Center for Child Health, Behavior and Development
advertisement

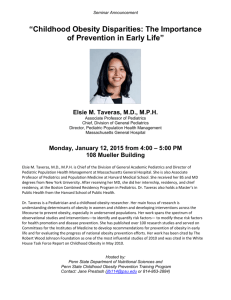
Center for Child Health, Behavior and Development Prevention and Treatment of Childhood Obesity Jason A. Mendoza, MD, MPH Associate Professor of Pediatrics University of Washington Benton Franklin County Medical Society CME February 2015 Center for Child Health, Behavior and Development Presentation goals • Scope of the Obesity Epidemic • Prevention • Safe Routes to School (SRTS) • Treatment Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 1985 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 1993 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 1997 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% ≥20% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 2001 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 2004 (*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%–14% 15%–19% 20%–24% ≥25% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 2009 No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30% Center for Child Health, Behavior and Development Obesity Trends* Among U.S. Adults BRFSS, 2013 Center for Child Health, Behavior and Development Obesity among US children and adolescents aged 10 to 17 in 2003 Singh, G. K. et al. Arch Pediatr Adolesc Med 2010;0:2010.84-10. Center for Child Health, Behavior and Development Obesity among US children and adolescents aged 10 to 17 in 2007 Singh, G. K. et al. Arch Pediatr Adolesc Med 2010;0:2010.84-10. Center for Child Health, Behavior and Development Global Obesity Problem Center for Child Health, Behavior and Development Responsibility • Personal: • Individuals make choices & “get what they deserve” • Ignores children’s developmental status and impact of family, school, and community environments • Collective: • Individuals make choices but within the influence of the environment • Create a healthier “default” setting through policy and environmental changes *Brownell et al, Health Affairs 2010 Center for Child Health, Behavior and Development Environment and policy • Environment: • Built environment • Availability/access (parks, grocery stores) • Foods offered in a school or business • Policy: • Costs of foods; incentives for behaviors • Regulation of environments, i.e. sidewalks for new housing developments Center for Child Health, Behavior and Development Ecological approach Sallis JF et al. Annual Review of Public Health. 2006;27(1):297-322 Center for Child Health, Behavior and Development Obesity Care Model Barlow S E Pediatrics 2007;120:S164-S192 Center for Child Health, Behavior and Development ©2007 by American Academy of Pediatrics Background Childhood obesity highly prevalent in US • 16.9% of 2-19 year olds were obese in 2011-12 (Ogden et al, 2014) • 18.4% of 4 year old were obese in 2005 (Anderson et al, 2009) • 31.2% American Indian/Native Alaskan • 22.0% Hispanic • 20.8% Black • 15.9% White Center for Child Health, Behavior and Development Background Pediatric obesity tracks strongly into adulthood (Whitaker et al, NEJM 1997) • Obese 15-17 year old: OR=17.5 (7.7-39.5) • Adolescent obesity tracks most strongly into adulthood Center for Child Health, Behavior and Development Obesity complications From: CDC Vital Signs 2010 Center for Child Health, Behavior and Development Obesity is costly; Prevention saves $ Health care spending for obesity est. $210 billion (2008) or 21% of US GDP (Cawley and Meyerhoefer, J. Health Econ. 31:1 (Jan 2012): 219–30) Center for Child Health, Behavior and Development Obesity treatment Childhood obesity highly prevalent • Can clinicians provide effective services to 1/3 of ALL children and adolescents in the US, i.e. overweight and obese? Behavioral treatment interventions • Modest success but required >25-75 hours therapy (USPSTF 2010) • Most clinicians cannot provide intensive multidisciplinary therapy Focus on Preventing Obesity Center for Child Health, Behavior and Development Childhood Obesity Prevention 7-5-2-1-0: a useful menemonic • • • • • 7 days a week eat a healthy breakfast 5 serving of fruits and veggies/day 2 hours or less of screen time 1 hour or more of physical activity 0 sugared drinks – water/lowfat milk instead Center for Child Health, Behavior and Development The state of physical activity in the United States? Center for Child Health, Behavior and Development Physical activity in the US Troiano et al. MSSE 2008;40(1):181-188 Center for Child Health, Behavior and Development Decline in physical activity, 9-15 year olds in US Average Weekday and Weekend Minutes of MVPA by Gender Nader, P. R. et al. JAMA 2008;300:295-305. Center for Child Health, Behavior and Development Physical activity built into our days Center for Child Health, Behavior and Development Background Physical activity is important for prevention of: • • • • Obesity Cardiovascular disease Type 2 Diabetes/insulin resistance Multiple types of Cancer Physical activity is positively associated with cognitive and academic outcomes among children • Higher physical activity or