External respiration - Mount Carmel Academy
advertisement

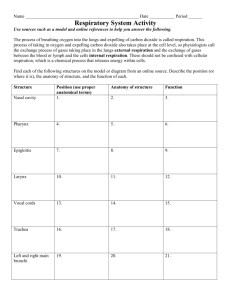
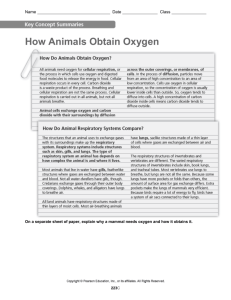
Chapter 13 – Part 2 The Respiratory System Events of Respiration The major function of the respiratory system is to supply the body with O2 and to dispose of CO2. To do this, at least four events must occur (collectively called respiration): 1. Pulmonary ventilation 2. External respiration 3. Respiratory gas transport 4. Internal respiration Events of Respiration 1. Pulmonary ventilation – moving air in and out of the lungs Commonly called breathing 2. External respiration – gas exchange between pulmonary blood and alveoli O2 loading and CO2 unloading Events of Respiration 3. Respiratory gas transport – transport of oxygen and carbon dioxide via the bloodstream to and from the lungs and body tissues 4. Internal respiration – gas exchange between blood and tissue cells in systemic capillaries Mechanics of Breathing (Pulmonary Ventilation) Completely mechanical process Depends on volume changes in the thoracic cavity Mechanics of Breathing (Pulmonary Ventilation) Volume changes lead to pressure changes, which lead to the flow of gases to equalize pressure A gas always conforms to the shape of its container In a large volume, the pressure will be low. If the volume is reduced, the gas molecules will be closer together and the pressure will rise. Mechanics of Breathing (Pulmonary Ventilation) Two phases 1. Inspiration – flow of air into the lungs 2. Expiration – air leaving the lungs Inspiration (Inhalation) Diaphragm and intercostal muscles contract resulting in the increased size of the thoracic cavity As the diaphragm contracts, it moves inferiorly and flattens out Contraction of the intercostals lifts the rib cage and thrusts the sternum forward Inspiration (Inhalation) The increased volume results in a decreased gas pressure within the lungs, which produces a partial vacuum External air is pulled into the lungs due to an increase in intrapulmonary volume Air continues to pull into the lungs until the intrapulmonary pressure equals the atmospheric pressure. Inspiration (Inhalation) Exhalation (Expiration) Largely a passive process which depends on natural lung elasticity As muscles relax, air is pushed out of the lungs Forced expiration can occur mostly by contracting internal intercostal muscles to depress the rib cage Exhalation (Expiration) Pressure Differences in the Thoracic Cavity Normal pressure within the pleural space (intrapleural pressure) is always negative Differences in lung and pleural space pressures keep lungs from collapsing If for any reason, the intrapleural pressure becomes equal to the atmospheric pressure, the lungs will collapse Atelectasis Atelectasis – lung collapse The lung is useless for ventilation Usually occurs when air enters the pleural space from: 1. A chest wound 2. A rupture of the visceral pleura Is reversed by drawing air out of the intrapleural space with chest tubes, which allows the lungs to re-inflate and resume its normal function Nonrespiratory Air Movements Can be caused by reflexes or voluntary actions Examples Cough - Clears the lower respiratory passages of debris Sneeze – Clears the upper respiratory passages of debris Laughing Crying Yawn – Increases ventilation to the lungs; May be initiated by a need to increase oxygen levels in the blood Hiccup – Sudden inspiration; Results from spasms of the diaphragm Respiratory Volumes and Capacities Tidal volume (TV) – Amount of air inhaled of exhaled with a normal breath Normal breathing moves about 500 ml of air (about a pint) with each breath Many factors that affect respiratory capacity 1. A person’s size 2. Sex 3. Age 4. Physical condition Respiratory Volumes and Capacities Inspiratory reserve volume (IRV) Amount of air that can be taken in forcibly over the tidal volume A person can inhale much more air than is taken in during a normal, or tidal, breath Usually between 2100 and 3200 ml Respiratory Capacities Respiratory Volumes and Capacities Expiratory reserve volume (ERV) Amount of air that can be forcibly exhaled After a normal expiration, more air can be exhaled Approximately 1200 ml Respiratory Volumes and Capacities Residual volume - Air remaining in the lungs after expiration Even after the most strenuous expiration, about 1200 ml of air still remains in the lungs The residual volume cannot be voluntarily expelled Is important because: 1. It allows gas exchange to go on continuously even between breaths 2. It helps to keep the alveoli open (inflated) Respiratory Capacities Respiratory Volumes and Capacities Vital capacity - the total amount of exchangeable air Vital capacity = TV + IRV + ERV Typically around 4800 ml in healthy young males Respiratory Volumes and Capacities Dead space volume - Air that remains in conducting zone and never reaches alveoli About 150 ml in a normal tidal breath Functional volume - Air that actually reaches the respiratory zone and contributes to gas exchange Usually about 350 ml Respiratory Volumes and Capacities Respiratory capacities are measured with a spirometer As a person breathes, the volumes of air exhaled can be read on an indicator Spirometer testing is useful for evaluating losses in respiratory functioning and in following the course of some