43-Hip Joint
advertisement

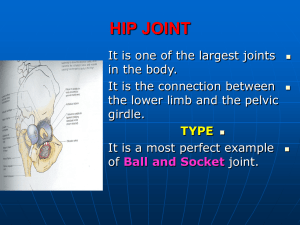
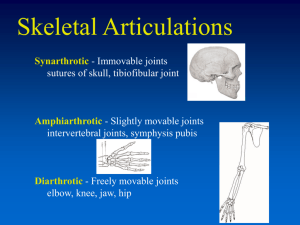
HIP JOINT …..the largest joint in the body Dr. Zeenat Zaidi ARTICULATION Hemispherical head of Femur Cup-shaped acetabulum of the hip bone Articular surfaces covered with hyaline cartilage Head of Femur Globular, more than a hemisphere Directed upward, medially, and a little forward Surface is smooth, covered with hyaline cartilage, except over an ovoid depression, the fovea capitis femoris, which is situated a little below and behind the center of the head The fovea gives attachment to the ligament of the head of femur ACETABULUM Horseshoe shaped articular surface Nonarticular part, acetabular fossa, lodges pad of fat Deepened by fibrocartilaginous rim called acetabular labrum Deficient inferiorly as the acetabular notch that is filled up by transverse acetabular ligament TYPE Synovial A perfect example of a ‘Ball and Socket’ joint CAPSULE • • Encloses the joint Attachment: Medially: Acetabular labrum Laterally: • Anteriorly: to the intertrochanteric line. Some fibers reflect upward along the neck, form ‘retinacula’ (carry blood vessels for head & neck of femur) • Posteriorly halfway along the posterior aspect of neck LIGAMENTS Iliofemoral Pubofemoral Ischiofemoral Transverse acetabular Ligament of head of femur Iliofemoral Ligament o o Strong, Y-shaped Attachment: Base to anterior inferior iliac spine Two limbs to upper & lower ends of intertrochanteric line Prevents over-extension during standing Pubofemoral Ligament o o Triangular in shape Attachment: Base to superior ramus of pubis Apex to lower part of intertrochanteric line Limits extension & abduction Ischiofemoral Ligament o o Spiral in shape Attachment: Medially to the body of the ischium near acetabulum Laterally to the greater trochanter Limits extension Transverse Acetabular Ligament o o Formed by acetabular labrum Bridges acetabular notch, converting it into tunnel through which vessels and nerves enter the joint Ligament of Head of Femur o o o Flat & triangular Attachment: Apex to the pit (fovea) on the head of femur Base to transverse ligament & the margin of acetabulum Intracapsular, ensheathed by synovial membrane Carries articular branch of obturator artery to the joint SYNOVIAL MEMBRANE Lines the capsule Attached to margins of articular surfaces Covers intracapsular part of the neck of femur Ensheaths ligament of head of femur Covers pad of fat in acetabular fossa Protrudes anteriorly through gap between pubofemoral & iliofemoral ligaments and forms psoas bursa RELATIONS Anterior Iliopsoas Inferior Pectineus Rectus femoris Obturator externus Posterior Sciatic nerve Obturator internus Superior & inferior Gemelli Quadratus femoris Superior Gluteus minimus Piriformis BLOOD SUPPLY Head & intra-capsular part of neck receives its blood supply from trochanteric anastomosis, mainly from branches of medial circumflex artery A branch from obturator artery in the ligament of head of femur is importanat in young child NERVE SUPPLY Apply Hilton’s law The nerve supplying a joint also supplies both the: Muscles that move the joint & Skin covering the articular insertion (area of action) of those muscles • Femoral • Obturator • Sciatic • Nerve to quadratus femoris These nerves also supply knee joint & therefore pain arising in the hip joint may be referred to the knee STRENGTH & STABILITY Depends largely on the: Shape of the bones Ligaments MOVEMENTS Wide range (less than shoulder joint) Some movements sacrificed in order to provide strength & stability Movements are: Flexion/Extension Abduction/Adduction Lateral/Medial rotation Circumduction FLEXION Flexors: Iliopsoas Rectus femoris Sartorius Adductor muscles Limitation: with the knee flexed: Anterior surface of thigh coming in contact with the anterior abdominal wall with the knee extended: Tension of hamstring group of muscles EXTENSION Extensors: Gluteus maximus Hamstring muscles Limitation: Tension of iliofemoral, pubofemoral & ischiofemoral ligaments ABDUCTION Abductors: Gluteus medius & minimus Piriformis Sartorius Tensor fascia lata Limitation: Tension of pubofemoral ligament ADDUCTION Adductors: Adductors (longus, brevis & adductor part of magnus) Pectineus Gracilis Limitation: Contact with the opposite limb & by tension in ligament of head of femur LATERAL ROTATION Lateral Rotators: Piriformis Obturator internus & externus Gemilli Quadratus femoris Gluteus maximus Limitation: tension in iliofemoral & pubofemoral ligaments MEDIAL ROTATION Medial Rotators: Anterior fibers of gluteus medius & minimus Tensor fascia lata. Limitation: tension of ischiofemoral ligament. CLINICAL ANATOMY Referred Pain From the Hip Joint The pain originating in the hip joint to be referred to the front and medial side of the thigh (femoral nerve) The hip joint disease may give rise to pain in the knee joint (posterior division of the obturator nerve supplies both the hip and knee joints) Congenital Dislocation Affects 1-2 babies in every 1000 Associated with a shallow acetabulum and an altered angle of the femoral head May be bilateral Females affected more than males May be caused by mechanical factors i.e. malformed uterus The affected limb is shorter than the normal limb • • • • Capsule is loose Upper lip of acetabulum is not developed properly (hypoplasia). Head of femur moves up out of acetabulum and lies against the gluteal surface of ilium. Characteristic clinical sign is the inability to abduct the hip Traumatic Dislocation Rare, because of the strength of joint Occurs when joint is flexed & abducted. This can occur in a car crash where the knee is pushed backwards, often breaking off the posterior rim of the acetabulum • • • • • The head of femur is displaced posteriorly and rests on the gluteal surface of ilium (posterior dislocation). Sciatic nerve is prone to get injured. Lower limb is flexed, adducted & medially rotated and is shorter than the normal limb Positive Trendelenburg’s sign ‘Dipping’ (unilateral dislocation) or ‘waddling’ (bilateral dislocation) gait Osteoarthritis Most common disease of hip joint in the adults Results in: Pain Stiffness (due to pain and reflex spasm of muscles) Deformity i.e. flexion, adduction & external rotation (due to muscle spasm & later on muscle contractures) Arthritis of the Hip Joint A patient with an inflamed hip joint will place the femur in the position that gives minimum discomfort (the position in which the joint cavity has the greatest capacity to contain the increased amount of synovial fluid secreted). The hip joint is partially flexed, abducted, and externally rotated Tenderness over the head of the femur (on the anterior aspect of the thigh just inferior to the inguinal ligament and just lateral to the pulsating femoral artery) usually indicates the presence of arthritis of the hip joint. Thank You & Good Luck