Atherosclerosis
advertisement

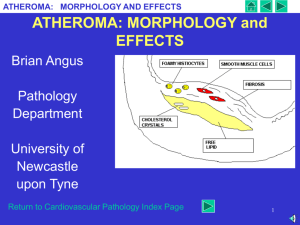
ATHEROSCLEROSIS DR.SAMINA QAMAR ASSISTANT PROFESSOR HISTOPATHOLOGY. Athero-sclerosis • The atheroma ("lump of gruel", from Greek (athera), meaning "gruel" OR Porridge. • Sclerosis means thickening. • Atherosclerosis (also known as arteriosclerotic vascular disease or ASVD) is a specific form of arteriosclerosis in which an arterial wall thickens as a result of invasion and accumulation of white blood cells . Arterioscelorosis Also called fatty streaks/plaques. • Early on, Atheromas are called "fatty streaks“ because of yellow appearance due to collection of foam cells: fat containing macrophages. • Later on the grumous core of lipid is covered by a white fibrous cap and then its called an atheroma. Fatty streaks can appear in the aortas of infants younger than 1 year and are present in virtually all children older than 10 years. Wall of artery showing fatty streaks/plaques. Arteriosclerosis: Fatty streaks Artery wall histology. NORMAL ARTERY WALL ARTERIOSCLEROTIC ARTERY WALL What are the results of atherosclerosis? • These changes reduce the elasticity of the arterial wall but do not affect blood flow for decades because the muscular wall of artery enlarges at the locations of plaque. • Atherosclerotic lesions can cause thromboembolism and complete closure of the lumen of a small blood vessel. Consequences • Atheroma can suddenly rupture, causing the formation of a thrombus that will rapidly slow or stop blood flow, leading to death of the tissues fed by the artery in approximately 5 minutes. • If artery of heart is blocked it can cause a heart attack. The same process in an artery to the brain is commonly called stroke. Consequences. Why it starts? • • • • RISK FACTORS: OLD AGE. MALE GENDER. POST MENOPAUSAL ESTROGEN DEFICIENCY. RISK FACTORS • • • • • • HYPERLIPIDEMIA(LDL). HYPERTENSION. OBESITY. CIGARETTE SMOKING. SEDENTRY LIFE STYLE. DIABETES. HOW IT STARTS? Response-to-injury hypothesis • This model views atherosclerosis as a chronic inflammatory response of the arterial wall to endothelial injury. • Hemodynamic disturbances, toxins and hypercholesterolemia. Participants • T-lymphocytes, monocytes/ • Macrophages and normal constituents of arterial wall. PATHOGENESIS. 1-After endothelial injury monocytes cluster beneath endothelium. 2-Macrophages,foam cells and platelets also accumulate. 3- They start engulfing lipid intracellulary. 4- SMC and collagen are deposited. 5-Extracellular lipid is released How do they appear grossly? • Atheromatous plaques grossly appear white to yellow. • Thrombosis superimposed over the surface of ulcerated plaques is red-brown in color. • Plaques vary from 0.3 to 1.5 cm in diameter but can coalesce to form larger masses AS • Mild AS : scattered lipid plaques. • Middle: shows many more larger plaques. • The severe atherosclerosis in the aorta at the top shows extensive ulceration in the plaques. PLAQUES: C,E,L. • Atherosclerotic plaques have three principal components: • (1)Cells: SMCs, macrophages, and T cells. • (2)ECM: collagen, elastic fibers, and proteoglycans. • (3)Lipid: intracellular and extracellular. Atheroma is composed of Atheroma. Atheroma • Superficial fibrous cap is composed of SMCs and relatively dense collagen. Beneath and to the side of the cap (the "shoulder") is a more cellular area containing macrophages, T cells, and SMCs. • Deep to the fibrous cap is a necrotic core, containing lipid (primarily cholesterol and cholesterol esters), debris from dead cells, foam cells (lipid-laden macrophages and SMCs), fibrin, plasma proteins and the cholesterol that appears as clefts. Histology of plaque. • Atheroma on the left. Cholesterol clefts are numerous in this atheroma. The surface on the far left shows ulceration and hemorrhage.