Creatine What Is Creatine?
advertisement

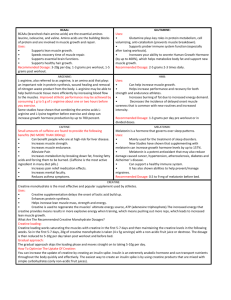
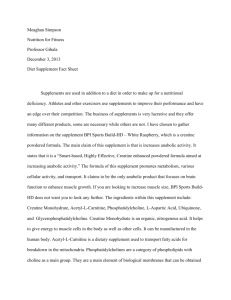
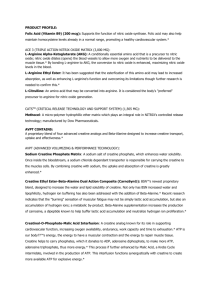
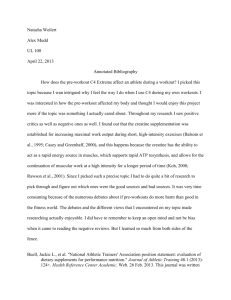
Ergogenic Aids: Creatine What Is Creatine? Amino acid derivative found mainly in skeletal muscle (90% to 95%) – Small amounts in brain, testes, and cardiac muscle tissues – Synthesized from glycine, arginine, and S-adenosylmethionine (1 to 2 g/day) – Found in meats (meat eaters consume 1 to 2 g/day) Acts as a reservoir for high-energy phosphate needed for adenosine triphosphate (ATP) synthesis – Phosphorylated creatine (creatine phosphate, or phosphocreatine) can donate a phosphate group to adenosine diphosphate (ADP) to make ATP Phosphocreatine stores depleted after 10 to 20 seconds of intense exercise Abbreviations: ADP, adenosine diphosphate; ATP, adenosine triphosphate. Juhn MS, et al. Clin J Sport Med. 1998;8(4):286-297. The Creatine Phosphate Pathway 3 different types (isoforms) of creatine kinase (CK) Urinary excretion – CK-BB, or CK-1 (brain, lung) – CK-MB, or CK-2 (cardiac) – CK-MM, or CK-3 (skeletal muscle) Abbreviations: ADP, adenosine diphosphate; ATP, adenosine triphosphate; BB, brain/brain; CPK, creatine phosphokinase; MB, muscle/brain; MM, muscle/muscle. Reprinted from Smith C, et al. Marks’ Basic Medical Biochemistry: A Clinical Approach. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:870-871. Potential Mechanisms for Benefits of Creatine for Athletes Loading can increase stores of phosphocreatine in muscle cells1 – Increased ATP production during high-intensity exercise – Diminished dependence on glycolysis and subsequent lactic acid formation • Indirect buffering of muscle pH – Faster re-synthesis of ATP after exercise Affects muscle cell stretching, which may trigger cell growth2 – Osmotically active inside muscle cells; water follows it into the cell Influences other pathways in the cell that increase the ratio of protein synthesis to protein breakdown3,4 – – – – Increased myogenic regulatory factors Increased insulin-like growth factor (IGF-1) expression Decreased myostatin levels in blood (myostatin reduces muscle growth) Decreased cellular damage following high-intensity exercise Abbreviations: ATP, adenosine triphosphate; IGF-1, insulin-like growth factor. 1. Terjung RL, et al. Med Sci Sports Exerc. 2000;32(3):706-717. 2. Haussinger D, et al. Lancet. 1993;341(8856):1330-1332. 3. Saremi A, et al. Mol Cell Endocrinol. 2010;317(1-2):25-30. 4. Deldicque L, et al. J Appl Physiol. 2008;104(2):371-378. Typical Creatine Feeding Protocol Loading period for rapid increase in muscle creatine – Approximately 20 g/day (~0.3 g/kg/day) for 3 to 5 days • 5 g, 4×/day Maintenance phase – 2 to 5 g/day indefinitely Slower increase in muscle creatine – 3 g/day for 28 days results in similar muscle creatine levels as in the loading phase Mc Ardle WD, et al. Sports and Exercise Nutrition, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:3476-377. Evidence for Creatine Benefits on Performance and Strength/Muscle Mass > 500 studies have evaluated the benefits of creatine in sports nutrition – None have shown detrimental effects – 300 examined performance: ~70% show significant improvements Performance benefits include: – – – – Maximal power/strength (5% to 15%) Work performed during sets of maximal effort muscle contractions (5% to 15%) Single-effort sprint performance (1% to 5%) Work performed during repetitive sprint performance (5% to 15%) Performance benefits generally limited to high-intensity, anaerobic exercise Supplementation during training is associated with a 0.5- to 2-kg greater increase in body mass (BM) and/or fat-free mass (FFM) than training alone – Includes trained and untrained adolescent, adult, and elderly populations – Both males and females respond equally well Abbreviations: BM, body mass; FFM, fat-free mass. Kreider RB. Mol Cell Biochem. 2003;244(1-2):89-94. Effects of Creatine Loading on Muscle Creatine Levels Total creatine, mmol/kg dm A 160 * 150 140 130 20 g creatine/day for 6 days, none after 120 110 100 Day 0 Day 7 Day 21 Day 35 * * * Total creatine, mmol/kg dm B 160 150 140 20 g creatine/day for 6 days, then 2 g/day for remainder of study 130 120 110 100 Day 0 Day 7 Abbreviation: dm, dry mass. *Significantly different from day 0, P < .05. Reprinted from Hultman E, et al. J Appl Physiol. 