Shared Decision Making
advertisement

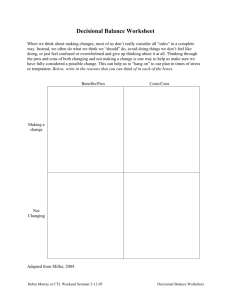
Shared Decision Making: Partnering with People to Support Informed Healthcare Decisions Etta Mitchell, LMSW September 23, 2011 Wellness Focus • Focused on the ‘whole person’- integrated physical and mental health care • Learning to provide healthcare management, bringing together all domains of treatment to one cohesive resource. Critical Care • We serve an ‘at risk’ population with a lifespan of up to 25 years less than the average population. • Healthcare challenges such as diabetes, obesity, cardiovascular disease, respiratory disease, infectious diseases, suicide, and mortality. • Lack of well coordinated care a contributor • Work, support, encourage, and care with a sense of URGENCY!! (Parks, Svendsen, Singer, Foti, & Mauer, 2006) • • • • • • • • • Freddie Michael Sue Patty Burt Francis Media Shaylynn David This is Not About Statistics. It’s Personal! It’s Personal Science—Suffering Treatment---Healing Empirical Facts----Hope Population Samples---Individuals Statistical Problem---Me Typical Medical Intervention • Average appointment with a physician 15-20 minutes • Within an appointment, the physician must: – Establish a ‘therapeutic alliance’ – Gather information- history, mental status, lab results, key issues – Treatment Planning- safety, adherence, side effects, general medical conditions – Establish a diagnosis and treatment goals- share information with the individual, prescribe intervention – Action-referrals, order labs, complete documentation, provide educational resources, determine follow up appointment. Consequences • Frustration with care because people feel they do not have input into decisions that effect health and lifestyles • Wasted resources on appointments not kept and prescriptions filled but not taken • 1/3 of the people that enter into care, disengage. • Use of emergent care and crisis services increase (Deegan, 2010) Medication Trap Symptoms increase, I can’t take care of my kids I want to be a good mother I take my medication and do what my doctor says to do I stop taking medications My medications make me sleepy. I am unable to get my kids on the school bus Substance Use Trap My friends are very important to me. We party together every weekend I take my medications and follow directions, but I miss my friends! I am told not to party anymore. If I do, my doctor will refuse to treat me. I will be drug tested. When we party, I forget to follow my plan for diabetes but I do pretty well during the week I get sick, and end up in the hospital I know I need to but….. I love to cook southern food for my family. Family dinners make me feel close to them. No one likes my new food and my family stops coming to dinner I try to change the way I cook but I don’t know how, and I get food from the food pantry that is not on my special diet I have high blood pressure and southern food is full of salt and sugar I don’t feel good, I go to the doctor. She tells me no more southern cooking. Shared Decision Making • A experience where clinicians and patients talk about what is important to the individual and how it is impacted by healthcare challenges. They discuss the diagnosis and best evidence based treatment options. Recognizing that some medical choices are not as simple as ‘compliance’ and ‘noncompliance’, individuals are supported to think about the benefits and costs of all options. This leads to a consensus in the treatment plan, which is sometimes a compromise on both parts. • Term first used in the ‘President's Commission for The Study of Ethical Problems in Medicine and Biomedical Research’ in 1998. • Expanded to include mental and physical healthcare. • Pat Deegan & Associates Foundations of Shared Decision Making • The person is able to share what is most important to them, their motivation for wellness. “Working at the library is the most important thing to me right now. I need help to management my diabetes and depression so that I can be a good clerk.” **This message should be personal and not about symptom abatement • The person is informed about their diagnosis and possible treatments. Foundations of Shared Decision Making • There is a change in the doctor-patient relationship. There are now to experts in the room. – The person is empowered to ask questions, express concerns and disagreement, and engage in clinical discussions. – The clinician learns to start conversations that promotes shared decision making, and expresses respect for the individual’s values, preferences, and right to choose. Foundations of Shared Decision Making • A team approach to include the individual, friends and family members, social workers, therapists, CSSs, nurses, and other clinicians. Anyone that the individual identifies as a support! – Supplements the brief medical appointment • • • • Educational materials and resources Peer support Decision aides Support with decisional uncertainty How Can You Help? • Assist the individual access information about the diagnosis that is clear and easy to read. • Encourage them to develop questions to ask in the medical appointment- write them down. • Support the individual to practice having difficult medical discussions- stating what is most important to them and knowing how to disagree or express concern. How Can You