GRAND ROUNDS

GRAND ROUNDS
Desiree Ong, M.D.
Vanderbilt Eye Institute
12/15/06
Our Patient
• CC: “Droopy eyelid”
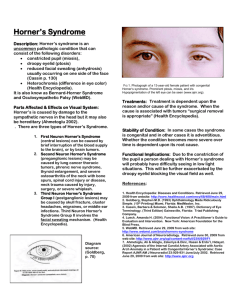
• HPI: 7 mo old male with unequal pupil size x 3 days noted by mother. Pt was evaluated at an outside ER, head CT was negative. Over the next 24 hrs, mother noticed that left eyelid began to droop.
History
• POHx: none
• PMHx: full-term, normal birthweight, no complications
• FHx: no eye disease, healthy 6 yo sibling
• Social hx: non-contributory
• Allergies: NKDA
• Meds: none
Exam
• VA: Fixes and follows
• Pupils: OD bright 4-->3mm dim 5.5-->4.5mm
OS bright 2.5-->2mm dim 2-->1.5mm
• Motility: grossly full OU
• Tp: soft to palpation OU
Exam continued
• PLE
– External: palpebral fissure OD 9mm, OS 6mm, small movable cervical nodes left>right
– Lids/lashes: quiet OU, mild ptosis OS
– S/C: quiet OU
– K: quiet OU
– A/C: formed OU
– Iris: intact OU
– Lens: clear OU
• DFE
– WNL OU, C/D 0.2 OU
Sympathetic Pathway
Differential diagnosis?
Acquired Pediatric Horner Syndrome
Differential Diagnosis
Acquired Pediatric Horner Syndrome
• First-order lesions (hypothalamus to C8-T2)
– Meningitis
– Basal skull tumors, pituitary tumor
– Brain stem vascular malformation
– Cerebral vascular accident
– Demyelinating disease
– Intrapontine hemorrhage
– Neck trauma/cervical disk disease
• Second-order (preganglionic) lesions (T1 to SCG)
– Neuroblastoma
– Lymphadenopathy (reactive or malignant)
– Apical lung tumors
– Metastases
– Mandibular tooth abscess
– Lesions of the middle ear (eg, acute otitis media)
– Thyroid adenoma
– Thoracic aorta, subclavian or common carotid artery aneurysm
– Trauma/surgical injury/chest tube/central venous catheter
• Third-order lesions (SCG to post-ganglionic neurons)
– Internal carotid dissection/aneurysm/vasopasm
– Extension of cavernous sinus tumor, nasopharyngeal tumor
– Carotid cavernous fistula
– Cluster/migraine headaches
– Herpes zoster
– Otitis media
– Neck trauma/tumor (i.e. rhabdomyosarcoma)/inflammation
• Drugs
– Bupivacaine
– Chlorprocaine
– Chlorpromazine
– Deserpidine
– Diacetylmorphine
– Diethazine
– Fluphenazine
– Guanethidine
– Influenza virus vaccine
– Levodopa
- Lidocaine
- Mepivacaine
- Mesoridazine
- Oral contraceptives
- Procaine
- Prochlorperazine
- Promethazine
- Propoxycaine
- Reserpine
- Thioridazine
Lab Results
• Pt was admitted for observation
• CXR: negative
• MRI/CT brain/chest/abdomen: negative
• CBC, CMP, HVA/VMA urine tests were
WNL
• LDH was elevated at 552
Horner Syndrome
• Ptosis denervation of Müller muscle
• “Reverse ptosis” - lower lid elevation
• Miosis - greater in dim light (dilation lag)
• Anhidrosis – impaired flushing and sweating
– First-order: ipsilateral body
– Second-order: ipsilateral face
– Post-ganglionic (third-order): absent or limited
• Iris heterochromia – affected iris is lighter
- Congenital or children < 2 yrs
- Long-standing lesions
Other associations
• First-order lesions :
– Hemisensory loss, weakness, dysarthria, dysphagia, ataxia, vertigo, and nystagmus
• Second-order lesions :
– H/o trauma/surgery, facial/neck, axillary/shoulder or arm pain/swelling, cough, hemoptysis
• Third-order lesions :
– Diplopia (CN VI palsy), numbness/pain in V1 and V2
• Cluster headaches
– may cause temporary or permanent Horner syndrome
Testing
• No standard evaluation protocol
• Previous studies suggested that a h/o birth trauma or urine studies alone is sufficient 3
• CBC, FTA-ABS, VDRL, PPD
• VMA and HVA urine tests
– positive in 90-95% with neuroblastomas
– localized tumors may be associated with normal urine studies 2
• MRI/MRA, extracranial Doppler, and/or chest x-ray
Testing
• Cocaine (4% or 10%)
– Inhibits the re-uptake of norepinephrine
– Denervation poor dilation regardless of level
– Anisocoria greater than 0.8 mm = positive
• Apraclonidine (0.5% or 1%)
– Alpha-receptor agonist
– Denervation supersensitivity of the iris dilator
– Reversal of anisocoria = positive
Chen et al. (2006)
• Small randomized crossover study (10 pts)
• Testing with 0.5% apraclonidine and 4% cocaine
• Mean differences in pupil diameter
-before/after 4% cocaine = -2.08/-2.97 mm
(p=0.0047)
-before/after 0.5% apraclonidine = -2.04/+1.08 mm (p=0.005)
• Conjunctival hyperemia in two patients
• Conclusion: 0.5% apraclonidine is safe and effective for diagnosis of Horner syndrome in children
Chen PL, Chen JT, Lu DW, Chen YC, Hsiao CH. Comparing efficacies of 0.5% apraclonidine with 4% cocaine in the diagnosis of Horner syndrome in pediatric patients. J Ocul Pharmacol Ther. 2006 Jun;22(3):182-7.
