Five Star Raing System Explained
advertisement

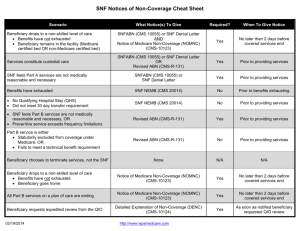
Measuring Quality in a SNF for Medical Directors 5 Star Rating System Quality Reporting Program Value Based Purchasing Judy Wilhide Brandt, RN, BA, RAC-MT, C-NE judy@judywilhide.com 909-800-9124 www. JudyWilhide.com Five Star Rating System • Tool created by CMS in 2008 to help consumers select and compare skilled nursing care centers. • Uses information from Health Care Surveys (standard, focus and complaint), Quality Measures, and Staffing • CMS intends to move to a five star-rating system for all of its "Compare" sites, "with a goal of full transition to star ratings by 2016,” – This will include hospitals. Nursing Home Compare & Five Star Rating System Review Actual Survey Reports (redacted for HIPPA) Details each citation with state and national average citations Staffing PT staff hours do not count in rating. Short Stay Long Stay New/worsen ed PrU Hi Risk PrU New Antipsychotic Antipsychotic Use Self Report Mod/Severe Pain Self Report Mod/Severe Pain Long Stay Fall Major Injury Restraint Use Lo risk Incontinence Weight loss Flu Vaccine UTI Depressive symptoms Pneumovax Catheter Pneumovax ADL Decline NH Compare Quality Measures Flu Vaccine Special Focus Facilities: (a) have had a history of serious quality issues and (b) are included in a special program to stimulate improvements in their quality of care. 2/23/15 Virginia North Carolina Florida New York Times 8/24/14 • Receiving a high star rating has never been more important to nursing homes. – Hospitals often use star ratings in referral decisions – Insurers consider them when setting up preferred networks – Often a first stop for investors and lenders, who consult them to decide whether a nursing home company is a safe bet. – Many bundled payment projects require at least 3 stars Five Star Rating System Details Survey ★ 3 years Annual 36 months complaint Staffing ★ +1 for 4 or 5 stars if above survey stars -1 for 1 Star Quality Measures ★ +1 for 5 stars -1 for 1 Star Overall Star Rating ★ You Shall Rise and Show Respect to the Aged Example: Overall Happy Valley ★★ Survey Staffing ★ QM ★★★★ ★★★★★ Peaceful ★★ ★★ ★★ ★★★★ Place Rocking ★★★ ★★★★ ★★★★ Retirement ★★★★ Swinging ★★★★★ ★★★ ★★★★ ★★★★★ City Terminal ★★ ★★★★ ★ Towers ★ Quintile definition: divided into five equal groups, based on performance Best Second best Third best (or third worst) Next to worst Worst Each Domain Divides all NFs into quintiles • All domains use different methods • End result: assignment of 1-5 stars overall ★★★★★ ★★★★ ★★★ ★★ ★ Much above average Above average Average Below average Much below average These quintiles are not always equally divided. Survey Domain • Comparison for survey stars is intra-state – Accounts for different types of surveys and different approaches to the survey process among states • Deficiencies are assigned points based on scope and severity • All NFs in a state are lined up from best to worst and split into quintiles – Top 10% = 5 stars – Bottom 20% = 1 star • Line-up and rating are based on intrastate comparisons – Survey agencies and processes vary widely across the country. Intra State Survey Comparisons 8.3 Virginia 3.7 North Carolina 5.3 Kentucky 7.3 Illinois Average number of citations 2/23/15 US Average: 6.8 Complaint Survey Weights 1/6 1/2 1/3 Revisits to Clear Revisit Number Noncompliance Points First 0 Second 50% of survey score added on Third 70% of survey score added on Fourth 85% of survey score added on CMS experience is that providers that fail to demonstrate restored compliance with safety and quality of care requirements during the first revisit have lower quality of care than other nursing homes. More revisits are associated with more serious quality problems. You Shall Rise and Show Respect to the Aged Intra-State Considerations Since it’s all a ‘quintile system based on what percentage did the best and worst, there is a wide variation between states in what the raw survey score number translates to. 20% 23.3 23.3 23.3 Cut point table posted every month. The month your survey is calculated, they use this table to see how many stars to give you. Then your stars are fixed until you get another survey. 