PCRRT Congress
London 2015
My Approach to Oliguria
Joseph A Carcillo MD
University of Pittsburgh
Why do I worry about oliguria?
•
•
•
•
What is oliguria?
Is it below 1.7 mL/kg/hr?
Is it below 0.5 mL/kg/hr?
Is it urine output less than total input – other
losses?
Hospital mortality according to UO ranges.
Candice Torres de Melo Bezerra et al. Nephrol. Dial.
Transplant. 2013;28:901-909
© The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA. All rights
reserved.
From: Early Volume Expansion During Diarrhea and Relative Nephroprotection During Subsequent Hemolytic
Uremic Syndrome
Arch Pediatr Adolesc Med. 2011;165(10):884-889. doi:10.1001/archpediatrics.2011.152
Date of download: 6/27/2015
Copyright © 2015 American Medical
Association. All rights reserved.
Cumulative patient survival between patients with normal and reduced UO.
Candice Torres de Melo Bezerra et al. Nephrol. Dial.
Transplant. 2013;28:901-909
© The Author 2013. Published by Oxford University Press on behalf of ERA-EDTA. All rights
reserved.
Modified RIFLE criteria for pediatric patients (pRIFLE)
eCCL, Estimated creatinine clearance; pRIFLE, risk, injury, failure, loss, and
end-stage renal disease in children
RIFLE criteria
Estimated CCL
Urine output
Risk (of renal dysfunction)
eCCL decrease by 25 %
<0.5 ml/(kg h) for 8 h
Injury (to the kidney)
eCCL decrease by 50 %
<0.5 ml/(kg h) for 16 h
eCCL decrease by 75 % or
<0.5 ml/(kg h) for 24 h or
anuric for 12 h
Failure (of kidney function)
eCCL <35 ml/min/1.73 m2
Loss (of kidney function)
Persistent failure >4 weeks
End-stage (kidney disease)
End-stage renal disease
(persistent failure >3
months)
Nilzete Bresolin1, 4 , Aline Patrícia Bianchini2 and Clarissa Alberton Haas3
Pediatric acute kidney injury assessed by pRIFLE as a prognostic factor in the
intensive care unit Pediatric Nephrology Journal of the International Pediatric
Nephrology Association 201228:2357 DOI: 10.1007/s00467-012-2357-8
Fluid Overload at 48 Hours Is
Associated With Respiratory
Morbidity but Not Mortality in a
General PICU: Retrospective Cohort
Study*.
Sinitsky, Lynn; MB, MRCPCH; Walls,
David; Nadel, Simon; MB, FRCP;
Inwald, David; FRCPCH, PhD
Pediatric Critical Care Medicine.
16(3):205-209, March 2015.
DOI:0.1097/PCC.0000000000000318
Figure 1 . Duration of ventilation in survivors according to different levels of fluid overload at 48 hr
from admission. Medians and interquartile range are shown. The relationship between fluid overload
percent and invasive ventilation days in survivors was significant, despite the wide interquartile range
(Kruskal-Wallis test, p < 0.001).
©2015The Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care
Societies. Published by Lippincott Williams & Wilkins, Inc.
4
Fluid Overload at 48 Hours Is Associated With Respiratory Morbidity but Not Mortality in a General
PICU: Retrospective Cohort Study*
.
Sinitsky, Lynn; MB, MRCPCH; Walls, David; Nadel, Simon; MB, FRCP; Inwald, David; FRCPCH, PhD
Pediatric Critical Care Medicine. 16(3):205-209, March 2015.
DOI: 10.1097/PCC.0000000000000318
©2015The Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care
Societies. Published by Lippincott Williams & Wilkins, Inc.
5
Figure 1 Mortality rates of pediatric intensive care unit patients receiving continuous renal
replacement therapy subdivided by degree of fluid overload. Error bars represent 95%
confidence intervals for the mortality rate in each fluid overload group..
Scott M. Sutherland , Michael Zappitelli , Steven R. Alexander , Annabelle N. Chua , Patrick
D. Brophy , Timothy E.Bunchman
Fluid Overload and Mortality in Children Receiving Continuous Renal Replacement
Therapy: The Prospective Pediatric Continuous Renal Replacement Therapy Registry
American Journal of Kidney Diseases, Volume 55, Issue 2, 2010, 316 - 325
Fluid restriction Yay or Nay?