1996;81(1-2):232-237. Day 21 Day 35 Influence of Creatine Loading on Myostatin Levels During 8 Weeks of Resistance Training (Typical 2 Phase Loading Protocol) Week 0 Week 4 Week 8 Myostatin, ng/mL 140 120 100 80 60 40 20 0 CON Abbreviations: CON, control; CR, creatine; PL, placebo; RT, resistance training. Reprinted from Saremi A, et al. Mol Cell Endocrinol. 2010;317(1-2):25-30. RT+PL RT+CR Influence of Creatine on Markers of Muscle Damage After the Ironman Triathlon * 4000 *** ns 3000 ** 2000 1000 0 Placebo Creatine supplemented ns 700 600 500 400 300 200 100 0 Placebo Triathletes 0 hours ns * Plasma activity of LDH, U/L Plasma activity of CK, U/L * 36 hours 60 hours 0 hours Creatine supplemented Triathletes 36 hours 60 hours Subjects: Ironman triathletes Treatments: 20 g/day creatine + 50 g carbohydrate for 5 days prior to the race Control: 50 g carbohydrate only Analysis: Markers of muscle damage measured at baseline and 36 or 60 hours after the race Abbreviations: CK, creatine kinase; LDH, lactate dehydrogenase; ns, not significant. *P < .05; **P < .01; ***P < .001. Reprinted from Bassit RA, et al. Eur J Appl Physiol. 2010;108(5):945-955. Example of Anaerobic Performance Benefit From Creatine * Subjects: 14 active, but not “well-trained” males Treatments: 5 g creatine monohydrate + 1 g glucose polymer for 5 days Control: 6 g glucose polymer for 5 days Training: 10 sets of either 5 or 6 x6-second maximal bike sprints with varying recoveries (24, 54, or 84 seconds between sprints) over a period of 80 minutes Assessed before (pre-loading) and after (post-loading) 5 days of treatment Data are mean ± standard error. *P < .05 vs placebo. Data from Preen D, et al. Med Sci Sports Exerc. 2001;33(5):814-821. Example of Creatine Effectiveness For Strength and Muscle Mass * * Subjects: Treatments: Training: 19 healthy, resistance-trained men 25 g creatine/day for 7 days 5 g creatine/day for 11 weeks Controls: identical amounts of cellulose powder 12-week resistance training Data are mean ± standard error. Abbreviations: BM, body mass; FFM, fat-free mass; FM, fat mass. *P ≤.05 vs placebo. Data from Volek JS, et al. Med Sci Sports Exerc. 1999;31(8):1147-1156. Creatine Effects on Increase in Cross-Sectional Area in Different Muscle Fiber Types * * * Change in area from Week 0 to Week 12, µm2 Data are mean ± standard error. *P ≤.05 vs placebo. Data from Volek JS, et al. Med Sci Sports Exerc. 1999;31(8):1147-1156. Is the Form of Creatine Important? Creatine monohydrate by far the most commonly studied – Therefore, most evidence for efficacy Creatine not stable in liquids over a period of time – Conversion to creatinine – Creatine liquids or serums not as effective as powder1 Limited studies with other forms – Creatine ethyl ester, creatine pyruvate, creatine with D-pinitol, polyethylene glycosylated creatine, etc – No consistent improvements relative to creatine monohydrate • Hard to improve on bioavailability of creatine monohydrate – These forms are likely more expensive 1. Gill ND, et al. J Strength Cond Res. 2004;18(2):272-275. Carbohydrate and Protein in the Facilitation of Muscle Creatine Uptake 60% increase in total muscle creatine in experimental group1 – N = 24 males – 5 g creatine followed by 93 g glucose 30 minutes later; repeated 4×/day – Control was 5 g creatine 4×/day Carbohydrate/Protein (carb/pro) and high-carbohydrate treatments had similar creatine retention2 – 5 g creatine 4×/day plus one of the following each time: • Placebo: 5 g glucose • Carb/pro: 47 g glucose and 50 g protein • High carb: 96 g glucose • Low carb: 50 g glucose – Low-carbohydrate treatment was not significantly different than placebo The large insulin response to either the high-carbohydrate or carb/pro combination is likely responsible for driving further uptake of creatine by muscle cells Abbreviation: carb/pro, carbohydrate/protein. 1. Green AL, et al. Am J Physiol Endocrinol Metab. 1996;271(5):E821-E826. 2. Steenge GR, et al. J Appl Physiol. 2000;89(3):1165-1171. Caffeine + Creatine: Is This a Concern? Caffeine eliminated the positive effect of creatine on a knee extensor exercise in 1 study1 – High caffeine dose (5 mg/kg/day) – 0.5 g/kg/day creatine for 6 days – Caffeine did not inhibit the increase in muscle creatine concentration Performance benefits shown in other studies of creatine2,3 – With lower doses of caffeine – With other nutrients 1. Vandenberghe K, et al. J Appl Physiol. 1996;80(5):452-457. 