The Morcellation Debate
advertisement

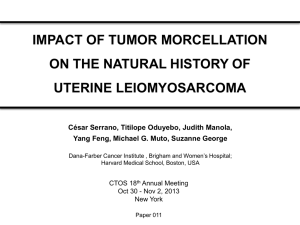
The Morcellation Debate Marisa Adelman, MD Assistant Professor, Dept. Obstetrics & Gynecology The Morcellation Debate (at least we’re not talking about vaginal mesh) Marisa Adelman, MD Assistant Professor, Dept. Obstetrics & Gynecology Talking points: • • • • • • Why now? The respondents: FDA, SGO, ACOG, AAGL The disease and it’s prognosis The affects of morcellation The alternatives Risks vs. Benefits: how does it all shake out? One woman’s opinion… “Always and never are two words you should always remember to never use” - Wendell Johnson We learn through experience…and we get better. The case that started the debate The case that started the debate The SGO weighs in December, 2013 “…the Society of Gynecologic Oncology (SGO) asserts that it is generally contraindicated in the presence of documented or highly suspected malignancy” “The SGO recognizes that currently there is no reliable method to differentiate benign from malignant leiomyomas…Furthermore, these diseases offer an extremely poor prognosis, even when specimens are removed intact.” Nobody likes being called soft “It is difficult to understand why the SGO has taken such a soft line” The Lancet Oncology, February 2014 …especially Barbara Goff (President of the SGO) “In the vast majority of cases, hysterectomy is done because of the presence of benign uterine fibroids. In these circumstances, intracorporial morcellation has benefited hundreds of thousands of women. It is especially beneficial for obese women. It would be a disservice to deny these women this option.” The Lancet Oncology, April 2014 The FDA responds to requests for recall April, 2014 Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. The FDA responds… “Based on an FDA analysis of currently available data, it is estimated that a 1 in 350 women undergoing hysterectomy or myomectomy for the treatment of fibroids is found to have an unsuspected uterine sarcoma” “…because there is no reliable method for predicting whether a woman with fibroids may have a uterine sarcoma, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids.” Why perform minimally invasively? ACOG weighs in… May, 2014 • Approximately 600,000 hysterectomies performed annually in the U.S. • 40% are for the indication of uterine leiomyomas ACOG weighs in… • Preoperative considerations: – Age: • Lowest incidence with age <35 • Highest incidence with age >65 – Menopausal status: • Increased risk of occult malignancy – Uterine size: • Not predictive, but large or rapidly growing leiomyomas may raise concern ACOG weighs in… • Patient counseling and informed consent: – Potential risk of undiagnosed gynecologic cancers • Approximately 2:1000 in women undergoing hysterectomy for uterine fibroids. – If present, power morcellation will increase the risk of intraperitoneal dissemination. • May result in the need for additional surgery and/or medical management. – There is a risk of disseminating and seeding viable ectopic benign tissue. ACOG weighs in… • “There should be a continual focus on training, including techniques for morcellation…” • “There is no sufficiently large population-based series to provide an accurate rate of preoperatively undiagnosed uterine sarcoma in patients undergoing hysterectomy.” • “…a national prospective morcellation surgery registry is needed to acquire an adequate volume of consistent and reliable data.” • “ACOG encourages the FDA to call for the establishment of such a registry. …oh yeah, don’t forget about the AAGL May, 2014 AAGL • “…despite our incomplete understanding of these issues, MIS employing morcellation remains safe when performed by experienced, high-volume surgeons in select patients who have undergone an appropriate preoperative evaluation.” • Studies analyzed by the FDA: – Not stratified by risk factors for sarcoma (esp. age) • Need to consider implications of alternatives AAGL Statement to the FDA on Power Morcellation 4 cautions against discontinuing morcellation 1) 2) 3) 4) “The AAGL cautions against eliminating beneficial technology on the basis of such imprecise data”. “… at this time there exist insufficient data to discontinue power morcellation in appropriately screened patients at low risk”. “The AAGL does not believe that such limited evidence warrants removal of the option of power morcellation”. “… the available data do not warrant discontinuing power morcellation”. Leiomyosarcoma • No reliable preoperative diagnostic tests – Not ultrasound, CT, PET, MRI • 1 in 400 to 1 in 1000 of hysterectomy specimens for presumed benign uterine leiomyoma. – Estimate of 1 in 350 based on 9 studies • All referral-center, single-institution, retrospective studies, with 104-1429 cases. • Spans several decades, with various histopathologic criteria • Includes postmenopausal women, and women diagnosed preoperatively. Prevalence: what are we counting? All-payer database, including more than 500 hospitals. 