern of Chinese formula and other single herbs used to treat the Sjögren's syndrome patients with catastrophic illness certificate. Discussion This study is the first nationwide population-based survey of the utilization and core pattern analysis of CHM with Sjögren's syndrome patients with catastrophic illness certificate from three LHID in Taiwan. Females SS/CIC patients had much higher ratio of using CHM than males (12.56: 1); and the female and male groups aged from 50 to 59 years both had the highest ratio of CHM use for SS/CIC. It may have the correlation with a lack of both active estrogens and androgens, which leads to apoptosis in epithelial salivary gland cells (26). A recent study demonstrated different serum levels of endocrines regarding SS symptoms and discussed that oral dryness may be related to a low level of androgens, while low level of estrogens were expressed with ocular dryness (27). The total numbers of SS/CIC were 15,914 (which 72,391 is the total patient number of generalized autoimmune syndrome requiring lifelong treatment with CIC (28)) in Taiwan from year 2002 to 2011, and the SS/CIC subjects treated with CHM were 366 patients, including from three LHID with the duplicating data are removed. The sample size in this study was not large enough; it could not represent the whole view of SS/CIC with CHM treatment. The database could only represent the ratio of one-million samplings/total 26-million total inhabitants (3.84%). We found that the ratio of SS/CIC patients treated with CHM could be traced back to consider as 63.55% of the entire SS/CIC, the ratio could also match the nationwide survey of TCM utilization (29). There were 366 subjects with TCM clinic visits among 472 TCM doctors; four subjects had visited over 100 times from year 2002 to 2011 while the 238 subjects (65.03%) had visited less than 10 times. The situation also occurred in the TCM doctor side; only three doctors had visited more over 100 times while 343 doctors (72.67%) had visited less than 10 times. The phenomenon of doctor shopping among patients with chronic illness may account for the observation that many SS/CIC patients received treatment with CHM from different TCM doctors (30). The common reasons for doctor shopping is that the health service of family doctors system in Taiwan had not yet been well-established (31); therefore, patients who have been bothered by persistent symptoms and medication side effects seek a second opinion (32). The health care cost may be also wasted due to this doctor shopping in TCM (33). “Qi-Ju-Di-Huang-Wan” was the most commonly-used formula for SS/CIC; its therapeutic function was “nourish the liver and brighten the eyes”, and it could be used for SS and dry eye. Recent literatures reported that “Qi-Ju-Di-Huang-Wan” had more effective effect than conventional medicine on SS, no matter whether using “Qi-Ju-Di-Huang-Wan” alone (34) or “Qi-Ju-Di-Huang-Wan” plus acupuncture (35). Chang (36) used “Qi-Ju-Di-Huang-Wan” with a randomized, double-masked, parallel grouped and controlled study to treat dry eyes, and the result showed that abnormalities of corneal epithelium reduction and it also could be an alternative drug for topical eye drops. However, the included subjects in Chang’s study were dry eye syndrome not SS, “Qi-Ju-Di-Huang-Wan” may have the potential therapeutic effect for the dry eye symptom of SS. “Gan-Lu-Yin” was the second commonly-used formulae in our database; its therapeutic function was “enrich yin and clear heat”, and it could be used for the treatment of SS and dry month. A study used “Gan-Lu-Yin” in post-radiotherapy NPC patients to alleviate the mucositis and dry mouth (37). “Jia-Wei-Xiao-Yao-San” can “course the liver and resolve depression”, and Yi et al. (38) used it to treat xerophthalmia in perimenopausal women with significant improvement of visual fatigue sensation, red eye, dryness, foreign body sensation, burning sensation and photophobia. “Zhi-Gan-Cao-Tang” features “boost qi and enrich yin”; however, no literature discusses it for treating SS related symptoms. “Xue-Fu-Zhu-Yu-Decoction” can “quicken the blood and dispel stasis”, it can modulate the immune function of B cells and T cells (39) and alleviate tissue fibrosis (40). “Xuan-Can” was the most commonly-used single herb with the function of “enrich yin and clear heat”, and it had some positive effects on anti-inflammation and tumor cell apoptosis (41). “Mai-Men-Dong” was the second commonly-used single herb to “nourish yin and moisten dryness”, it can down-regulate the mRNA expression of TGF-β1 and had potential antioxidant activity (42). “Sheng-Di-Huang” can “enrich yin and clear heat”, it also reduced eosinophil cationic proteins level which was positively correlated with "heat zheng" (43). “Tian-Hua-Fen” can “clear heat and engender liquid”, and it can inhibit Nitrogen oxide activity and elevate anti-inflammation effects (44). “Huang-Qin” can “clear heat and drain fire” and it has the function of scavenging reactive oxygen species.