Cardiogenic Shock: Look, Listen and Treat
advertisement

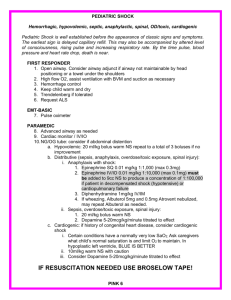
INTRA-AORTIC BALLOON COUNTERPULSATION CARDIOGENIC SHOCK: LOOK, LISTEN AND TREAT Class Code: 220 MCV00018180 REVA LEARNING OBJECTIVES At the conclusion of this program, the participants will be able to: Identify the signs and symptoms of cardiogenic shock Identify two factors that place a patient at risk for developing cardiogenic shock Discuss what is currently being stated in the literature regarding the usefulness of IABC in the setting of cardiogenic shock MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND MCV00018180 MCV00018180 REVA REVA CARDIOGENIC SHOCK — BACKGROUND CARDIOGENIC SHOCK – NRMI DATABASE 1995 - 2004 CS developed in 8.6% of patients with acute myocardial infarction (ST-segment elevation or left bundle branch block) hospitalized in 775 U.S. hospitals with revascularization capability Overall in-hospital mortality decreased from 60.3% in 1995 to 47.9% in 2004 29% of patients with CS were in shock as they presented to hospital 71% developed CS after admission CS patients were more likely to have a history of hypertension, dyslipidemia, and prior coronary angioplasty Source: Crit Care Med 2008 Vol. 36, No. 1 (Suppl.) MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND CARDIOGENIC SHOCK — BACKGROUND Definition of Cardiogenic Shock State of inadequate tissue perfusion due to cardiac dysfunction or a state of end-organ hypo-perfusion due to cardiac failure Mortality rate for Cardiogenic Shock 50% - 80% Incidence of Cardiogenic Shock 5% - 8% Cardiogenic shock is the leading cause of death for patients hospitalized with acute MI Source: Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND THE PATHOPHYSIOLOGY OF CARDIOGENIC SHOCK Myocardial injury causes systolic and diastolic dysfunction A decrease in cardiac output leads to a decrease in systemic and coronary perfusion This reduction in systemic and coronary perfusion worsens ischemia and causes cell death in the infarct border zone and the remote zone of myocardium Source: Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND ACUTE MYOCARDIAL INFARCTION AND CARDIOGENIC SHOCK The most common cause of cardiogenic shock is extensive acute myocardial infarction Patients with previous impairment of ventricular function may also experience shock with the occurrence of a small infarction The cardiovascular system fails to maintain sufficient perfusion resulting in inadequate cellular metabolism and eventually cell death The consequence is irreversible cell damage Source: Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND TIMEFRAME FOR DEVELOPMENT OF CARDIOGENIC SHOCK Median time frame for development of cardiogenic shock is 12 hours into AMI 39.6% develop cardiogenic shock within 6 hours 63.2% develop cardiogenic shock within 24 hours The majority of patients develop shock after arrival to the hospital Source: Hasdai D, et al. American Heart Journal. 1999;138 (1 Pt 1):21-31 MCV00018180 REVA CARDIOGENIC SHOCK — BACKGROUND MCV00018180 REVA CARDIOGENIC SHOCK — IDENTIFICATION MCV00018180 MCV00018180 REVA REVA CARDIOGENIC SHOCK — IDENTIFICATION PATIENT PRESENTATION Appear ashen or cyanotic and have cool skin and mottled extremities Peripheral pulses are rapid and faint and may be irregular if arrhythmias are present Jugular venous distention and crackles in the lungs are usually (but not always) present Patients show signs of hypoperfusion, such as altered mental status and decreased urine output Source: Andrew Lenneman, MD. Cardiogenic Shock. Medscape Reference February 2011 MCV00018180 REVA CARDIOGENIC SHOCK — IDENTIFICATION CARDIOGENIC SHOCK HEMODYNAMIC PARAMETERS Systolic B/P <90 mmHg or a MAP 30 mmHg lower than baseline Cardiac Index <1.8 L/m/M2 without support and adequate filling pressures Cardiac Index <2.0-2.2 L/m/M2 with support and adequate filling pressures PCWP >15–18 mmHg Source: Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — IDENTIFICATION CARDIOGENIC SHOCK RISK FACTORS Four risk factors account for >85% of the predictive information needed to determine if a patient is at high risk to develop cardiogenic shock: Age Single greatest risk factor For every ten year increase in age, the risk of developing shock increases by 47% Systolic Blood Pressure HR Killip Class Source: Hasdai D, et al. American Heart Journal. 