fitness = higher scores • Suggests benefits of physical education and recess Center for Child Health, Behavior and Development Active commuting to school: The journey to school matters Center for Child Health, Behavior and Development Background In 1969, 48% of US children walked or biked to school vs. only 13% in 2009 (McDonald et al 2011) Active commuting to school (ACS): appears promising to increase physical activity • ACS = walking and cycling to school • ↑ACS is an objective of US Healthy People 2020 Barriers to ACS • • • • Safety concerns Distance to school Weather School policy Center for Child Health, Behavior and Development ACS, Physical Activity, & BMI NHANES study • • • n=789, 12-19 year olds Accelerometer-determined MVPA Height , weight , waist, and skinfolds measured per protocol • Results: • ACS positively related to daily MVPA (β=0.12, P=0.024) • 30 min ACS additional 4.5 min MVPA • ACS inversely related to BMI z-score (β=-0.07, P=0.046) • ACS inversely related to skinfolds (β=-0.06, P=0.029) Mendoza JA, et al. J Phys Act & Health. 2011;8(4):488-495 Center for Child Health, Behavior and Development What is this? *From Zhu X. and Lee C. Active Living Research Annual Conference 2007 http://activelivingresearch.com/files/Plenary_Zhu_0.pdf Center for Child Health, Behavior and Development Walkable? *From Zhu X. and Lee C. Active Living Research Annual Conference 2007 http://activelivingresearch.com/files/Plenary_Zhu_0.pdf Center for Child Health, Behavior and Development Walkability *From Zhu X. and Lee C. Active Living Research Annual Conference 2007 http://activelivingresearch.com/files/Plenary_Zhu_0.pdf Center for Child Health, Behavior and Development Walkable and Bikeable www.pedbikeimages.org | Dan Burden (top images) | Carl Sundstrom (bottom images) Center for Child Health, Behavior and Development Safe Routes to School (SRTS) In the US, federally funded SRTS program began in 2005 after successful pilot programs • Part of the federal Safe, Accountable, Flexible, Efficient Transportation Equity Act: A Legacy for Users (SAFETEA-LU) • Major goal: Promote walking and bicycling to school safely by primary and middle school students • Consist of four core elements • Education (for drivers) • Enforcement (law) • Engineering (sidewalk, road, built environment) • Encouragement (for students/families, e.g. walking school buses) Center for Child Health, Behavior and Development Safe Routes to School: infrastructure and walking/cycling More parents report children walking or biking to school after Safe Routes to Schools project completion % change in walking or biking to school 50% 45% 40% 35% 28.6% 30% 25% 19% 20% 20.6% 15.6% 13.7% 15% 10% 11.6% 12% 10.9% 6.7% 3.1% 5% 0% Juan Cabrillo Murrieta Sheldon Valley West Glenoaks Jasper Randall Mt. Vernon Cesar Chavez Newman Boarnet MG, Anderson CL, Day K, McMillan T, Alfonzo M. Evaluation of the California Safe Routes to School Legislation: Urban form changes and children’s active transportation to school. American Journal of Preventive Medicine 2005; 28(2S2):134-140. Center for Child Health, Behavior and Development Pedestrian crashes, New York City, 2001–2010 DiMaggio C , and Li G. Pediatrics 2013;131:290-296 Center for Child Health, Behavior and Development School-aged pedestrian crashes during school-travel hours, New York City No SRTS DiMaggio C , and Li G Pediatrics 2013;131:290-296 SRTS Center for Child Health, Behavior and Development Walking school bus A group of children led to school by parents/adults who walk together along a set route (active commuting) Addresses safety concerns: supervised period of physical activity and pedestrian safety teaching Pedestrian safety is modeled and taught Center for Child Health, Behavior and Development Walk to school studies Seattle: Quasi-experimental trial of the Walking School Bus (WSB) • Setting: inner-city public elementary schools in Seattle, WA • One intervention school and two comparison schools • Intervention school with WSB had 18% more ACS vs. comparison schools at 1-year (Mendoza, Levinger, and Johnston, BMC Public Health, 2009) Center for Child Health, Behavior and Development Walk to school studies Pilot randomized controlled trial of the WSB Setting: Houston Independent School District, elementary schools serving low-income families Design: Cluster RCT of 4 intervention + 4 controls schools • • • Convenience sample Matched schools on race/ethnicity, SES, randomized schools Fourth grade students Center for Child Health, Behavior and Development Houston: WSB trial •20 students, 5 WSB stops •Total distance 1.1 miles Center for Child Health, Behavior and Development Results: Active Commuting % of week using ACS: Intervention vs. Control Intervention Group 29% Control Group 8% *controlling for age, gender, baseline ACS, distance from home Mendoza JA, Watson K, Baranowski T, Nicklas TA, Uscanga DK, Hanfling MJ. The Walking School Bus and Children's Physical Activity: A Pilot Cluster Randomized Controlled Trial. Pediatrics. September 1, 2011 2011;128(3):e537-e544 Center