Hypertension
advertisement

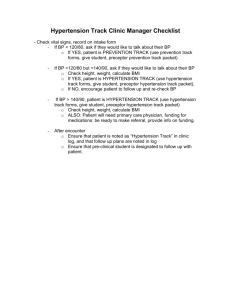
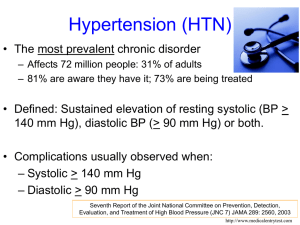
Hypertension Robin Felker Bloomer Hill-NCSRHC September 16, 2009 Outline Epidemiology of HTN Clinical Presentation Interventions Symptoms BP measurement and interpretation Behavior Modification Drugs Comorbitities and Complications HTN at Bloomer Hill Epidemiology Epidemiology Hypertension is the most common primary diagnosis in US (PDx in 35 million office visits) Framingham Heart Study suggests that individuals who are normotensive at age 55 have a 90 percent lifetime risk for developing hypertension In Stage I HTN, achieving a sustained 12 mmHg reduction in SBP over 10 years will prevent 1 death for every 11 patients treated If CVD or organ damage, only 9 patients would require such BP reduction to prevent a death Epidemiology Age-adjusted prevalence of hypertension is significantly higher among blacks (39%) than among whites (29%) Racial disparity in SBP control contributes to nearly 8,000 excess deaths annually from heart disease and stroke among blacks Hypertension is the single largest contributor, of any medical condition, to racial disparity in adult mortality Identifying HTN in the Clinic Clinical Symptoms Commonly ASYMPTOMATIC! “Classic Sx”: Headache, epistaxis, dizziness No more frequent in HT than non-HT patients Flushing, sweating, blurred vision Family history (first degree relatives) Manifestations of organ damage Will discuss later Natural History Essential Hypertension (95% of cases) Chronic Renal Disease (2-4%) Age of onset: 20-50 years Family history of hypertension (1st degree relatives) Gradual onset, mild-to-moderate BP Normal serum K+, urinalysis Increased creatinine, abnormal urinalysis Primary aldosteronism (1-2%) Decreased serum K+ Proper BP measurement Persons should be seated quietly for at least 5 minutes in a chair (rather than on an exam table), with feet on the floor, and arm supported at heart level Need an appropriate-sized cuff (cuff bladder encircling at least 80 percent of the arm) Release air so needle falls 2-3 mmHg/sec Be wary of stress, discomfort, and other evidence of “White Coat HTN” Need elevated HTN on 2 separate occasions Things to think about Ideal PE should include BP confirmation, with verification in the contralateral arm Examination of the optic fundi Body mass index(BMI)/waist circumference Auscultation for carotid, abdominal, and femoral bruits Palpation of the thyroid gland Thorough examination of the heart and lungs Examination of the abdomen for enlarged kidneys, masses, and abnormal aortic pulsation Palpation of the lower extremities for edema and pulses Neurological assessment Things to think about Laboratory tests Urinalysis and serum Cr/BUN (rule out renal disease) Serum potassium (aldosteronism) Blood glucose level (diabetes strongly linked to HTN and renal disease) Serum Cholesterol (global vascular screen) ECG (to monitor for LVH) Interpreting Blood Pressure HTN Interventions Interventions Goal of treatment is to reduce cardiovascular and renal morbidity and mortality A combination of lifestyle modifications and drug therapy are recommended REMEMBER: The most effective therapy prescribed by the most careful clinician will control hypertension only if patients are motivated Behavior Modifications Lifestyle modifications are recommended even for those with near normal BP: ≥ 120/80 Eight modifications are recommended by the AHA: Eat a better diet, which may include reducing salt Enjoy regular physical activity Maintain a healthy weight Manage stress Avoid tobacco smoke Understand hot tub safety Comply with medication prescriptions If you drink, limit alcohol = Cardiac disease, renal & diabetes Drugs (on the $4 list…) Diuretics ACEI Atenolol, Bisoprolol, Carvedilol, Metoprolol, Naldolol, Pindolol, Propranolol, Sotalol CCB Lisinopril, Enalapril, Captopril, Benazepril ARB BB Hydrochlorothiazide (HCTZ) and Chlorthalidone Thiazide-like diuretics have been shown to be best first-line treatment Diltiazem, verapamil Most patients will need at least 2 drugs to achieve BP goals Combos: Lisinopril-HCTZ, Enalopril-HCTZ, Atenolol-Chlorthalidone, Comorbidities and Complications Comorbidities: Obesity BMI >30 is an increasingly prevalent risk factor for the development of hypertension and CVD Intensive lifestyle modification should be pursued in these individuals Consider drug treatment for components of metabolic syndrome Obesity, glucose intolerance, high BP, high TGs, low HDL Comorbidities : Diabetes Target of <130/80 mmHg Thiazide diuretics, BBs, ACEIs, ARBs, and CCBs are beneficial in reducing CVD and stroke incidence in diabetics ACEI- or ARB-based treatments favorably affect the progression of diabetic nephropathy and reduce albuminuria Old Age Hypertension occurs in more than two-thirds of individuals after age 65 However, this group has worst BP control Lower initial drug doses may be indicated to avoid symptoms But, standard recommendations should apply Tx in Women Oral contraceptives may increase BP Risk of hypertension increases with duration of use Women taking oral contraceptives should have their BP checked regularly Development of hypertension is a reason to consider other forms of contraception Tx in Minorities Impact of hypertension are increased in African Americans African-Americans develop high blood pressure at younger ages than other groups in the U.S. Complications are more likely to develop with high blood pressure, including stroke, kidney disease, blindness, dementia, and heart disease Reduced BP responses to monotherapy with BBs, ACEIs, or ARBs; want to include diuretic in treatment! Differences in adherence by race may be due to affordability of medicines, personal beliefs, anticipated adverse effects, and health BP control is lowest in Mexican American and Native American populations Target organ damage Heart Heart failure Brain Left ventricular hypertrophy Angina or prior myocardial infarction Prior coronary revascularization Stroke or transient ischemic attack Chronic kidney disease Peripheral arterial disease Retinopathy Take Home Points Hypertension is a VERY common medical condition Lifestyle modifications should start even in persons with near-normal BP (≥120/80) Proper BP interventions include lifestyle modifications and drug interventions Proper identification and treatment is essential to preventing CHF and target organ damage Two-drug therapy may be necessary for control First line control is usually thiazide-like diuretic Tx of BP with comorbidities must take into account concurrent treatment of comorbid conditions HTN at Bloomer Hill It is essential to follow BP trends and address HTN in our patients If someone has a high reading, ask about caffeine/smoking, have them sit for 5 mins and recheck BP in the exam room Try for repeat visit in anyone with high BP, especially >140/90 Follow-up: every 6 months for well-controlled, monthly/bimonthly if uncontrolled, monthly with med changes Counseling on lifestyle modifications for almost every patient is warranted! Try for discrete goals that the patient is on-board with and document them for follow-up References Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7 Express). Drugs for hypertension. Treatment Guidelines from the Medical Letter 2009; 7(77). http://medletbest.securesites.com.libproxy.lib.unc.edu/restrictedtg/t77.html Fiscella K, Holt K. Racial disparity in hypertension control: tallying the death toll. Ann Fam Med 2008;6:497-502. Lilly. Pathophysiology of Heart Disease, ed 4. http://www.webmd.com/hypertension-high-bloodpressure/hypertension-in-african-americans