1999;138 (1 Pt 1):21-31 MCV00018180 REVA CARDIOGENIC SHOCK — CASE STUDY MCV00018180 MCV00018180 REVA REVA CARDIOGENIC SHOCK — CASE STUDY CARDIOGENIC SHOCK CALCULATION TABLE (EXAMPLE) 70-year-old, 60 kg female from the US with a history of hypertension, no prior PCTA, diagnosed with acute anterior MI. On admission, HR=123, B/P=112/70 and a few crackles in lungs Points Age 37 Systolic B/P 49 Weight 17 HR 17 Diastolic B/P 5 Killip Class 9 MI Location 8 Thrombolytics 0 Misc [6+3+2+5] 16 Total 155 40% probability of shock Source: Hasdai, D, et al; J Am Coll Cardiol 2000; 35:136-43 MCV00018180 REVA CARDIOGENIC SHOCK — CASE STUDY PATIENT CONDITION WHEN SHE LEFT THE CATH LAB AFTER SUCCESSFUL STENTING OF LAD HR=105, B/P=102/65 Few crackles in lungs when she left CCL MCV00018180 REVA CARDIOGENIC SHOCK — CASE STUDY NOW LET’S TAKE A LOOK AT THIS PATIENT 4 HOURS LATER IN THE CCU BP 80/40, HR – 135 Skin cool and clammy; becoming agitated Saturating 90% on 2L per N/C Crackles more prominent Short of breath with minimal activity Pulses weak and thready Has not urinated since admission 12 Lead EKG shows no changes MCV00018180 REVA 3/2/2010 V CARDIOGENIC SHOCK — CASE STUDY INTERVENTIONS 2D Echo at bedside No mechanical complications i.e. VSD or MR Shows wall motion abnormality 100% non-rebreather oxygen mask Fluid bolus 250cc NS Dopamine 10 mcg/kg/min Dobutrex 5 mcg/kg/min Lasix 40 mg IV Foley catheter placed Swan-Ganz Catheter inserted at bedside MCV00018180 REVA CARDIOGENIC SHOCK — CASE STUDY PATIENT CONDITION AFTER INTERVENTIONS BP 88/48; HR – 145; CI – 1.8 L; PCWP – 22 Skin remains cool and clammy Patient is lethargic Saturating 94% on 100% NRB Patient complains of difficulty breathing Pulses remain weak and thready Response from diuretic minimal 100 cc urine from catheter total MCV00018180 REVA CARDIOGENIC SHOCK — CASE STUDY FURTHER INTERVENTIONS AFTER NO IMPROVEMENT IN PATIENT CONDITION Considering intubation Dopamine increased to 20 mcg/kg/min Dobutrex 10 mcg/kg/min Bumex (diuretic) 4 mg IV given Preparing patient for IABP placement MCV00018180 REVA 3/2/2010 V CARDIOGENIC SHOCK — TREATMENT MCV00018180 MCV00018180 REVA REVA CARDIOGENIC SHOCK — TREATMENT CARDIOGENIC SHOCK PHARMACOLOGICAL TREATMENT Negative inotropes and vasodilators should be used in the lowest doses possible Higher doses results in poorer survival rates Positive inotropes increase myocardial ATP consumption resulting in a short term hemodynamic improvement The cost is an increased oxygen demand on the failing heart Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT CARDIOGENIC SHOCK GENERAL SUPPORT MEASURES Arterial oxygenation and near-normal pH should be maintained to minimize ischemia There should be a low threshold to institute mechanical ventilation via mask or ET tube Positive end-expiratory pressure decreases preload and afterload Mechanical ventilation also decreases the work of breathing Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT INDEPENDENT RISK FACTORS FOR LOWER SURVIVAL RATES Older age (p=0.0007) Shock on admission (p=0.012) Hx of hypertension (p=0.032) Creatinine > 1.9 (p<0.0001) Noninferior MI location (p=0.022) Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT KEY TO TREATMENT “Effective therapy for cardiogenic shock must include a prevention strategy. This requires identification of patients at high risk for shock development and selection patients who are candidates for aggressive intervention.” Source: Barry WL, et al. Clinical Cardiology 1998;21(2):72-80 MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT MECHANICAL SUPPORT WITH IABC IAB INFLATION: INCREASES SUPPLY OF OXYGEN TO MYOCARDIUM How it works Balloon inflates at onset of diastole (when aortic valve closes) Displaces blood, causing an increase in aortic pressure Benefits Increases coronary artery perfusion Increases mean arterial pressure MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT MECHANICAL SUPPORT WITH IABC IAB DEFLATION: DECREASES DEMAND FOR OXYGEN BY LEFT VENTRICLE How it works Balloon deflates just prior to systolic ejection (before aortic valve opens) Results in a rapid decrease in aortic pressure Benefits Decreases afterload Decreases cardiac workload Increases cardiac output MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT INDICATIONS — CARDIOGENIC SHOCK Source: Abdel-Wahab, et al; Am J Cardiol 2010;105:967-971 MCV00018180 REVA CARDIOGENIC SHOCK — TREATMENT CONCLUSION CS is a treatable illness with a reasonable chance for full recovery. It is important to realize that although patients with CS are at very high risk for early death, great potential exists for salvage. Clinicians and researchers must focus on the potential for full recovery if we are truly to make an impact on the burden of this disease. Prevention with very early reperfusion therapy remains the major goal. Source: Reynolds H, Hochman J; Circulation 2008;117(5):686-697 MCV00018180 REVA QUESTIONS? MCV00018180 MCV00018180 REVA REVA