(45) Figure 3 includes the top 50 Chinese formula and single herbs for the Sjögren's syndrome patients with catastrophic illness certificate and shows the core pattern of these CHMs. This figure implies that Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Mai-Men-Dong and Sheng-Di-Huang are among the most frequently used combinations. Although these items may have some potential effects on antioxidant capacity, anti-inflammation and immune modulation, they were rarely applied in clinical trials. Furthermore, these five CHMs of the core pattern identified in the figure did not have the function of alleviating tissue fibrosis. For this purpose, we initiated a randomized, double-blind, placebo-controlled, cross-over design clinical trial (Clinicaltrials.gov NCT02110446) for the SS/CIC patients in order to evaluate the effect of CHM (SS-1) on the regulation of oxidative stress-related cytokines and the antioxidant capacity. “Gan-Lu-Yin, Sang-Ju-Yin and Xue-Fu-Zhu-Yu-Decoction” with the ratio of 2:1:1 is the composition of SS-1, and its therapeutic functions include antioxidant capacity, anti-inflammation, immune modulation and anti-fibrosis. We expect the quality of patients’ life and clinical manifestation will be improved by reducing the oxidative stress. And we also plan to use a SS cell model to elucidate the antioxidant effect and the mechanism of action of SS-1. Our analysis shows different results from a recent SS report surveying the CHM prescription patterns in Taiwan from 1997 to 2008 (22): (1) We included the SS/CIC subjects from three LHID between year 2002 to 2011 for a comprehensive and up-to-date nationwide survey. (2) We only included the primary diagnosis with SS/CIC in TCM visits, so as to reduce the statistical bias due to TCM visits for non-SS treatments. (3) The statistics of SS/CIC patient number and the dosage of top 10 Chinese formulae demonstrated more rational and significant results in this study. However, there are some limitations in this study: (1) Many potential SS patients accepted the conventional therapy or TCM, but they were not CIC holders due to incompatibility of histopathology or autoantibody criteria. Since the SS subjects included in this study are required to have the CIC, the CHM utilization of SS patients may be underestimated. (2) The sample size in this study was not large enough; hence, we should conduct another larger survey on this issue in the future. (3) Since the subjects included in this study were extracted from three LHIDs, the multivariate logistic regression model was not conducted to evaluate the correlated factors in the CHM utilization. (4) We studied the utilization of CHM only in the recruited SS/CIC patients; however, we did not investigate the utilization of acupuncture, Chinese tuina or other CAMs which they might be applied in SS therapies as well. Clinical Trial Protocol A Protocol of Chinese Herbal Medicine SS-1 Randomized Control Trial for Sjögren's Syndrome We initiated a randomized, double-blind, placebo-controlled, cross-over design clinical trial (Clinicaltrials.gov NCT02110446) to evaluate the effect of Chinese herbal medicine (SS-1) on the regulation of oxidative-related cytokines and the antioxidant capacity for the SS/CIC patients from April 2014 and recruited the subjects from July 2014. Through the oxidative stress reduction, the quality of patients’ life and clinical manifestation will be improved. And we will also use a SS cell model to elucidate the antioxidant mechanism of SS-1. This study was approved by the Institutional Review Board and ethics committee of Chang Gung Memorial Hospital in Taiwan (103-4180C). All the participants who were included in this study provided their written informed consent to participate. Ninety of SS patients in this clinical trial will be screened and be referred from the out-patient department (OPD) of the Rheumatology Department of Chang Gung Memorial Hospital. The 60 of the included patients will be randomly divided