13- Neck & Peripheral Vessels, Lymphatic System
advertisement

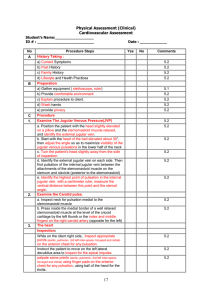
Peripheral Vascular System and Lymphatic System By InnaKorda, MD, Institute of Nursing, TSMU Direction of Blood Flow Lecture objectives: Structure and function of vascular system: Taking client’s complaints and history. Assessment techniques: Arteries Veins Lymphatics Inspection and palpation of the neck vessels Inspection and palpation of the arms (radial pulse, lymph nodes) Inspection and palpation of the legs (edema, Homans’ sign; femoral, popliteal, dorsalis pedis pulses, manual compression test Additional techniques: Trendelenburg test, colour changes, doppler ultrasonic stethoscope. Abnormal findings: Variations in arterial pulse Raynauld’s syndrome Lymphedema Arteriosclerosis Superficial varicose veins Peripheral artery disease: occlusions, aneurysms Structure And Function The vascular system consists of the vessels of the body. Vessels are tubes for transporting fluid, such as the blood or lymph. Function - transporting the blood or lymph : Delivery of oxygen to the tissues Delivery of nutrients to the tissues Elimination of carbon dioxide from cells Elimination of waste products from cellular metabolism Arteries. Carry freshly oxygenated blood to tissues High-pressure system Walls are strong, tough, and tense with elastic fibers ► stretch with systole, recoil with diastole with muscle fibers (VSM) ► control the amount of blood delivered to the tissues and the rate of blood flow Pulse is a pressure wave created by each heartbeat, palpable at body sites where the artery lies close to the skin and over a bone. Arteries accessible to examination Temporal artery (review chapter 13) Carotid artery Arteries in the arm: Brachial Radial Ulnar Arteries in the leg: Femoral artery Popliteal Anterior tibial ► dorsalis pedis Posterior tibial ► plantar arteries Ischemia is a deficient supply of oxygenated arterial blood to a body part, due to constriction or obstruction of a blood vessel Arteries accessible to examination Arteries accessible to examination Veins accessible to examination Jugular veins Veins in the arm: Superficial – in the subQ tissue, responsible for most of the venous return Deep Veins in the leg: Deep veins: femoral, popliteal; responsible for most of the venous return Superficial: great and small saphenous Perforators: connecting veins that join the two sets. They have one-way valves ► blood ► into the deep veins. Veins accessible to examination Lymphatics. A completely separate vascular system. It retrieves excess fluid from the tissue spaces and returns it to the blood stream. Lymphatic ducts and drainage patterns Functions of the lymphatic system: To converse fluid and plasma proteins that leak out of the capillaries. To form the major part of the immune system that defends body against infection. To absorb lipids from the intestinal tract. Structure of the lymphatic system Microscopic open-ended tubes (capillaries) Vessels, like veins, have valves Lymphatic ducts Subclavian veins Lymphoid tissue: Lymph nodes: Tonsils: Filter the fluid before it comes back to the bloodstream Filter out microorganisms Pharyngeal (adenoid) Palatine Lingual Spleen Peyer’s patches (Lymphoid tissue in intestines) Tymus gland Bone marrow Groups of peripheral lymph nodes: 1. 2. 3. 4. 5. 6. 7. 8. 9. Auricular: anterior and posterior Sublingual. Submandibular. Cervical: anterior and posterior. Supra- and subclavian. Axillary. Epithrochlear. Inguinal. Popliteal. Assesment: Inspection and palpation Amount in each group Size Shape Consistency Movable/connected with surrounding tissues Pain/tenderness Signs of inflammation: swelling and redness above the node Claudication distance is the number of blocks walked or stairs climbed to produce pain. Note sudden dencrease in claudication distance, or pain suddenly not relieved by rest. Taking client’s complaints and history. Ask: “Any leg pain (cramps)? Where?” Detail: pain type, onset (gradual/sudden), aggravating/ relieving factors (activity, walking, dangling, rubbing), associated signs (skin changes, sexual malfunction), relation to time of day, claudication distance. Edema is bilateral when caused by a systemic problem (heart failure), or unilateral when due to a local obstruction or inflammation. Taking client’s complaints and history. Objective data Preparation: Environment Privacy Should be warm (about 22°C) and draftless to prevent vasodilatation or vasoconstriction. Make sure the female’s breasts and client’s genitals remain draped. Order of exam Begin with observations peripherally and move toward the heart. 1. 2. 3. 4. Pulse and blood pressure Extremities – peripheral vascular assessment Neck vessels Precordium – (portion of body over heart and thorax) Equipment needed: Tourniquet or blood pressure cuff Stethoscope Paper tape measure Doppler ultrasonic stethoscope Assessing Neck Vessels Carotid Artery Palpate the carotid artery Avoid excessive pressure. Excessive vagal stimulation could slow down heart rate. Carotid arteries should be same bilaterally Auscultation Listen for bruits – blowing, swishing sounds indicating blood flow turbulence. Caused by atherosclerotic narrowing (one half or two thirds of artery). Assessing Neck Vessels Jugular Veins Can be used to assess central venous pressure (CVP) and cardiac efficiency Position the patient at 30-45 degree angle, wherever pulsations can be seen best. Remove pillow to avoid flexion of head. Distended external jugular veins signify increased CVP, as with heart failure The higher the CVP, the higher the position you will need Turn the pt’s head away from examiner’s side Distinguish from carotid artery pulsations. Internal jugular pulse is lower, varies with respiration, not palpable, and disappears as person is sitting. Assessing Neck Vessels Jugular Venous Pressure Estimate Used to assess heart failure Position the patient at 30-45 degree angle. Place one ruler vertically at the manubriosternal angle. Place a second ruler perpendicular to the first and record the height of pulsation of the internal jugular vein. Normal pulsation is 2 cm or less above sternal angle Pulsations 3 or more cm above sternal angle while at 45 degrees occur with heart failure Record height of pulsations and degrees of elevation Question The examiner has estimated the jugular venous pressure. Identify the finding that is abnormal. 1. 2. 3. 4. Patient elevated to 30 degrees, internal jugular vein pulsation at 1 cm above sternal angle. Patient elevated to 30 degrees, internal jugular vein pulsation at 2 cm above sternal angle Patient elevated to 40 degrees, internal jugular vein pulsation at 1 cm above sternal angle Patient elevated to 45 degrees, internal jugular vein pulsation at 4 cm above sternal angle Inspection and palpation of the arms Inspect for: Color of skin and nailbeds Temperature, texture and turgor of skin Any lesions, edema Nail clubbing. 160 degrees What is normal nail bed angle? Use profile sign to detect early clubbing Capillary refill is an index of peripheral perfusion and cardiac output. Depress and blench the nail beds; release and note the time for color return. Normally 1 to 2 seconds. Inspection and palpation of the arms Palpate both radial pulses: Symmetricity (equal force), rhythm, rate, elasticity. Grade the force (amplitude) on a fore-point grade: 0 – absent 1+, weak 2+, normal 3+, increased 4+, bounding For ulnar pulse palpate along the medial site of the inner forearm. Not palpable in healthy person. Inspection and palpation of the arms Palpate the brachial pulses. Palpate the epitrochlear lymph node Modified Allen test: Normal 2 to 5 seconds