232,882 MIS hysterectomies (2006-2012) 36,470 morcellations 99 cases of uterine cancer. Prevalence of 27/10,000 (~ 1/368) Prevalence: what are we counting? • There was no distinction made between uterine cancers. • The population was older. Leiomyosarcoma: staging Leiomyosarcoma: staging Leiomyosarcoma: prognosis SEER report, 2007 Stage Location 5-year survival Stage I Confined to the uterus 60% Stage II Confined to the pelvis 35% Stage III Abdominal spread, local nodes 28% Stage IV Bladder, rectum, or distant metastases 15% Leiomyosarcoma: prognosis • Retrospective • Single institution: Asian Medical Center, Seoul, Korea. TAH (31) 77 patients with LMS (1989-2010) 56 w/ early disease (confined to the uterus) Abdominal, vaginal, or laparoscopic morcellation (25) Leiomyosarcoma: prognosis 65% 40% 5-year DFS 53% (all patients) 73% 46% 5-year OS 60% (all patients) Leiomyosarcoma: prognosis • Identified all cases of LMS and STUMP’s from 2005-2012 at Brigham and Women’s, Dana Farber Cancer Institute, and Mass. General Hospital. – 15 with LMS – 5 with STUMP • Assigned a FIGO stage after the initial surgery and restaging surgery. – – – – – 3 LMS upstaged 5 LMS not-upstaged 3 LMS not re-staged 3 LMS unstaged initially 1 LMS was already stage IV initially Leiomyosarcoma: prognosis • Three patients with LMS were upstaged – One stage III stage IV – Two stage I stage III • 2 out of 3 upstaged patients are deceased, and the 3rd is alive with evidence of disease. • 5 of 5 who were not upstaged were alive without evidence of disease at follow-up. Leiomyosarcoma: prognosis • 58 patients with LMS from 2007 to 2012 – 39 patients underwent TAH without morcellation – 19 patients underwent morcellation Leiomyosarcoma: prognosis 10.8 39.6 73% 64% * The mean age was 53.4 years Leiomyosarcoma: prognosis • 1091 cases of uterine morcellation from 2005-2010 for presumed fibroids at BWH. – 10 cases of leiomyoma variants – 2 cases of malignancy (1 endometrial stromal sarcoma, 1 leiomyosarcoma) • 14 cases of follow-up laparoscopy – 7 “in-house” (5 leiomyoma variants, 1 ESS, 1 LMS) – 7 “consults” (1 leiomyoma variant, 6 LMS) Leiomyosarcoma: prognosis • 64.3% occurrence of morcellator-based dissemination. • No definite infiltration or invasion of adjacent tissue. Leiomyosarcoma: prognosis • 4 out of 7 (57.1%) LMS with peritoneal dissemination. – 3 out of 4 with dissemination are deceased (average survival of 24.3 months) – 3 out of 3 without dissemination were alive (average follow-up of 29.7 months) • 4 out of 7 were alive at 24 months (57.1%) Park et al George et al ~90 % ~60% Leiomyosarcoma: prognosis ~60% ~ 25% Assuming early stage disease: • Non-morcellated patients ≈ expected 5 year OS. • Morcellated patients = worse survival (but not quite Stage IV disease) Leiomyosarcoma: prognosis (big picture) • 60% of patients present with disease confined to the uterus. • Local and distant failure rates 45-80%. – 50% recurrence risk after TAH • Long-term survival rates 20-60%, with an overall survival of 40% at 5 years. • Median overall survival of 1-2 years in patients with metastatic disease. Hysterectomy: Complications • Per Cochrane Review: – Decreased rate of abdominal wall or wound infection – Significantly lower EBL – No difference in vaginal cuff cellulitis, hematoma, abscess formation, or GU injury. Hysterectomy: mortality • Retrospective cohort from 2002-2008. – LH patients experienced lower rates of DVT, PE, blood transfusion, MI. – LH patients experienced lower mortality rates (0.01% versus 0.03%, OR 0.48). Informed consent • Per AAGL: – Dissemination of malignant tissue – Dissemination of benign tissue – Difficult or incomplete pathologic evaluation – Injury to adjacent organs Where have all the morcellators gone? • Johnson & Johnson withdrew their morcellators from the market in late July. • Highmark Inc. stopped covering L/S power morcellation on September 1st. Alternatives to