into two groups (A and B) and all of them will keep receiving the routine treatment in the rheumatology OPD. Group A patients will first receive a 12-week SS-1 treatment and then stop the SS-1 for 4 weeks in order to enter the wash-out phase; at last, they will receive a 12-week placebo treatment. Group B patients will receive a 12-week placebo first and then stop the placebo treatment for 4 weeks in order to enter the wash-out phase; afterwards, they will receive a 12-week SS-1 treatment. SS-1 is composed of the powder of “Gan-Lu-Yin, Sang-Ju-Yin and Xue-Fu-Zhu-Yu-Decoction” in the ratio of 2:1:1; while the placebo is composed of corn starch, pigment and 1/100 SS-1. Patients in both groups will take 6 grams of experimental medicine three times per day. We plan to evaluate the associated parameters at the time just before treatment (V1), after the first treatment (V2), at the end of wash-out phase (V3) and when the crossover treatment is completed (V4). Primary Outcome Measure: Clinical manifestation and quality of life SS-1 may improve the clinical manifestation (EULAR Sjogren's Syndrome Patient Reported Index, Ocular Surface Disease Index, SS symptoms Questionnaire, Schirmer's test, salivary scintigraphy) and the quality of life (SF-36) for the patients with Sjögren's syndrome. Secondary Outcome Measures: Oxidative stress, antioxidant capacity and regulatory effect on cytokine SS-1 may reduce the oxidative stress (8-OHdG) and elevate the antioxidant capacity (TAC, GSH, SOD, GPX, CAT). Moreover, SS-1 may have the regulatory effect on related cytokine secretion of immune function. Other Pre-specified Outcome Measures: Patient safety, adverse effect and tongue diagnosis We will monitor the patient safety and adverse effect (ADR) during the SS-1 trial, and monitor Liver, Kidney and Blood function (RBC, WBC, Hb, PLT, AST, ALT, BUN, Cre) during the SS-1 trial. Besides, SS-1 may have effect on the tongue diagnosis before and after the treatment. Statistical methods for efficacy/safety evaluations We will analyze the study population with an intent-to-treat model, and a generalized estimating equation will be used to evaluate the difference of the primary, secondary outcomes, drug safety monitor and tongue diagnosis between two groups. The statistical difference was considered to be significant at p value < 0.05 and both with a 95% confidence interval. Conclusions Qi-Ju-Di-Huang-Wan was the most commonly-used formula while Xuan-Can was the most commonly-used single herb in our database. Among different age groups, the highest utilization of CHM was found between ages 50 and 59 in both female and male. The most commonly-used two formulae combination was “Qi-Ju-Di-Huang-Wan plus Gan-Lu-Yin”, and the most commonly-used two single herbs combination was “Xuan-Can plus Mai-Men-Dong.” The core pattern prescriptions were Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Sheng-Di-Huang and Mai-Men-Dong. However, the therapeutic effects and safety of these commonly-used CHMs treated for Sjögren's syndrome in this study have not been clearly elaborated, so well-designed clinical trials for this purpose are required in the future. Author’s contributions CMC, TJC and HHC were responsible for study concept and design, modification of study design, and review and interpretation of data. CMC, TJC and HHC were also responsible for drafting the manuscript. HTC, SWW and PCW provided modifications of study design and revisited the manuscript. YHW, FPC and HRY contributed to collection, analysis and interpretation of data and revisited the manuscript. All authors read and approved the final manuscript. Conflict of interests The authors declare that they have no competing interests. Acknowledgments This study was a portion of data that were extracted from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Ministry of Health and Welfare in Taiwan. This study was supported by the National Science and Technology Program for Biotechnology and Pharmaceuticals, Ministry of Science and Technology [MOST 103-2325-B-039-009], Taiwan, and it was also supported by China Medical University under the Aim for Top University Plan of the Ministry of Education, Taiwan, R.O.C. References 1. Tincani A, Andreoli L, Cavazzana I, Doria A, Favero M, Fenini MG, et al. Novel aspects of Sjogren's syndrome in 2012. BMC medicine. 2013;11:93. 2. Bowman SJ, Fox RI. Classification criteria for Sjogren's syndrome: nothing ever stands still! Ann Rheum Dis. 2014;73(1):1-2. 