2. Kraemer WJ, et al. Eur J Appl Physiol. 2007;101(5):637-646. 3. Smith AE, et al. J Int Soc Sports Nutr. 2010;7:10 doi: 10.1186/1550-2783-7-10. Creatine Nonresponders? Individuals with high muscle levels of total creatine (> 120 mmol/kg dry matter) may not be as responsive to creatine supplementation1 – Conversely, vegetarians have lower creatine stores and may be more responsive to creatine supplementation (loading and performance)2 1. Greenhaff PL, et al. Am J Physiol Endocrinol Metab. 1994;266(5):E275-E730. 2. Burke DG, et al. Med Sci Sports Exerc. 2003;35(11):1946-1955. Creatine Side Effects Generally well tolerated in the gastrointestinal tract when dose is ≤ 5 g1 at one time Weight gain is common (may or may not be considered a “side effect”) Early concern was potential muscle cramping and impaired temperature regulation2,3 – Possibly related to fluid shift to intracellular space (less circulating fluid) Several recent studies have dispelled any concern regarding creatine with regard to muscle cramping, heat tolerance, and hydration status3,4,5 – May actually augment sprint performance and reduce cramping in the heat6 1. Ostojic SM, et al. Res Sports Med. 2008;16(1):15-22. 2. Dalbo VJ, et al. Br J Sports Med. 2008;42(7):567-573. 3. Lopez RM, et al. J Athl Train. 2009;44(2):215-223. 4. Greenwood M, et al. J Athl Train. 2003;38(3):216-219. 5. Volek JS, et al. Med Sci Sports Exerc. 2001;33(7):1101-1108. 6. Wright GA, et al. J Strength Cond Res. 2007;21(3):655-660. Creatine Safety Most publicized potential safety concern is renal function Long-term studies of the safety of creatine in athletes are lacking The general safety of creatine is supported via several lines of evidence – Creatine supplementation (up to 5 years) in athletes have not shown impairment in renal function or other clinical markers with up to 20 g/day in healthy athletes1,2,3 – Short-term studies have shown no effects of creatine supplementation on renal parameters or hematologic indices4,5,6,7 • Loading: 15 to 20 g/day for 5 to 7 days • Maintenance: 3 to 10 g/day for up to 9 weeks – Comprehensive risk assessment showing an Observed Safe Level (OSL) of 5 g/day for chronic supplementation8 – Long-term studies of creatine use in clinical populations such as patients with Parkinson’s disease and gyrate atrophy of the choroid and retina have not shown adverse effects9,10,11 • Typically maintenance doses (1.5 to 4 g/day) have been used for up to 5 years 1. Poortmans JR, et al. Med Sci Sports Exerc. 1999;31(8):1108-1110; 2. Mayhew DL, et al. Int J Sport Nutr Exerc Metab. 2002;12(4):453-460; 3. Kreider RB, et al. Mol Cell Biochem. 2003;244(1-2):95-104; 4. Poortmans JR, et al. Eur J Appl Physiol Occup Physiol. 1997;76(6):566-567; 5. Robinson TM, et al. Br J Sports Med. 2000;34(4):284-288; 6. Gualano B, et al. Eur J Appl Physiol. 2008;103(1):33-40; 7. Cancela P, et al. Br J Sports Med 2008;42(9):731-735; 8. Shao A, et al. Regul Toxicol Pharmacol. 2006;45(3):242-251; 9. Bender A, et al. Nutr Res. 2008;28(3):172-178; 10. Sipila I, et al. N Engl J Med. 1981;304(15):867-870; 11. Vannas-Sulonen K, et al. Ophthalmology. 1985;92(12):1719-1727. Creatine Safety (continued) There have been a few isolated case reports of kidney dysfunction (interstitial nephritis) that have been associated with creatine supplementation1,2,3 In each of these case studies, there are factors that greatly limit interpretation of the results – The patient had pre-existing kidney disease1 – The patient took 20 g/day for 4 weeks (exceeded recommended dose) and symptoms started 4 weeks after stopping creatine2 – The patient took only 15 g creatine/week and was on many other dietary supplements (17 amino acids, 18 herbal/plant extracts, and 16 other nutritional supplements)3 • Symptoms resolved when ALL supplements were stopped • Causative agent could not be identified 1. Pritchard NR, et al. Lancet. 1998;351(9111):1252-1253. 2. Koshy KM, et al. N Engl J Med. 1999;340(10):814-815. 3. Thorsteinsdottir B, et al. J Ren Nutr. 2006;16(4):341-345. Creatine Safety—Summary Creatine has an excellent overall safety profile in a variety of healthy populations when taken as recommended – Do not exceed recommended doses: • Loading: 20 g/day • Maintenance: 5 g/day Creatine should not be taken by persons with pre-existing kidney disease As with any dietary supplement, the user’s physician should be made aware of its use in the rare event that an adverse effect is experienced