respiratory diseases Respiratory Sounds Sounds are monitored with a stethoscope Bronchial sounds – Produced by air rushing through trachea and bronchi Vesicular breathing sounds – Occur as air fills the alveoli; soft sounds that resemble a muffled breeze Diseased respiratory tissue, mucus, or pus can produce abnormal sounds such as rales (a rasping sound) and wheezing (a whistling sound) External Respiration External respiration – the actual exchange of gases between the alveoli and the blood Oxygen movement into the blood Because body cells continually remove O2 from the blood, there is always more O2 in the alveoli than in the blood Oxygen moves by diffusion towards the area of lower concentration Pulmonary capillary blood gains oxygen External Respiration Carbon dioxide movement out of the blood Blood returning from tissues has higher concentrations of carbon dioxide than air in the alveoli Pulmonary capillary blood gives up carbon dioxide Blood leaving the lungs is oxygen-rich and carbon dioxide-poor Gas Transport in the Blood Oxygen is transported in the blood in two ways: 1. Most attaches to hemoglobin molecules inside the red blood cells to form oxyhemoglobin (HbO2) 2. A very small amount of oxygen is carried dissolved in the plasma Color change in blood Oxygen-rich blood = bright red Oxygen-poor blood = dark red Gas Transport in the Blood Carbon dioxide transport in the blood 1. Most is transported in the plasma as bicarbonate ion (HCO3–) Plays a very important role in the blood buffer system 2. A small amount is carried inside red blood cells on hemoglobin, but at different binding sites than those of oxygen Internal Respiration Internal respiration - exchange of gases between blood and body cells An opposite reaction to what occurs in the lungs Carbon dioxide diffuses out of tissue to blood Oxygen diffuses from blood into tissue Internal Respiration External Respiration, Gas Transport, and Internal Respiration Summary Hypoxia Hypoxia – Inadequate oxygen delivery to body tissues Impaired oxygen transport May be the result of anemia, pulmonary disease, or impaired or blocked blood circulation Symptoms: Easy to recognize in fair-skinned people because their skin and mucosae take on a bluish cast (become cyanotic) In dark-skinned individuals, this color change can be observed only in the mucosae and nailbeds. Carbon Monoxide Poisoning Type of hypoxia Odorless, colorless gas that competes vigorously with O2 for the same binding sites on hemoglobin Crowds out or displaces O2 (hemoglobin binds to carbon dioxide more readily than to oxygen) Leading cause of death from fire Dangerous because it kills softly and quietly Does not produce the characteristic signs of hypoxia – cyanosis and respiratory distress Instead, the victim becomes confused and has a throbbing headache Neural Regulation of Respiration Activity of respiratory muscles is transmitted to the brain by the phrenic and intercostal nerves Neural centers that control rate and depth are located in the medulla The pons appears to smooth out respiratory rate Normal respiratory rate (eupnea) is 12–15 respirations per minute Hyperpnea is increased respiratory rate often due to extra oxygen needs (exercise) Suppressed Medulla Centers If the medulla centers are completely suppressed, respiration stops completely and death occurs. Can occur with an overdose of sleeping pills, morphine, or alcohol Neural Regulation of Respiration Factors Influencing Respiratory Rate and Depth 1. Physical factors (Increased body temperature, exercise, talking, coughing) 2. Conscious control (during swimming, swallowing, singing) • Voluntary control of breathing is limited and the respiratory centers will ignore messages from our wishes when the O2 supply is getting too low. 3. Emotional factors (Ever been so scared that you gasped or were nearly panting?) Factors Influencing Respiratory Rate and Depth Chemical factors Carbon dioxide levels Level of carbon dioxide in the blood is the main regulatory chemical for respiration Increased carbon dioxide increases respiration Changes in carbon dioxide act directly on the medulla oblongata Factors Influencing Respiratory Rate and Depth Chemical factors (continued) It is the body’s need to rid itself of carbon dioxide (not to take in oxygen) that is the most important stimulus for breathing in a healthy person. Factors Influencing Respiratory Rate and Depth Hyperventilation – A rapid and deep breathing pattern Occurs when carbon dioxide or other sources of acid begin to accumulate in the blood and the pH starts to drop Different breathing pattern from the hyperpnea of exercise This blows off more carbon dioxide, which returns blood pH to normal Hyperventilation When brought on by anxiety attacks, it often leads to brief periods of apnea (cessation of breathing) until the carbon dioxide builds up in the blood again If breathing stops for an extended period of time cyanosis can occur The individual may get dizzy and faint Such attacks can be prevented by having the person breath into a paper bag (raises the CO2 levels in the blood) Factors Influencing Respiratory Rate and Depth Hypoventilation – Extremely slow or shallow breathing Occurs when blood starts to become too basic Allows carbon dioxide to accumulate in the blood and brings blood pH into normal range