10% Staffing • • Considerable evidence of a relationship between nursing home staffing levels and resident outcomes. Staffing Study found a clear association between nurse staffing ratios and nursing home quality of care, identifying specific ratios of staff to residents below which residents are at substantially higher risk of quality problems. You Shall Rise and Show Respect to the Aged Staffing based on two case-mix adjusted measures, with equal weight. Total Nurse RN Staffing Details • Not a valid/reliable way to verify staffing adequacy • Facility reports staff hours worked in the last full two week pay period that ends closest to day 1 of the survey • Census is from day 1 of survey • Acuity is from end of last quarter closest to da 1 of survey – Based on RUG scores Illustration: Q1 Q2 Q3 Target Date Jun 29 Q1 RUG Data Survey Date July 6 No RUG Data for Q2 yet Staffing Stars assigned Q4 Census Some time in the future: Q1 Q2 Q3 Target Date Jun 29 Survey Date July 6 Q4 Census Q2 RUG Available Staffing Stars assigned New Staffing Stars assigned Doing the math Hoursadjusted = (Hoursreported/Hoursexpected)*HoursNational average Total Nurse Example 3 reported/ 6 expected = ½ x 4.0309 = 2.0154 adjusted hours National Average Hours per Resident Day Calculated April 2012 Total Nurse: 4.0309 RN: 0.7472 You Shall Rise and Show Respect to the Aged Five Star Quality Measures The measures were selected based on their validity and reliability, the extent to which facility practice may affect the measure, statistical performance, and importance. Three quarters of MDS data is averaged SNFs are assigned stars based on comparative data with other SNFs 5 Star Quality Measures 8 long stay (over 100 CDIF) • ADL decline (Bed mob, toilet, transfer, eating) • High-risk residents with pressure ulcers (St 2, 3 and 4 only) • Indwelling catheter (exclusions: Neurogenic bladder, obstructive uropathy) • Physically restrained (other than side rail, daily) • UTI (Must have MD dx, tx, specific s/s, sig lab in 30 day lookback for MDS) • Self-report moderate to severe pain (From MDS interview only) • Fall with major injury (Fracture, dislocation, closed head inj w/altered consciousness, subdural hematoma) • • • • • Antipsychotic Use (Exclusions: Schizophrenia, Tourette's, Huntington’s) 3 short stay (< or = 100 CDIF) New/worsened pressure ulcers (St 2, 3, 4 only) Self-report moderate to severe pain (From MDS interview only) Newly received antipsychotic (Exclusions: Schizophrenia, Tourette's, Huntington’s) IMPACT Act: SNF Quality Reporting System (QRS) https://www.cms.gov/Medicare/Quality-Initiatives-Patient-AssessmentInstruments/NursingHomeQualityInits/SNF-Quality-Reporting.html 9/18/14: Improving Medicare Post-Acute Care Transformation Act of 2014 • Requires development of cross postacute setting quality comparisons for –Assessment and Quality Measures –Quality care and improved outcomes –Discharge Planning –Interoperability –Care coordination Post Acute Settings SNF Require skilled therapy 5xW or skilled Nsg 7xW IRF Therapy 15 hr wk 2 disc MD 3xW HHA Be homebound Require intermittent skilled therapy or nsg Standardization LTCH Stay > 25 days, rehab, resp ther, head trauma,pain mgt Standardized Patient Assessment Data • Requirements for reporting assessment data: – Providers must submit standardized assessment data through PAC assessment instruments – Data must be collected at admission and discharge for each patient, or more frequently as required • Data categories: – – – – – – Functional status Cognitive function and mental status Special services, treatments, and interventions Medical conditions and co-morbidities Impairments Other categories required by the Secretary Use of Standardized Assessment Data: HHAs: no later than January 1, 2019 SNFs, IRFs, and LTCHs: no later than October 1, 2018 34 QRP Measure Domains to be standardized: Skin integrity and changes in skin integrity Functional status, cognitive function, and changes in function and cognitive function Incidence of major falls Finalized in FY16 Rule; Will be collected Oct 1 – Dec 31 2016 Payment penalties will be for FY18 To be developed Medication reconciliation Transfer of health information and care preferences when an individual transitions Resource use measures, including total estimated Medicare spending per beneficiary Discharge to community All-condition risk-adjusted potentially preventable hospital readmissions rates. Going Forward: New