• All mechanically ventilated PICU patients with
respiratory distress have oliguria
• Limit intravenous maintenance fluid to
’ventilator maintenance’ or 2/3 maintenance
• Concentrate non-maintenance fluids and give
maintenance fluids through the enteral tract
• I do not restrict fluids because it could induce
renal injury – here is the evolving HUS story
Timing of critical events during illness.
Julie A. Ake et al. Pediatrics 2005;115:e673-e680
©2005 by American Academy of Pediatrics
Volume and characteristics of fluids that were administered during first 4 days of illness.
Julie A. Ake et al. Pediatrics 2005;115:e673-e680
©2005 by American Academy of Pediatrics
From: Early Volume Expansion During Diarrhea and Relative Nephroprotection During Subsequent Hemolytic
Uremic Syndrome
Arch Pediatr Adolesc Med. 2011;165(10):884-889. doi:10.1001/archpediatrics.2011.152
Date of download: 6/27/2015
Copyright © 2015 American Medical
Association. All rights reserved.
From: Early Volume Expansion During Diarrhea and Relative Nephroprotection During Subsequent Hemolytic
Uremic Syndrome
Arch Pediatr Adolesc Med. 2011;165(10):884-889. doi:10.1001/archpediatrics.2011.152
Date of download: 6/27/2015
Copyright © 2015 American Medical
Association. All rights reserved.
Appropriate Oliguria – Prerenal Response
Rule out appropriate oliguria
1) ‘Outs’ much greater than ‘ins’ due to other
losses (DKA, Diarrhea, DI etc), increased
urine specific gravity or glucose
2) Hypoalbuminemia with hypoproteinemia
leading to low oncotic pressure
Acute Pathologic Oliguria
1) SIADH – high urine sodium, positive fluid
balance
2) Preglomerular vasoconstriction
3) Increased intra-abdominal pressure
Reduced Renal Perfusion
MAP - IAP or MAP - CVP
Palmer BF, Fenves AZ. Optimizing blood pressure control in patients with
chronic kidney disease. Proc (Bayl Univ Med Cent). 2010 Jul;23(3):239-45.
Urine
output
(mL/kg/hr)
Basal
Day 1
Day 2
Day 3
Day 4
NE-group
4.3±2.9
4.7±1.7
5.1±1.7
4.9±1.5
4.5±1.2
Placebogroup
3.5±2.2
3.9±1.6
3.8±1.0
4.1±1.5
4.5±1.5
* 0.016
Jefferson Piva1, Tamila Alquati2, Pedro Celiny Garcia23, Humberto Fiori23, Paulo
Einloft23, Francisco Bruno23 Norepinephrine infusion increases urine output in children
under sedative and analgesic infusion. Rev. Assoc. Med. Bras. [online]. 2014, vol.60, n.3,
pp. 208-215. ISSN 0104-4230.
No.
%
Mechanical ventilation
26
100
Inotropic or vasopressor support
22
85
Dialysis
8
31
ECMO
3
12
Preoperative cardiac arrest
11
42
Leukocytosis (WCC > 11 × 109 cells/L)
16
67
Leukopenia (WCC < 4 × 109 cells/L)
5
21
Mean preoperative bladder pressure, mm Hg
(range)
26 (12-44)
Mean preoperative lactate, mg/dL (range)
8.6 (1.5-22)
Oliguria
26
Preoperative support
Preoperative variables
100
Pearson EG1, Rollins MD, Vogler SA, Mills MK, Lehman EL, Jacques E, Barnhart DC, Scaife ER,
Meyers RL. J Pediatr Surg. Decompressive laparotomy for abdominal compartment
syndrome in children: before it is too late. 2010 Jun;45(6):1324-9. doi:
10.1016/j.jpedsurg.2010.02.107.
Chronic Pathologic Oliguria
1) Low Cardiac Output
2) Liver Failure
3) Nephrotic Syndrome
Sequential Nephron Blockade Breaks
Resistance to Diuretics in Edematous
States. Knauf, H; Mutschler, E
Journal of Cardiovascular Pharmacology.
29(3):367-372, March 1997.