3. Goules AV, Tzioufas AG, Moutsopoulos HM. Classification criteria of Sjogren's syndrome. Journal of autoimmunity. 2014;48-49:42-5. 4. He J, Ding Y, Feng M, Guo J, Sun X, Zhao J, et al. Characteristics of Sjogren's syndrome in rheumatoid arthritis. Rheumatology (Oxford). 2013;52(6):1084-9. 5. Hernandez-Molina G, Zamora-Legoff T, Romero-Diaz J, Nunez-Alvarez CA, Cardenas-Velazquez F, Hernandez-Hernandez C, et al. Predicting Sjogren's syndrome in patients with recent-onset SLE. Rheumatology (Oxford). 2013;52(8):1438-42. 6. Kobak S, Oksel F, Aksu K, Kabasakal Y. The frequency of sicca symptoms and Sjogren's syndrome in patients with systemic sclerosis. International journal of rheumatic diseases. 2013;16(1):88-92. 7. Weng MY, Huang YT, Liu MF, Lu TH. Incidence and mortality of treated primary Sjogren's syndrome in Taiwan: a population-based study. The Journal of rheumatology. 2011;38(4):706-8. 8. Yu KH, See LC, Kuo CF, Chou IJ, Chou MJ. Prevalence and incidence in patients with autoimmune rheumatic diseases: a nationwide population-based study in Taiwan. Arthritis care & research. 2013;65(2):244-50. 9. Voulgarelis M, Tzioufas AG. Pathogenetic mechanisms in the initiation and perpetuation of Sjogren's syndrome. Nature reviews Rheumatology. 2010;6(9):529-37. 10. Youinou P, Pers JO. Disturbance of cytokine networks in Sjogren's syndrome. Arthritis research & therapy. 2011;13(4):227. 11. Kroese FG, Bootsma H. Biomarkers: New biomarker for Sjogren's syndrome-time to treat patients. Nature reviews Rheumatology. 2013;9(10):570-2. 12. Nocturne G, Mariette X. Advances in understanding the pathogenesis of primary Sjogren's syndrome. Nature reviews Rheumatology. 2013;9(9):544-56. 13. Yoshimoto K, Tanaka M, Kojima M, Setoyama Y, Kameda H, Suzuki K, et al. Regulatory mechanisms for the production of BAFF and IL-6 are impaired in monocytes of patients of primary Sjogren's syndrome. Arthritis research & therapy. 2011;13(5):R170. 14. Segal BM, Pogatchnik B, Henn L, Rudser K, Sivils KM. Pain severity and neuropathic pain symptoms in primary Sjogren's syndrome: a comparison study of seropositive and seronegative Sjogren's syndrome patients. Arthritis care & research. 2013;65(8):1291-8. 15. Haldorsen K, Bjelland I, Bolstad AI, Jonsson R, Brun JG. A five-year prospective study of fatigue in primary Sjogren's syndrome. Arthritis research & therapy. 2011;13(5):R167. 16. Segal B, Thomas W, Rogers T, Leon JM, Hughes P, Patel D, et al. Prevalence, severity, and predictors of fatigue in subjects with primary Sjogren's syndrome. Arthritis and rheumatism. 2008;59(12):1780-7. 17. Johnsen SJ, Brun JG, Goransson LG, Smastuen MC, Johannesen TB, Haldorsen K, et al. Risk of non-Hodgkin's lymphoma in primary Sjogren's syndrome: a population-based study. Arthritis care & research. 2013;65(5):816-21. 18. Wu GL, Li TY, Fan YS, Yu GY. Therapeutic effect of Chinese herbal medicine for strengthening qi, nourishing yin, and removing stasis on serum osteopontin and quality of life of patients with primary Sjogren's syndrome. Chinese journal of integrative medicine. 2011;17(9):710-4. 19. List T, Lundeberg T, Lundstrom I, Lindstrom F, Ravald N. The effect of acupuncture in the treatment of patients with primary Sjogren's syndrome. A controlled study. Acta odontologica Scandinavica. 1998;56(2):95-9. 20. Luo H, Li X, Liu J, Andrew F, George L. Chinese Herbal Medicine in Treating Primary Sjogren's Syndrome: A Systematic Review of Randomized Trials. Evidence-based complementary and alternative medicine : eCAM. 2012;2012:640658. 21. Lee YC, Huang YT, Tsai YW, Huang SM, Kuo KN, McKee M, et al. The impact of universal National Health Insurance on population health: the experience of Taiwan. BMC health services research. 2010;10:225. 22. Yu MC, Lin SK, Lai JN, Wei JC, Cheng CY. The traditional Chinese medicine prescription patterns of Sjogrens patients in Taiwan: A population-based study. Journal of Ethnopharmacology. 2014. 23. Cheng SH, Chiang TL. The effect of universal health insurance on health care utilization in Taiwan. Results from a natural experiment. The Journal of the American Medical Association. 1997;278(2):89-93. 24. Chen HY, Lin YH, Su IH, Chen YC, Yang SH, Chen JL. Investigation on Chinese herbal medicine for primary dysmenorrhea: implication from a nationwide prescription database in Taiwan. Complement Ther Med. 2014;22(1):116-25. 25. Yang DH, Kang JH, Park YB, Park YJ, Oh HS, Kim SB. Association rule mining and network analysis in oriental medicine. PloS one. 2013;8(3):e59241. 