Measure Development will Evolve Over Time Measure Specification thru rulemaking Collect Data for that measure 1 year later Impose penalties 2 yrs later SNF QRP Measures Finalized in FY16 rule making Percent of Residents or Patients with Pressure Ulcers That Are New or Worsened (short stay) Percent of Residents Experiencing One or More Falls with Major Injury (long stay) Percent of patients/residents with an admission and discharge functional assessment and a care plan that addresses function (Part A stay) Existing SNF QMs New 37 Data Collection • For these QRP Measures: – Collect data upon SNF admission & SNF discharge • This is a new way to calculate QMs • Data only collected/calculated on resident in a Part A SNF stay QRP Measures • First round with these 3 will be collected for three months only – Oct, Nov, Dec 2016 • Will only be collected on residents in a Medicare Part A stay – No other pay source, no MA plans • Will be collected using: – PPS 5 day MDS (existing) – SNF Discharge (new) • Upon discharge from a Part A stay – Even if remaining in the SNF afterwards QRP Measures Initial Year Data collected Q1 FY17 Will have 5 ½ months to submit/correct data (5/15/17) 2% reduction in market basket update for ENTIRE FY18 for noncompliance Non-Compliance • Beginning FY18, 80% of all MDSs submitted must contain 100% of the data elements required to calculate the 3 QRP measures. – No dashes in ANY calculator fields! • Direct items • Covariates • Exclusions • CMS intends to raise threshold going forward through rulemaking Data collection period for penalties: Phase In (If CMS plans come to fruition) Data Collected Q1 FY 2017 Q2, Q3, Q4 FY 2017 FY 2018 Penalties Apply FY 2018 FY 2019 FY 2020 We have one year to perfect data collection systems! We can expect more/different measures going forward Future updates to Pressure Ulcer QM under CMS consideration: Would require revising QM and MDS • Would include: – New unstageable pressure ulcers, including suspected deep tissue injuries (sDTIs) – Stage 1 or 2 Pressure ulcers that become unstageable due to slough/eschar Percent of patients/residents with an admission and discharge functional assessment and a care plan that addresses function • In first three days of SNF stay, must be at least one fxn goal • New section added to SNF MDS upon admit and DC only • At the time of discharge, function is reassessed using the same 6-level rating scale, to evaluate success in achieving goals – Unplanned discharge: Fxl status reporting will not be required Percent of patients/residents with an admission and discharge functional assessment and a care plan that addresses function • Requires new data elements on PPS 5 day and “SNF discharge” assessments – SNF DC assessment will be at the time of DC from the Part A stay, even if resident does not leave • 30% of SNF residents stay in facility after SNF discharge • Initial goals and fxl status must be determined no later than day 3 of SNF stay SNF measures under future consideration • SNF 30-day all-cause readmission measure • Application of the payment standardized Medicare spending per beneficiary • Percentage of residents at discharge assessment, who are discharged to a higher level or to the community • Potentially preventable readmissions • Drug regimen review with follow-up for identified issues Protecting Access to Medicare Act (PAMA) of 2014 Skilled Nursing Facility 30-Day All-Cause Readmission Measure (SNFRM) VALUE BASED PURCHASING INITIATIVE Overview • SNF payment rate must be based, in part, on performance on this measure starting Oct 1, 2018 • SNFs with the highest rankings must receive the highest incentive payments – SNFs with the lowest rankings receiving the lowest (or zero) incentive payments. – Lowest 40 percent of SNFs (by ranking) will be reimbursed less than they otherwise would be reimbursed without the SNF VBP program. Funding: CMS will withold 2% of SNF Medicare payments starting 10/1/18 CMS will keep 3050% 50-70% will be incentive payments to SNFs. Measure estimates risk-standardized rate of all-cause, unplanned hospital readmissions of SNF Medicare beneficiaries within 30 days of discharge from their prior proximal acute hospitalization • Claims based • Readmissions within 30-day window are counted regardless of whether the beneficiary is readmitted directly from SNF or had been