FIG. 4 . Top: Pathogenesis of sodium retention in
edematous diseases modified after Schrier (8) and Seldin
(9). EABV, effective arterial blood volume; RAA system,
renin-angiotensin-aldosterone system; GFR, glomerular
filtration rate; RPF, renal plasma flow; FF, filtration
fraction; ADH, antidiuretic hormone. Bottom: Relation
between urinary delivery of diuretic and natriuretic
response in normal controls, in patients with chronic renal
failure, and in edematous states with reduced effective
arterial blood volume (EABV). To be independent of
individual GFRs, urinary diuretic excretion ([mu]g/min) is
divided by each patient's GFR (ml/min) yielding fractional
diuretic excretion [mu]g/ml) corresponding to tubular
disposition of the diuretic. Natriuretic response is given by
fractional Na+ excretion. The "plateau" of the curve
represents the intrinsic activity of the diuretic in the
respective diseases. This, in turn, is set by the Na+ load at
the tubular site of the diuretic's action. Schematically
modified after refs. 30, 31, 33, and 34.
© Lippincott-Raven Publishers. Published by Lippincott Williams & Wilkins, Inc.
6
Figure 1 Diuretic Resistance and the Nephron Sites of diuretic action and sodium retention with suggested strategies to overcome
diuretic resistance. Sodium delivery into tubular fluid is determined by glomerular filtration rate (GFR). Percentage of filte...
Jacob C. Jentzer , Tracy A. DeWald , Adrian F. Hernandez
Combination of Loop Diuretics With Thiazide-Type Diuretics in Heart Failure
Journal of the American College of Cardiology, Volume 56, Issue 19, 2010, 1527 - 1534
http://dx.doi.org/10.1016/j.jacc.2010.06.034
Sequential Nephron Blockade Breaks Resistance to
Diuretics in Edematous States.
Knauf, H; Mutschler, E
Journal of Cardiovascular Pharmacology. 29(3):367372, March 1997.
FIG. 2 . Left: Sodium excretion per day after the
administration of 50 mg hydrochlorothiazide (HCTZ)
in relation to the patients' pretreatment fractional
sodium excretion, FENa+. Right: The increment of
sodium excretion achieved by acetazolamide, 250
mg, coadministered with 25 mg HCTZ in relation to
the patients' pretreatment FENa+. Co, healthy
controls.
© Lippincott-Raven Publishers. Published by Lippincott Williams & Wilkins, Inc.
4
Sequential Nephron Blockade Breaks Resistance to
Diuretics in Edematous States.
Knauf, H; Mutschler, E
Journal of Cardiovascular Pharmacology. 29(3):367372, March 1997.
FIG. 3 . The same experiment as depicted in Fig. 2.
Instead of hydrochlorothiazide (HCTZ), furosemide
(FU) is administered. Left: 80 mg FU. Right: 40 mg FU
and 250 mg acetazolamide (AA).
© Lippincott-Raven Publishers. Published by Lippincott Williams & Wilkins, Inc.
5
Sequential Nephron Blockade Breaks Resistance to
Diuretics in Edematous States.
Knauf, H; Mutschler, E
Journal of Cardiovascular Pharmacology. 29(3):367-372,
March 1997.
FIG. 1 . Sodium excretion per day after the administration
of hydrochlorothiazide (HCTZ), furosemide (FU), and
acetazolamide (AA) compared with pretreatment data
(pre) [on "basic" spironolactone (100 mg/day) treatment
throughout the study] in congestive heart failure, liver
cirrhosis with ascites, and nephrotic syndrome. In the
headline, the excretion data of healthy controls are given.
© Lippincott-Raven Publishers. Published by Lippincott Williams & Wilkins, Inc.
3
Who would argue with using CRRT
for renal failure? NOT ME
I would argue that attention to fluid
balance and diuretic therapy before
going to CRRT is worthwhile.
Goal = < 10% total body water fluid
overload
Figure 2. Kaplan-Meier
curves for time to
worsening of the SepsisRelated Organ Failure
Assessment (SOFA) score.
The hemofiltration (HF)
group showed a more
rapid deterioration
compared with the
control (C) group (logrank test: [chi]2 = 8.73; p
< 0.01).
Impact of continuous venovenous hemofiltration on organ failure during the early phase of severe sepsis: A
randomized controlled trial *.
Payen, Didier; MD, PhD; Mateo, Joaquim; Cavaillon, Jean; Fraisse, Francois; Floriot, Christian; Vicaut, Eric; MD, PhD
Critical Care Medicine. 37(3):803-810, March 2009.