Testing
• Hydroxyamphetamine 1% (Paredrine)
– Stimulates presynaptic norepinephrine release
– Distinguishes presynaptic from postganglionic lesions
– 40-97% sensitive; inaccurate within 24-48 hours of cocaine test
– Failure of affected pupil to dilate equally or greater to normal pupil = third-order lesion
Mahoney et al. (2006)
• Retrospective review (56 children)
• 28 (50%) had no previously identified cause
- 18 with complete imaging and urine studies
- Mass lesions found in 6/18 (33%); 4 had neuroblastoma; all negative urine studies
• Of all patients, 13/56 had a neoplasm (23%)
• Conclusions:
- Urine testing alone is inadequate
- Recommend physical exam with palpation
- MRI brain/neck/chest, VMA and HVA by spot
Mahoney NR, Liu GT, Menacker SJ, Wilson MC, Hogarty MD, Maris JM. Pediatric Horner syndrome: etiologies and roles of imaging and urine studies to detect neuroblastoma and other responsible mass lesions. Am J Ophthalmol. 2006 Oct;142(4):651-9
Cervical Lymphadenopathy in Children
• Acute bilateral - adenovirus, influenza, RSV; EBV and CMV
• Acute unilateral - strep or staph (40-80%)
• Indications for biopsy:
- Persistent enlargement
- Solid fixed or supraclavicular mass
- Constitutional signs and symptoms
• Increased risk for malignancy: 8
- Generalized LAD
- LAD > 3 cm
- Hepatosplenomegaly
- High LDH levels
Cervical Lymphadenopathy in
Children
• Subacute/chronic LAD
– Cat scratch, mycobacteria, and toxoplasmosis
– EBV, CMV, histoplasmosis, HIV
– Leukemia, lymphoma, neuroblastoma, rhabdomyosarcoma, and nasopharyngeal carcinoma
• Laboratory tests are not necessary in majority
• Most cases are self-limited and require no treatment
Cervical Lymphadenopathy
Oguz et al. (2006)
- Retrospective review
- 457 children aged 2 mo -19 yrs
- 76% benign, 24% malignant
- 61% of the benign group had an unknown etiology
- Most common benign etiologies: EBV and acute lymphadenitis
Most common malignant: Hodgkin’s and NHL
- None in the infant group had a malignant process
Oguz A and Karadeniz C. Evaluation of Peripheral Lymphadenopathy in Children. Pediatric
Hematology and Oncology. 23:549-561, 2006.
Our Patient
• Started on Unasyn
• Improvement was noted over the next few days
• Repeat CT showed decreased necrosis
• Persistent Horner syndrome, monitored closely
• Recently started on 10 days of Omnicef for a persistent otitis media/URI
Take Home Points
• Horner syndrome may be the first symptom of a potentially serious condition
• Children with Horner syndrome should undergo a thorough physical exam with urine testing and
MRI
• Acute cervical lymphadenopathy in children usually has an infectious cause but should be monitored closely
References
3.
4.
5.
8.
9.
6.
7.
1.
2.
Chen PL, Chen JT, Lu DW, Chen YC, Hsiao CH. Comparing efficacies of 0.5% apraclonidine with 4% cocaine in the diagnosis of Horner syndrome in pediatric patients. J Ocul Pharmacol Ther. 2006 Jun;22(3):182-7.
Fritsch P, Kerbl R, Lackner H, et al. “Wait and see” strategy in localized neuroblastoma in infants: an option not only for cases detected by mass screening.
Pediatr Blood Cancer 2004;43:679-682.
George ND, Gonzalez G, Hoyt CS. Does Horner's syndrome in infancy require investigation? J Ophthalmol. 1998 Jan;82(1):51-4
Leung AK, Robson WL. Childhood cervical lymphadenopathy. J Pediatr Health Care.
2004 Jan-Feb;18(1):3-7
Mahoney NR, Liu GT, Menacker SJ, Wilson MC, Hogarty MD, Maris JM. Pediatric horner syndrome: etiologies and roles of imaging and urine studies to detect neuroblastoma and other responsible mass lesions. Am J Ophthalmol. 2006
Oct;142(4):651-9
Oguz A and Karadeniz C. Evaluation of Peripheral Lymphadenopathy in Children.
Pediatric Hematology and Oncology. 23:549-561, 2006.
Sauer C, Levingohn MW. Horner's syndrome in childhood. Neurology. 1976
Mar;26(3):216-20
Twist CJ. Assessment of lymphadenopathy in children. Pediatr Clin North Am
2002;49(5):1009-1025.
Yaris N et al. Analysis of Children with Peripheral lymphadenopathy. Clinical
Pediatrics. 2006;45:544-549.