26. Mavragani CP, Fragoulis GE, Moutsopoulos HM. Endocrine alterations in primary Sjogren's syndrome: an overview. Journal of autoimmunity. 2012;39(4):354-8. 27. Forsblad-d'Elia H, Carlsten H, Labrie F, Konttinen YT, Ohlsson C. Low serum levels of sex steroids are associated with disease characteristics in primary Sjogren's syndrome; supplementation with dehydroepiandrosterone restores the concentrations. The Journal of clinical endocrinology and metabolism. 2009;94(6):2044-51. 28. Administration NHI. Medical Utilization of Major Illness/Injury. Taipei: National Health Insurance Administration, 2012. 29. Chen FP, Chen TJ, Kung YY, Chen YC, Chou LF, Chen FJ, et al. Use frequency of traditional Chinese medicine in Taiwan. BMC health services research. 2007;7. 30. Sato T, Takeichi M, Shirahama M, Fukui T, Gude JK. Doctor-shopping patients and users of alternative medicine among Japanese primary care patients. General hospital psychiatry. 1995;17(2):115-25. 31. Mercer SW, Siu JY, Hillier SM, Lam CL, Lo YY, Lam TP, et al. A qualitative study of the views of patients with long-term conditions on family doctors in Hong Kong. BMC family practice. 2010;11:46. 32. Siu JY. "Seeing a doctor is just like having a date": a qualitative study on doctor shopping among overactive bladder patients in Hong Kong. BMC family practice. 2014;15:27. 33. Wang MJ, Lin SP. Study on doctor shopping behavior: insight from patients with upper respiratory tract infection in Taiwan. Health Policy. 2010;94(1):61-7. 34. Zhao ZW, Wang WR. Modified Qiju Dihuang decoction in the treatment of 30 cases of primary Sjögren's syndrome. Chinese Journal of Traditional Medical Science and Technology. 2003;10:314–5. 35. Zhou Q, Zhu HQ. Integrated traditional Chinese and western medicine in the treatment of 34 cases of Sjögren's syndrome. Journal of New Chinese Medicine. 1997;29:29-30. 36. Chang YH, Lin HJ, Li WC. Clinical evaluation of the traditional chinese prescription Chi-Ju-Di-Huang-Wan for dry eye. Phytotherapy research : PTR. 2005;19(4):349-54. 37. Lin IH. Mucositis and dry mouth due to NPC radiotherapy treated by Chinese herb Gan-Lu-Yin. Yearbook of Chinese Medicine abd Pharmacy. 2000;8(6):127-45. 38. Yi Y-M, Yi J-L, Cheng X-H, Zuo Z-Q, Luo Y-Y. Efficacy of Modified Xiaoyaosan in Perimenopausal Women with Xerophthalmia. Practical Clinical Medicine. 2013;14(4):82-5. 39. Ji C-Z, Zhang P-Y, Wang Y-X, Zhang D-S, Zhang L. Effect of Xuefuzhuyu soup on the levels of IL-2 and SIL-2R in mice serum. Journal of Qiqihar Medical. 1999;1(06):540-1. 40. Shao S-j. The clinical application and research progress of Xie-Fu-Zhu-Yu-Tang. Beijing Journal of Traditional Chinese Medicine. 2008;27(9):724-7. 41. Shen X, Eichhorn T, Greten HJ, Efferth T. Effects of Scrophularia ningpoensis Hemsl. on Inhibition of Proliferation, Apoptosis Induction and NF-kappaB Signaling of Immortalized and Cancer Cell Lines. Pharmaceuticals (Basel). 2012;5(2):189-208. 42. Chen XM, Tang J, Xie WY, Wang JJ, Jin J, Ren J, et al. Protective effect of the polysaccharide from Ophiopogon japonicus on streptozotocin-induced diabetic rats. Carbohyd Polym. 2013;94(1):378-85. 43. Hsu CH, Yu MC, Lee CH, Lee TC, Yang SY. High eosinophil cationic protein level in asthmatic patients with "heat" Zheng. American Journal of Chinese Medicine. 2003;31(2):277-83. 44. Arawwawala M, Thabrew I, Arambewela L, Handunnetti S. Anti-inflammatory activity of Trichosanthes cucumerina Linn. in rats. Journal of Ethnopharmacology. 2010;131(3):538-43. 45. Wang SC, Chen SF, Lee YM, Chuang CL, Bau DT, Lin SS. Baicalin Scavenges Reactive Oxygen Species and Protects Human Keratinocytes Against UVC-induced Cytotoxicity. In Vivo. 2013;27(6):707-14. 46. Peng H-r. Great Compendium of Chinese Medical Formulae. 1 ed. Beijing: People's Medical Publishing House; 2005. 47. Medicine NUoC. Chinese medical Great Dictionary. 