Cardiac Rehabilitation Accessibility Survey
advertisement

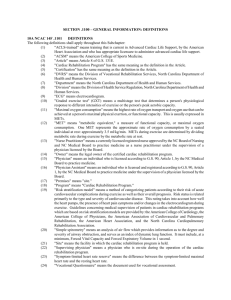
A Survey of Accessibility to Australia’s Phase 2 Cardiac Rehabilitation Programs Dr. Deborah van Gaans Centre for Research Excellence in the Prevention of Chronic Conditions in Rural and Remote Populations School of Population Health The research reported in this presentation has been supported by the Australian Primary Health Care Research Institute, which is supported by a grant from the Commonwealth of Australia as represented by the Department of Health and Ageing. The information and opinions contained in it do not necessarily reflect the views or policy of the Australian Primary Health Care Research Institute or the Commonwealth of Australia (or the Department of Health and Ageing). An Australian Research Council Funded Linkage Project with the Following Collaborating Partners : The University of Adelaide - Mr. Neil Coffee Alphapharm Pty Ltd. - Mr. Peter Astles, Ms. Marian Milligan University of South Australia - Dr. Robyn Clark University of Queensland - Professor David Wilkinson, Dr. Kerena Eckert Monash University - Professor Andrew Tonkin The Baker Heart Research Institute - Professor Simon Stewart Background Cardiac Event Cath Lab Local hospital GP Phone Ambulance Cardiac Speciality Area Home Transplant Cardiac Rehabilitation 1.Introduced into Australia by the National Heart Foundation in 1961. 2.By 1986, cardiac rehabilitation had advanced sufficiently for it to be seen as an important component of cardiac care. 3.Defined benefits include reduced mortality and reduced risk of further cardiac events; improvements in physical and social functioning, risk factor profiles and quality of life; and reduced prevalence of depression Source: Bunker, S,J, and Goble, A, J 2003, ‘Cardiac rehabilitation: under-referral and underutilisation’, MJA 2003; 179 (7): 332-333 Method Cardiac Rehabilitation Accessibility Survey Postal survey of all cardiac rehabilitation services (n=401) Completed surveys (n= 204) Services that did not run a Phase 2 Cardiac Rehabilitation Program (n= 158) No reply (n= 39) No time to fill out the survey (n= 28) Services that did not run a Phase 2 Cardiac Rehabilitation Program (n= 9) No reply (n= 2) Results The Cardiac Rehabilitation Accessibility Survey found the following: • 73% Phase 2 Cardiac Rehabilitation Programs in Australia require patients to have a referral prior to patients accessing their program. • All Phase 2 Cardiac Rehabilitation Programs in Australia were each run with very limited and specific hours of operation, with some programs operating as little as 2 hours a week. • Only 2% of the Phase 2 Cardiac Rehabilitation Programs ran out of hours sessions for patients. Results The Cardiac Rehabilitation Accessibility Survey found the following: • The Cardiac Rehabilitation Accessibility Survey found that more than half (56%, n=228) of the Phase 2 Cardiac Rehabilitation Programs Surveyed conducted both group and individual sessions. • Group only sessions were conducted by 36.8% of the total number of Phase 2 Cardiac Rehabilitation Programs in Australia. • Individual only sessions were run by only 6.6% of the Phase 2 Cardiac Rehabilitation Programs surveyed. Results The Cardiac Rehabilitation Accessibility Survey found the following: • 49% of Phase 2 Cardiac Rehabilitation Programs had all 6 recommended components the National Heart Foundations’ Recommended Framework (2004). • The percentage of Cardiac Rehabilitation Programs with components recommended by the NHF: Health education 96% Physical activity 96% Counselling 80% Behaviour modification strategies 84% Support for self-management 90% Cultural understanding 62% Source: National Heart Foundation and Australian Cardiac Rehabilitation Association, 2004, Recommended Framework for Cardiac Rehabilitation ’04, National Heart Foundation, Melbourne, Victoria. Results • Results from the Cardiac Rehabilitation Accessibility Survey show that 68% of Phase 2 Cardiac Rehabilitation Programs in Australia accept all age groups into their programs. • Of the 32% that did not accept all age groups into their programs all most all accepted patients from 35 to 85 years and older into their programs. Results • Results from the Cardiac Rehabilitation Accessibility Survey, reveal that completion rates of Phase 2 Cardiac Rehabilitation Programs are low with only 14 % of programs having 100% of patients complete their program. The survey also revealed that 18% of Phase 2 Cardiac Programs had half or less of their patients complete the program. Unknown Percentage of Patient Completions • 100% 90 - 99% 80 - 89% 70 - 79% 51- 69% 1- 50% 0% 0% 2% 4% 6% 8% 10% 12% 14% 16% Percentage of Phase 2 Cardiac Rehabilitation Programs 18% Results The National Heart Foundation identified the following core group of people who are eligible for cardiac rehabilitation: • • • • • Myocardial infarction (ST elevation MI, non-ST elevation MI) Re-vascularisation procedures Stable or unstable angina Controlled heart failure Other vascular or heart disease Source: National Heart Foundation and Australian Cardiac Rehabilitation Association, 2004, Recommended Framework for Cardiac Rehabilitation ’04, National Heart Foundation, Melbourne, Victoria. Results Discharge Diagnosis Accepted into Phase 2 Cardiac Rehabilitation Programs. Results Postal Internet 12% 3% Home visits 52% of Phase 2 Cardiac Rehabilitation Programs operate out of an acute public hospital. • Programs offering alternative modes of delivery such as: telephone service (28%), home visits (25%), postal (12%) and internet (3%), are limited. 25% Telephone service 28% As part of an outreach service to communities Setting • 8% Within a private outpatient service 3% Within a public community health centre/service 33% Within a non-acute/community hospital 7% Within an Aboriginal medical service 2% Within an acute private hospital 8% Within an acute public hospital 52% 0% 10% 20% 30% 40% 50% Percentage of Phase 2 Cardiac RehabilitationPrograms 60% Results • The Cardiac Rehabilitation Accessibility Survey revealed that only 23% of Phase 2 Cardiac Rehabilitation Programs in Australia are provided to the patient as a free service. • Schemes to make the Phase 2 Cardiac Rehabilitation Programs accessible to poorer patients such as Medicare (59%), Centrelink (56%), Health Card (57%) and Department of Veteran Affairs Cards (70%) were not accepted at all programs. • Extra costs were also identified through the survey which ranged from a gold coin donation per session to $60 per session. Conclusion • Results from the Cardiac Rehabilitation Accessibility Survey show that patient accessibility to Phase 2 Cardiac Rehabilitation Programs extends beyond service availability and includes various impediments that can prevent or limit service use. • The Cardiac Rehabilitation Accessibility Survey highlighted that the need for a referral, the cardiac disease the patient has, the provision of group and individual sessions, flexibility in service delivery setting, hours of operation, cost, and range of program components as significant barriers imposed by Phase 2 Cardiac Rehabilitation Programs that limit patient accessibility. • While patient barriers to cardiac rehabilitation are well documented, program barriers need to be considered by service providers when providing a Phase 2 Cardiac Rehabilitation Program, to improve accessibility. Dr. Deborah van Gaans Centre for Research Excellence in the Prevention of Chronic Conditions in Rural and Remote Populations School of Population Health Email: Deborah.vangaans@unisa.edu.au