for Child Health, Behavior and Development Results: MVPA Daily MVPA (min): Intervention vs. Control Intervention Group 2 min Control Group 5 min *controlling for age, gender, baseline MVPA, distance from home Mendoza JA, Watson K, Baranowski T, Nicklas TA, Uscanga DK, Hanfling MJ. The Walking School Bus and Children's Physical Activity: A Pilot Cluster Randomized Controlled Trial. Pediatrics. September 1, 2011 2011;128(3):e537-e544 Center for Child Health, Behavior and Development Safe Routes to School • Information on the WSB and other Safe Routes to School programs: • http://guide.saferoutesinfo.org/ • http://guide.saferoutesinfo.org/walking_school_ bus/index.cfm • http://www.saferoutespartnership.org/ Center for Child Health, Behavior and Development Where do we go from here? Center for Child Health, Behavior and Development Call to Action Health care providers, researchers, and institutions as community leaders – advocates for children and families • School board or community organizations • Businesses & chamber of commerce • Community presentations • Input to policy-makers and elected officials • Help create the healthier “default” setting in your own communities! Center for Child Health, Behavior and Development Think outside the box Disease prevention in our communities for children and families • Community-based programs (SRTS) target multiple aspects of health to reduce disease burden and healthcare costs • Likely will have increased relevance once Medicaid Accountable Care Organizations become more prevalent Transformation: hospitals’ community outreach central core of hospitals’ mission for improving patients’ health (expertise, staff, resources) • Affects patients and the hospitals’ bottom line ($$) Center for Child Health, Behavior and Development Pediatric Obesity Screening & Management Center for Child Health, Behavior and Development Pediatric BMI Categories 1. Measure height and weight 2. Calculate BMI 3. Plot on CDC growth chart to obtain BMI percentile • Some EMRs provide automatically • http://nccd.cdc.gov/dnpabmi/Calculator.aspx Barlow S E Pediatrics 2007;120:S164-S192 Center for Child Health, Behavior and Development Universal assessment of obesity risk and steps to prevention and treatment. Barlow S E Pediatrics 2007;120:S164-S192 Center for Child Health, Behavior and Development ©2007 by American Academy of Pediatrics Prevention Plus Basic lifestyle eating and activity habits to improve BMI • More frequent monitoring and visits vs. prevention • 7-5-2-1-0 mnemonic • Involve entire family in lifestyle changes • Child should self-regulate meals, avoid overly restrictive feeding behaviors • Tailor to cultural values Center for Child Health, Behavior and Development Prevention Plus Implementation pointers: • Work w/ families to choose a behavior(s) • Use a stepped approach, e.g. 15 min activity to work up to >60 minutes • Tailor frequency of visits with family • Primary care office and team Center for Child Health, Behavior and Development Prevention Plus Implementation pointers: • If no improvement in 3-6 months, offer/refer Structured Weight Management • • • • • • Dietitian to develop a daily eating plan Motivational interviewing techniques; counselor for parenting skills Physical therapist or exercise therapist Monthly visits Group sessions possible If no improvement in 3-6 months, offer a referral to a Comprehensive Multidisciplinary Intervention (e.g. pediatric weight management center) Center for Child Health, Behavior and Development Lipid management of overweight/obese children Fasting Non-Fasting If abnormal: obtain fasting lipids Figure 2. Published in Childhood Obesity. August 2014, 10(4): 304-317. DOI: 10.1089/chi.2013.0120 Center for Child Health, Behavior and Development Risk Factors for CVD High Risk • Parent/grandparent/uncle/aunt h/o premature CVD (Dx <55 y.o. ♂; 65 y.o. ♀), coronary atherosclerosis, PVD, cerebrovascular disease, or early deaths before 50 y.o. of unknown cause in relatives • BMI ≥ 97th %ile • Type 1 or 2 DM • HTN (bp ≥ 99th %ile + 5 mm Hg, requiring therapy) • Smoker • Chronic renal disease • H/o solid organ kidney or heart transplant • H/o Kawasaki disease w/ current coronary aneurysms Center for Child Health, Behavior and Development LDL management for high risk lipid profiles Published in Childhood Obesity. August 2014, 10(4): 304-317. DOI: 10.1089/chi.2013.0120 Center for Child Health, Behavior and Development Center for Child Health, Behavior and Development Triglyceride management Published in Childhood Obesity. August 2014, 10(4): 304-317. DOI: 10.1089/chi.2013.0120 Center for Child Health, Behavior and Development Evaluation of abnormal liver enzymes Published in Childhood Obesity. August 2014, 10(4): 304-317. DOI: 10.1089/chi.2013.0120 Center for Child Health, Behavior and Development Hypertension evaluation & management Published in Childhood Obesity. August 2014, 10(4): 304-317. DOI: 10.1089/chi.2013.0120 Center for Child Health, Behavior and Development Questions? Center for Child Health, Behavior and Development