2 ed. Shanghai: Shanghai Science and Technology Press; 2006. Authors: Ching-Mao Chang 1,2, Hsueh-Ting Chu 3,4,d, Yau-Huei Wei 5,6, Fang-Pey Chen 2, Shengwen Wang 7, Po-Chang Wu 8, Hung-Rong Yen 9,a,d, Tzeng-Ji Chen b,c,*, Hen-Hong Chang 1,9,a,d,* Affiliation: 1 Graduate Institute of Clinical Medicine, and Graduate Institute of Traditional Chinese Medicine, College of Medicine, Chang Gung University, Taoyuan 33378, Taiwan 2 Center for Traditional Medicine, Taipei Veterans General Hospital, Taipei 11217, Taiwan 3 Department of Computer Science and Information Engineering, Asia University, Taichung 41354, Taiwan 4 Department of Medical Research, China Medical University Hospital, China Medical University, Taichung 40447, Taiwan 5 Department of Biochemistry and Molecular Biology, School of Life Sciences, National Yang-Ming University, Taipei 11221, Taiwan 6 Department of Medicine, Mackay Medical College, New Taipei 25245, Taiwan 7 Cloud Computing and System Integration Division, National Center for High-Performance Computing, Taichung 40763, Taiwan 8 Division of Rheumatology and Immunology and Department of Education, China Medical University Hospital, Taichung 40447, Taiwan 9 Research Center for Traditional Chinese Medicine, Department of Chinese Medicine and Department of Medical Research, China Medical University Hospital, Taichung 40447, Taiwan a School of Chinese Medicine, China Medical University, Taichung 40447, Taiwan b Department of Family Medicine, Taipei Veterans General Hospital, Taipei 11217, Taiwan c Institute of Hospital and Health Care Administration, School of Medicine, National Yang-Ming University, Taipei 11217, Taiwan d Research Center for Chinese Medicine & Acupuncture, China Medical University, Taichung 40447, Taiwan * Correspondence and co-correspondence to: Prof. Hen-Hong Chang and Prof. Tzeng-Ji Chen Table 1. Age distribution of Sjögren's syndrome patients with catastrophic illness certificate treated with Chinese herbal medicine Total Number Age < 20 20-29 30-39 40-49 Female Male Female/Male Ratio 366 339 27 12.56 1 (0.27%) 9 (2.46%) 38 (10.38%) 72 (19.67%) 1 (0.29%) 7 (2.06%) 36 (10.62%) 68 (20.06%) 0 (0.00%) 2 (7.41%) 2 (7.41%) 4 (14.81%) 3.5 18 17 50-59 60-69 70-79 ≧ 80 108 (29.51%) 86 (23.50%) 40 (10.93%) 12 (3.28%) 101 (29.79%) 81 (23.89%) 36 (10.62%) 9 (2.65%) 7 (25.93%) 5 (18.52%) 4 (14.81%) 3 (11.11%) 14.43 16.2 9 3 Mean ± SD Max Min Range 55.05 ± 13.28 90 16 74 54.82 ± 13.00 90 16 74 57.96 ± 16.42 85 28 57 Table 2. Visit distribution of patients and doctors of Sjögren's syndrome with catastrophic illness certificate in the treatment of Chinese herbal medicine Patient Number Total Visit < 10 10-19 20-29 30-39 Doctor 366 4867 472 4867 238 (65.03%) 55 (15.03%) 19 (5.19%) 19 (5.19%) 343 (72.67%) 66 (13.98%) 26 (5.51%) 9 (1.91%) 40-49 50-59 60-69 70-79 10 (2.73%) 11 (3.01%) 1 (0.27%) 5 (1.37%) 6 (1.27%) 5 (1.06%) 2 (0.42%) 2 (0.42%) 80-89 90-99 100-109 110-119 120-129 130-139 ≧ 140 3 (0.82%) 1 (0.27%) 2 (0.55%) 1 (0.27%) 1 (0.27%) 0 (0.00%) 4 (0.85%) 6 (1.27%) 1 (0.21%) 0 (0.00%) 0 (0.00%) 0 (0.00%) 0 (0.00%) 13.30 ± 20.09 129 1 128 2 (0.42%) 10.31 ± 19.15 143 1 142 Mean ± SD Max Min Range Table 3. The top 10 formulae of Sjögren's syndrome with catastrophic illness certificate in Taiwan (total prescription numbers =26,733) TCM prescription 1 2 Qi-Ju-Di-Huang-Wan Gan-Lu-Yin Therapeutic actions and indications (46) Frequency of prescription N (%) Average daily dosage (g) (Mean ± SD) Ju-Hua (Chrysanthemum morifolium Nourish the liver and 834 (9.08%) 4.78 ± 1.62 (Ramat.) Tzvel.), Gou-Qi (Lycium barbarum L.), Shou-Di-Huang (Rehmannia glutinosa Libosch.), Shan-Zhu-Yu (Cornus officinalis Sieb. et Zucc.), Shan-Yao (Dioscorea opposita Thunb.), Ze-Xie (Alisma orientalis (Sam.) Juzep.), Fu-Ling (Poria cocos (Schw.) Wolff), Mu-Dan-Pi brighten the eyes 750 (8.16%) 4.37 ± 1.78 Ingredients (Paeonia suffruticosa Andr.) Sheng-Di-Huang (raw Rehmannia glutinosa Libosch.), Shou-Di-Huang (Rehmannia glutinosa Libosch.), Tian-Men-Dong (Asparagus cochinchinensis (Lour.) Merr.), Mai-Men-Dong (Ophiopogon japonicus (L. f.) Ker-Gawl.), Shi-Hu (Dendrobium chrysanthum Wall.), Yin-Chen-Hao (Artemisia capillaris Thunb.), Huang-Qin (Scutellaria baicalensis Georgi), Zhi-Ke Enrich yin and clear heat 3 Jia-Wei-Xiao-Yao-San (Citrus aurantium L.), Pi-Pa-Ye (Eriobotrya japonica (Thunb.) Lindl.), Zhi-Gan-Cao (Glycyrrhiza glabra L.) Zhi-Gan-Cao (Glycyrrhiza glabra L.), Course the liver and Dang-Gui (Angelica sinensis (Oliv.) Diels), resolve depression 553 (6.02%) 4.70 ± 1.49 Boost qi and enrich yin 189 (2.06%) 3.65 ± 2.23 Mai-Men-Dong (Ophiopogon japonicus (L. f.) Ker-Gawl.), Ma-Zi-Ren (Cannabis sativa L.), Da-Zao (Ziziphus jujuba Mill.) Xue-Fu-Zhu-Yu-Decoction Dang-Gui (Angelica sinensis (Oliv.) Diels), Quicken the blood and 187 (2.03%) 4.50 ± 2.21 Fu-Ling (Poria cocos (Schw.) Wolff), Bai-Shao-Yao (Paeonia lactiflora Pall.) , Bai-Zhu (Atractylodes macrocephala Koidz.), Chai-Hu (Bupleurum chinense DC.), Sheng-Jiang (Zingiber officinale Rosc.), Bo-He (Mentha haplocalyx Briq.), Mu-Dan-Pi (Paeonia suffruticosa Andr.), 4 Zhi-Gan-Cao-Tang Zhi-Zi (Gardenia jasminoides Ellis) Zhi-Gan-Cao (Glycyrrhiza glabra L.), Sheng-Jiang (Zingiber officinale Rosc.), Ren-Can (Panax ginseng C. A. Meyer), Sheng-Di-Huang (raw Rehmannia glutinosa Libosch.), Gui-Zhi (Cinnamomun cassia Presl), A-Jiao (Equus asinus L.), 5 Sheng-Di-Huang (raw Rehmannia glutinosa dispel stasis Libosch.), Tao-Ren (Prunus persica (L.) Batsch), Hong-Hua (Carthamus tinctorius L.), Zhi-Ke (Citrus aurantium L.), Chi-Shao (red Paeonia lactiflora Pall.), Chai-Hu 6 Yi-Guan-Jian (Bupleurum chinense DC.), Zhi-Gan-Cao (Glycyrrhiza glabra L.), Jie-Geng (Platycodon grandiflorum (Jacq.) A. DC.), Chuan-Qiong (Ligusticum chuanxiong Hortorum), Niu-Xi (Achyranthes bidentata Blume) Dang-Gui (Angelica sinensis (Oliv.) Diels), Bai-Zhu (Atractylodes macrocephala Koidz.), Fu-Ling (Poria cocos (Schw.) Coursing the liver and 185 (2.01%) 3.58 ± 1.44 183 (1.99%) 4.27 ± 1.56 fortify the spleen Wolff), Gou-Teng (Uncaria rhynchophylla (Miq.) Jacks.), Chuan-Qiong (Ligusticum chuanxiong Hortorum), Chai-Hu (Bupleurum chinense DC.), Zhi-Gan-Cao (Glycyrrhiza glabra L.) 7 Zhi-Bo-Di-Huang-Wan Zhi-Mu (Anemarrhena asphodeloides Bunge), Huang-Bo (Phellodendron chinense Schneid.), Shou-Di-Huang (Rehmannia glutinosa Libosch.), Enrich yin and clear heat Shan-Zhu-Yu (Cornus officinalis Sieb. et Zucc.), Shan-Yao (Dioscorea opposita Thunb.), Ze-Xie (Alisma orientalis (Sam.) Juzep.), Fu-Ling (Poria cocos (Schw.) Wolff), Mu-Dan-Pi (Paeonia suffruticosa 8 Ping-Wei-San 9 Sha-Can-Mai-Dong-Tang Andr.) Cang-Zhu (Atractylodes lancea (Thunb.) DC.), Hou-Po (Magnolia officinalis Rehd. et Wils.), Chen-Pi (Citrus reticulata Blanco), Zhi-Gan-Cao (Glycyrrhiza glabra L.) Sha-Can (Glehnia littoralis F. Schmidt ex Miq.), Yu-Zhu (Polygonatum odoratum (Mill.) Druce), Sheng-Gan-Cao ( raw Dry dampness and fortify the spleen 183 (1.99%) 2.56 ± 1.09 Nourish yin and engender 174 (1.89%) 4.31 ± 1.93 165 (1.80%) 2.78 ± 1.59 liquid Glycyrrhiza glabra L.), Sang-Ye (Morus alba L.), Mai-Men-Dong (Ophiopogon japonicus (L. f.) Ker-Gawl.), Bian-Dou (Dolichos lablab L.), Tian-Hua-Fen (Trichosanthes kirilowii Maxim.) 10 Ma-Zi-Ren-Wan Ma-Zi-Ren (Cannabis sativa L.), Bai-Shao-Yao (Paeonia lactiflora Pall.), Zhi-Shi (Citrus aurantium L.), Da-Huang (Rheum tanguticum Maxim. ex Balf.), Moisten the intestines and drain fire 29 Sang-Ju-Yin Hou-Po (Magnolia officinalis Rehd. et Wils.), Xing-Ren (Prunus armeniaca L.) Sang-Ye (Morus alba L.), Ju-Hua (Chrysanthemum morifolium (Ramat.) Tzvel.), Xing-Ren (Prunus armeniaca L.), Lian-Qiao (Forsythia suspense (Thunb.) Vahl), Bo-He (Mentha haplocalyx Briq.), Jie-Geng (Platycodon grandiflorum (Jacq.) A. DC.), Zhi-Gan-Cao (Glycyrrhiza glabra L.), Lu-Gen (Phragmites communis Trinus) Course wind and discharge heat 89 (0.97%) 3.75 ± 1.26 Table 4. The top 10 single herbs of Sjögren's syndrome with catastrophic illness certificate in Taiwan (total prescription numbers =26,733) TCM prescription Xuan-Can Mai-Men-Dong Sheng-Di-Huang Tian-Hua-Fen Huang-Qin Gou-Qi Da-Huang Ju-Hua Dan-Can Shi-Hu Therapeutic actions and indications (47) Frequency of prescription N (%) Scrophularia ningpoensis Hemsl. Ophiopogon japonicus (L. f.) Ker-Gawl. raw Rehmannia glutinosa Libosch. Trichosanthes kirilowii Maxim. Scutellaria baicalensis Georgi Lycium barbarum L. Enrich yin and clear heat Nourish yin and moisten dryness 522 (2.98%) 514 (2.93%) 1.86 ± 0.41 1.38 ± 0.58 Enrich yin and clear heat Clear heat and engender liquid Clear heat and drain fire Boost essence and brighten the eyes 380 (2.17%) 357 (2.04%) 342 (1.95%) 322 (1.84%) 1.42 ± 0.52 1.24 ± 0.46 1.24 ± 0.46 1.27 ± 0.59 Rheum tanguticum Maxim. ex Balf. Chrysanthemum morifolium (Ramat.) Tzvel. Salvia miltiorrhiza Bge. Dendrobium chrysanthum Wall. Clear heat and drain fire Course wind and discharge heat 294 (1.68%) 292 (1.66%) 1.07 ± 0.73 1.18 ± 0.38 Cool the blood and clear heat Enrich yin and clear heat 289 (1.65%) 282 (1.61%) 1.20 ± 0.44 1.23 ± 0.46 Ingredients Average daily dosage (g) (Mean ± SD) Table 5. The most common prescription patterns for two formulae and two single herbs combination in a single prescription of Sjögren's syndrome with catastrophic illness certificate Number of prescriptions N (%) Name Two formulae combination 1 Qi-Ju-Di-Huang-Wan 2 Jia-Wei-Xiao-Yao-San 3 Jia-Wei-Xiao-Yao-San Gan-Lu-Yin Qi-Ju-Di-Huang-Wan Ping-Wei-San 268 (3.34%) 102 (1.27%) 68 (0.85%) 4 5 6 7 Jia-Wei-Xiao-Yao-San Gan-Lu-Yin Jia-Wei-Xiao-Yao-San Qi-Ju-Di-Huang-Wan Zhi-Bo-Di-Huang-Wan Sang-Ju-Yin Gan-Lu-Yin Shen-Tong-Zhu-Yu-Tang 57 (0.71%) 56 (0.70%) 55 (0.69%) 53 (0.66%) 8 9 10 Jia-Wei-Xiao-Yao-San Jia-Wei-Xiao-Yao-San