Help? • Support them with decisional uncertainty Many decision aides available: www.bcbs.com/betterknowledge/tec/ www.Cochrane.org http://decisionaid.ohri.ca/decguide.html www.informedmedicaldecisions.org http://effectivehealthcare.ahrg.gov http://mentalhealth.samhsa.gov/consumersurvivor Great work creating “Cool Tools” www.healthwise.net Decisional Aides • Created by unbiased sources with unbiased content • Peer support and recovery stories • Support groups • Booklets, articles, CD Rom • Worksheets to weigh benefits to risksImportant to assign importance or value to each item Pat Deegan and Associates Non Compliance • Compliance communicates a paternalistic stance regarding healthcare decisions • Adherence is a personal and complicated decision, not an arbitrary one. Decisional Uncertainty with Medication • People have several reasons for decisional uncertainty regarding medications: Side effects Meds unhelpful Health Concerns Interactions with other medications Interactions with substance use Need more support Exploration Logistics- co-pays and transportation Confusion Beliefs Fears Motivation Pat Deegan & Associates Antipsychotic Medication • Questions often asked by consumers: • Which one will present the least risk for metabolic dysregulation? • Will I gain weight and get diabetes? • Will it cause sexual dysfuntion? • Can I use alternative options such as vitamins, psychotherapy, or watchful waiting? • What if I get pregnant? • What about hair loss or tremors? • What about sudden death? • Be open to exploration, not dismissive Decisional Aide Yeah...but…. • People do not know enough to make informed medical decisions • There is not enough time in the appointment. • I am not going to prescribe whatever patients want! • What if people make the ‘wrong decisions’? Listen, present options with facts, arrange for decisional support and peer support More Concerns • People that say, “I don’t have a mental illness.” Avoid the power struggle! Build common ground by discussing what is important to them, how their life is impacted. It does not matter if they accept the label, focus on the impact of quality of life. • People who are not able to make decisions for themselves. • Help to create advance directives and proxy decision makers, in essence a good crisis plan. • Not appropriate for emergencies, people without capacity- Alzheimers, intoxication, delirium Research • Has indicated that the decision making process for people with mental health diagnoses do not differ from people with other major medical diagnoses. In fact, they express and increased desire to participate. (The MacArthur Treatment Competence Study, 1995) • Shared Decision Making – Increases favorable health outcomes (Kaplan, Greenfield, & Ware, 1989) – – – – – – Empowers people to make decisions Reduces anxiety Promotes recovery Increases adherence (Guadagnoli & Ward, 1998). Leads to reduced demand for healthcare resources Reduces medical cost DNKA rate, unused medications (Devine & Cook, 1983) Bottom Line • People want good information • People want to feel listened to • People want a say in things that affect their lives • People have the right and ability to make decisions about treatment!! Laurie Curtis, SAMHSA 2010 BE THE DIFFERENCE References Adams, J., Drake, R.,& Wolford, G.(2007). Shared decision-making preferences of people with severe mental illness. Psychiatric Services 58, 1219–1221. Devine, E. & Cook,T. (1983). A meta-analytic analysis of effects of psychoeducational interventions on length of postsurgical hospital stay. Nurs Res, 32 ,267-74. Deegan, P. (2010). A description of a web application to support shared decision making. Psychiatric Rehabilitation Journal, 34(1):23-8. Deegan, P., & Drake, R. (2006). Shared decision making and medication management in the recovery process. Psychiatric Services, 57, 1636–1639. Drake, R.., Deegan, P., & Rapp, C. (2010). The promise of shared decision making in mental health. Psychiatric Rehabilitation Journal, 34(1),713. Drake, R., & Deegan, P. (2009). Shared decision making is an ethical imperative. PsychatricServ.60, 1007. Greenfield ,S., Kaplan, S., & Ware , J. (1985). Expanding patient involvement in care. Effects on patient outcomes. Ann Intern Med, 102, 5208. Greenfield ,S., Kaplan, S., & Ware J.(1988). Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. J Gen Intern Med, 3(5), 448-57. Grisso, T., Appelbaum, P., Mulvey, E., & Fletcher, K. (1995). The MacArthur treatment competence study. II: Measures of abilities related to competence to consent to treatment. Law and Human Behavior, 19(2), 127-148. Guadagnoli, E., & Ward, P. (1998). Patient participation in decision-making. Soc Sci Med , 47(3), 329-39. Kaplan, S., Greenfield, S., & Ware, J. (1989). Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care , 27, 110-27. Parks, J., Svendsen, D., Singer, P., Foti, M., & Mauer, B. (2006). Morbidity and Mortality in People with Serious Mental Illness. National Association of State Mental Health Program, National Association of State Mental Health Program Directors, Medical Directors Council, Alexandria Virginia. President's Advisory Commission on Consumer Protection and Quality in the Health Care Industry (1998). "Quality First: Better Health Care for All Americans“ http://www.samhsa.gov/consumersurvivor/SDMWebinar/html/slide_001.html