discharged from SNF • Risk-adjusted based on patient demographics, principal diagnosis in prior hospitalization, comorbidities, and other health status variables that affect probability of readmission • Excludes planned readmissions since these are not indicative of poor quality Exclusions: • Hospital principal dx – cancer – rehabilitation, fitting of prosthetics, adjustment of devices – pregnancy • Pts who did not have Medicare A coverage for 12 months preceding hospital discharge – Or for full 30 day window • Post acute admission in 30 day window • More than 1 day between the hospital discharge and the SNF admission • Discharge AMA Calculation: Based on Standardized Risk Ratio (SRR): Ratio > 1 = high quality Ratio < 1 = poorer quality SNF’s Risk Standardized Readmission Rate (RSSR): SRR x Overall national raw readmission rate for all SNFs • CMS is required to replace this measure with an all-condition, risk-adjusted potentially preventable hospital readmission rate. CMS advises it intends to address this topic in future rulemaking. – Under development PAYROLL BASED JOURNAL (PBJ) PBJ: Payroll Based Journal • Staffing and census data be collected for each fiscal quarter through the QIES ASAP System • Includes hours worked by each staff member each day within the quarter – administration, physician services, nursing services, pharmacy services, dietary services, therapeutic services, dental services, podiatry services, mental health services, vocational services, clinical laboratory services, diagnostic x-ray services, administration & storage of blood, housekeeping services, other services. • Census data is census on the last day of the quarter. • Strict guidelines for timeliness of submission – If out of compliance subject to enforcement actions not yet defined. • Voluntary October 1, 2015. • Mandatory July 1, 2016 PBJ: Goals • Staffing is a vital components of a nursing home’s ability to provide quality care. • Over time, CMS has utilized staffing data for a myriad of purposes in an effort to more accurately and effectively gauge its impact on quality of care in nursing homes. • The data, when combined with census information, can then be used: – To report on SNF staffing levels – To report on employee turnover and tenure • Which can impact the quality of care delivered. Submission Timeliness • Submissions must be received by the end of the 45th calendar day (11:59 PM Eastern Standard Time) after the last day in each fiscal quarter. • Facilities may enter and submit data at any frequency throughout a quarter. • The last accepted submission received before the deadline will be considered the facility’s final submission. Accuracy: • Staffing information is required to be an accurate and complete submission of a facility’s staffing records. CMS will conduct audits to assess a facility’s compliance related to this requirement. Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities PFR 7/16/15 • When this improved staffing data is collected at the nursing home level, more accurate and reliable estimates of the care hours provided by staff categories will be available, potentially leading to updated research and reconsideration of HPRD requirements and recommendations. Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities PFR 7/16/15 • Our intent is to require facilities to make thoughtful, informed staffing plans and decisions that are focused on meeting resident needs, including maintaining or improving resident function and quality of life. • We maintain that such an approach is essential to person-centered care. • At this time, we have deferred deciding on any potential specific requirement pending evaluation of additional data that will be collected on payroll based staffing data. FOCUSED SURVEYS: A NEW HORIZON Focused Surveys • MDS/Staffing: Pilot complete; In nationwide roll-out, Phase 1 • Dementia Care: Pilot complete, Expansion in 2015 on a voluntary basis – Texas conducting a comprehensive survey effort with more states expected to participate • 7/17/15: Focused Survey on Medication Safety Systems has begun pilot testing Impact • Small number chosen by methods not publically reported • Surveys open or continue an enforcement cycle • Once out of “pilot” also contribute to 5 Star rating • May not be combined with annual survey • DISCUSSION Questions/Discussion