Qi-Ju-Di-Huang-Wan Huang-Lian-Jie-Du-Tang Ma-Zi-Ren-Wan Xin-Yi-Qing-Fei-Tang 51 (0.64%) 49 (0.61%) 42 (0.52%) Two single herbs combination 1 Xuan-Can Mai-Men-Dong 2 Sheng-Di-Huang Mai-Men-Dong 3 4 5 6 7 8 9 10 # Xuan-Can Gou-Qi Sha-Can Tian-Men-Dong Mu-Dan-Pi Wu-Wei-Zi Tian-Hua-Fen Nu-Zhen-Zi Sheng-Di-Huang Mai-Men-Dong Mai-Men-Dong Mai-Men-Dong Huang-Qin Gou-Qi Mai-Men-Dong Wu-Wei-Zi 176 (0.41%) 160 (0.37%) 152 (0.35%) 93 (0.22%) 92 (0.21%) 88 (0.20%) 88 (0.20%) 79 (0.18%) 79 (0.18%) 75 (0.17%) Nu-Zhen-Zi: Ligustrum lucidum Ait., Wu-Wei-Zi: Schizandra chinensis (Turcz.) Baill., Table 6 The most common prescription patterns for two and triple drugs combination in a single prescription of Sjögren's syndrome with catastrophic illness certificate Number of prescriptions N (%) Name Two combination 1 Qi-Ju-Di-Huang-Wan 2 Xuan-Can 3 Sheng-Di-Huang 4 5 6 7 8 9 10 3 4 5 6 7 8 9 10 # Mai-Men-Dong Mai-Men-Dong Xuan-Can Sheng-Di-Huang Xuan-Can Gan-Lu-Yin Qi-Ju-Di-Huang-Wan Mai-Men-Dong Tian-Hua-Fen Gan-Lu-Yin Xuan-Can Qi-Ju-Di-Huang-Wan Jia-Wei-Xiao-Yao-San Qi-Ju-Di-Huang-Wan Sheng-Di-Huang Qi-Ju-Di-Huang-Wan Triple combination 1 Xuan-Can 2 Nu-Zhen-Zi 268 (0.322%) 176 (0.212%) 160 (0.193%) Gan-Lu-Yin 152 (0.183%) 130 (0.156%) 123 (0.148%) 113 (0.136%) 110 (0.132%) 102 (0.123%) 95 (0.114%) Sheng-Di-Huang Mai-Men-Dong Jia-Wei-Xiao-Yao-San Gou-Qi Nu-Zhen-Zi Wu-Wei-Zi Jia-Wei-Xiao-Yao-San Wu-Wei-Zi Jia-Wei-Xiao-Yao-San Gou-Qi Qi-Ju-Di-Huang-Wan Gan-Lu-Yin Dan-Can Nu-Zhen-Zi Wu-Wei-Zi Gou-Qi Jia-Wei-Xiao-Yao-San Ping-Wei-San Bai-Ji Da-Huang Bai-Hua-She-She-Cao Mei-Yao Jia-Wei-Xiao-Yao-San Gou-Qi Hai-Piao-Xiao Xuan-Can Gan-Lu-Yin Qi-Ju-Di-Huang-Wan 96 (0.055%) 66 (0.038%) 66 (0.038%) 64 (0.037%) 63 (0.036%) 59 (0.034%) 52 (0.030%) 49 (0.028%) 47 (0.027%) 47 (0.027%) Bai-Ji: Bletilla striata (Thunb.) Rechib. f., Mei-Yao: Commiphora myrrha Engler, Hai-Piao-Xiao: Sepia esculenta Hoyle Figure Legends Figure 1. Flowchart of recruitment of Sjögren's syndrome with catastrophic illness certificate from the 3-million random sample. We identified the Sjögren's syndrome with ICD-9 code “710.2” with catastrophic illness certificate in Taiwan between years 2002, and they were matched with three cohorts of one million random samples from the LHID2000, LHID2005 and LHID2010. And the subjects with catastrophic illness certificate were included in this study after duplicating data were removed. Figure 2. Relationship between the numbers of Chinese formula and single herbs for the Sjögren's syndrome patients. Sjögren's syndrome patients with catastrophic illness certificate was given an average item of 6.24 ± 2.47 CHMs in a single prescription, and five items of CHMs (16.85%) was the most common prescription with the combination of formulae or single herbs. Figure 3. The core pattern of Chinese formula and single herbs for the Sjögren's syndrome patients. The top 50 Chinese formula and single herbs for the Sjögren's syndrome patients with catastrophic illness certificate were analyzed through an open-sourced freeware NodeXL and the core pattern of these CHMs showed that Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Mai-Men-Dong and Sheng-Di-Huang are among the most frequently used combinations. Figure 1. Flowchart of recruitment of Sjögren's syndrome with catastrophic illness certificate from the 3-million random sample. We identified the Sjögren's syndrome with ICD-9 code “710.2” with catastrophic illness certificate in Taiwan between years 2002, and they were matched with three cohorts of one million random samples from the LHID2000, LHID2005 and LHID2010. And the subjects with catastrophic illness certificate were included in this study after duplicating data were removed. Figure 2. Relationship between the numbers of Chinese formula and single herbs for the Sjögren's syndrome patients. Sjögren's syndrome patients with catastrophic illness certificate was given an average item of 6.24 ± 2.47 CHMs in a single prescription, and five items of CHMs (16.85%) was the most common prescription with the combination of formulae or single herbs. Figure 3. The core pattern of Chinese formula and single herbs for the Sjögren's syndrome patients. The top 50 Chinese formula and single herbs for the Sjögren's syndrome patients with catastrophic illness certificate were analyzed through an open-sourced freeware NodeXL and the core pattern of these CHMs showed that Qi-Ju-Di-Huang-Wan, Gan-Lu-Yin, Xuan-Can, Mai-Men-Dong and Sheng-Di-Huang are among the most frequently used combinations.