morcellation: • • • • • Contained morcellation Vaginal morcellation Colpotomy Minilaparotomy Abdominal hysterectomy Let’s do the numbers (a quick run down) • >600,000 hysterectomies per year • 0.1% mortality rate for LH versus 0.3% for TAH: – 600 deaths if all hysts were laparoscopic – 1,800 deaths if all hysts were abdominal – Excess of 1,200 deaths if all done abdominally. • Using conservative 1/400 risk of leiomyosarcoma: – 1,500 cases • This is an over exaggeration, but you get the point… Let’s do the numbers (a little more scientific) • Decision analysis: treatment of symptomatic fibroids. – Laparoscopic morcellation vs. TAH (not amenable to vaginal removal). • 100,000 subject hypothetical cohort. • 5-year time-line • Outcomes: – Morbidity (transfusion, wound infection, cuff dehiscence, VTE, and hernia) – Death from leiomyosarcoma – Death from TAH. M. Siedhoff, D. Clarke-Pearson. Presented at 2014 AAGL Global Conference. Decision analysis (continued) • Used an estimate of 0.0012 for occult leiomyosarcoma incidence (~1/850). • Estimated death from leiomyosarcoma by laparoscopic and abdominal route. – Assumed occult LMS cases would be FIGO stage III (59% death in 5 years). – Assumed morcellation would escalate staging to FIGO stage III (72% death in 5 years) M. Siedhoff, D. Clarke-Pearson. Presented at 2014 AAGL Global Conference. Decision analysis (continued) Outcome LH AH Leiomyosarcoma cases 120 120 Leiomyosarcoma deaths 86 71 Hysterectomy-related deaths 12 32 98/100,000 103/100,000 Total deaths • 5 additional deaths per 100,000 with AH. • Lower mortality and higher QOL with LH. M. Siedhoff, D. Clarke-Pearson. Presented at 2014 AAGL Global Conference. Conclusions The debate is not: • Is morcellation of a leiomyosarcoma associated with a worse outcome? What we should be asking: • What do we stand to loose by abandoning morcellation? • How do we make it more safe? Parting words (I guess it is kind of like vaginal mesh) References • SGO (Society of Gynecologic Oncology) position statement: morcellation. Available at: https://www.sgo.org/newsroom/position-statements2/morcellation/ • The Lancet Oncology. Patient safety must be a priority in all aspects of care. Lancet Oncol 2014; 15:123. • Goff BA. SGO not soft on morcellation: risks and benefits must be weighed. Lancet Oncol 2014; 15:e148. • Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. Available at: http://www.fda.gov/medicaldevices/safety/alertsandnotices/ucm3 93576.htm. References • American College of Obstetricians and Gynecologists. Power morcellation and occult malignancy in gynecologic surgery. Washington, DC: American College of Obstetricians and Gynecologists; 2014. • Hodgson B. AAGL Practice Report: Morcellation During Uterine Tissue Extraction. J Minim Invasive Gynecol 2014; 21:517-30. • Wright JD et al. Uterine pathology in women undergoing minimally invasive hysterectomy using morcellation. JAMA 2014; 312:1253-55. • Zivanovic O et al. Stage-specific outcomes of patients with uterine leiomyosarcoma: A comparison of the International Federation of Gynecology and Obstetrics and American Joint Committee on Cancer Staging Systems. J Clin Oncol 2009; 27:2066-72. References • Park JY et al. The impact of tumor morcellation during surgery on the prognosis of patients with apparently early stage uterine leiomyosarcoma. Gynecol Oncol 2011; 122:255-9. • Oduyebo T et al. The value of re-exploration in patients with inadvertently morcellated uterine sarcoma. Gynecol Oncol 2014; 132:360-5. • George S et al. Retrospective cohort study evaluating the impact of intraperitoneal morcellation on outcomes of localized uterine leiomyosarcoma. Cancer 2014; 120:3154-8. • Seidman MA et al. Peritoneal dissemination complicating morcellation of uterine mesenchymal neoplasms. PLOS 2012;7:e50058. References • Clark-Pearson DL, Geller EJ. Complications of hysterectomy. Obstet Gynecol 2013; 121:654-73. • Wiser A et al. Abdominal versus laparoscopic hysterectomies for benign diseases: evaluation of morbidity and mortality among 465,798 cases. Gynecol Surg 2013; 10:117-22. • Kho KA, Nezhat CH. Evaluating the risks of electric uterine morcellation. JAMA 2014; 311:905-6. • Johnson & Johnson suspends sale of device used in fibroid surgery: Wall Street Journal. Available at:http://onlinewsj.com/news/articles. References • Cortez, Michelle F. “Device recall means tougher surgeries.” The Philadelphia Inquirer [Philadelphia] 11 Aug. 2014: A2. Print.