DOI: 10.1097/CCM.0b013e3181962316
7
Figure 3. Kaplan-Meier
curves for time to death
during the observation
period (14 days). Log-rank
test: [chi]2 = 2.638; p =
0.104. C, control; HF,
hemofiltration.
Impact of continuous
venovenous hemofiltration on
organ failure during the early
phase of severe sepsis: A
randomized controlled trial *.
Payen, Didier; MD, PhD; Mateo,
Joaquim; Cavaillon, Jean;
Fraisse, Francois; Floriot,
Christian; Vicaut, Eric; MD, PhD
Critical Care Medicine.
37(3):803-810, March 2009.
DOI:
10.1097/CCM.0b013e31819623
16
© 2009 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams
& Wilkins, Inc.
8
Figure 4. A, Kaplan-Meier curves for
time to weaning from mechanical
ventilation. Weaning took a
significantly longer time in the
hemofiltration (HF) group (log-rank
test: [chi]2 = 4.19; p = 0.04). B,
Kaplan-Meier curves for time to
weaning of catecholamines. Time to
weaning was significantly longer in
the HF group (log-rank test [chi]2 =
3.9; p = 0.048). C, control.
Impact of continuous venovenous
hemofiltration on organ failure
during the early phase of severe
sepsis: A randomized controlled
trial *.
Payen, Didier; MD, PhD; Mateo,
Joaquim; Cavaillon, Jean; Fraisse,
Francois; Floriot, Christian; Vicaut,
Eric; MD, PhD
Critical Care Medicine. 37(3):803810, March 2009.
DOI:
10.1097/CCM.0b013e3181962316
© 2009 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams
& Wilkins, Inc.
9
ADEQUATE
PERFUSION
PRESSURE
SEQUENTIAL DIURETIC BLOCKADE
Dopexamine
MAP – CVP
Amiloride
Metalozone
MAP– IAP
Aminophylline
1 mg/kg q 6 hours
Continuous Furosemide infusion
0.04 -0.16 mg /kg /h
INCREASED
DIURESIS
Hydrochlorothiazide
5-10 mg/kg q 12 hours
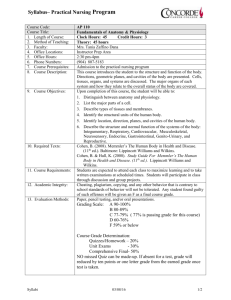
Fig. 2 Forest plot displaying the effect of continuous vs intermittent (bolus) loop diuretic
infusion on daily (A) or hourly (B) urine output in trials of adults and daily (C) urine output in
trials of children.
Fahad Alqahtani , Ioannis Koulouridis , Paweena Susantitaphong , Khagendra Dahal , Bertrand L. Jaber
A meta-analysis of continuous vs intermittent infusion of loop diuretics in hospitalized patients
Journal of Critical Care, Volume 29, Issue 1, 2014, 10 - 17
http://dx.doi.org/10.1016/j.jcrc.2013.03.015
Aminophylline in the treatment
of fluid overload.
Pretzlaff, Robert; Vardis, Ralph;
Pollack, Murray; MD, FCCM
Critical Care Medicine.
27(12):2782-2785, December
1999.
Figure 3 . Change in urine output.
Data presented represent the
mean percent changes in urine
output after administration of the
aminophylline bolus compared
with baseline values.
© 1999 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.
5
Surviving Sepsis Campaign Renal
Replacement Therapy Recommendations
Adult Recommendations
1.We suggest that continuous renal replacement therapies
and intermittent hemodialysis are equivalent in patients
with severe sepsis and renal failure (grade 2B)
2.We suggest the use of continuous therapies to facilitate
management of fluid balance in hemodynamically unstable
septic patients(grade 2D)
Pediatric Recommendations
1. We suggest the use of diuretics to reverse fluid overload
when shock has resolved and if unsuccessful, then
continuous veno venous hemofiltration or intermittent
dialysis to prevent greater than 10% total body weight fluid
overload (grade 2C)
My Approach to Oliguria
My Goal is Even Fluid Balance!
•
•
•
•
•
•
2/3 ventilator maintenance fluid
Enteral maintenance rather than parenteral
Replace fluid losses, maintain oncotic pressure
Maintain adequate MAP-CVP or MAP-IAP
Sequential blockade diuretic therapy
CVVH