Obtaining Useful Information from Pharmaceutical Representatives
advertisement

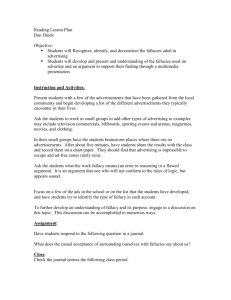
Separating the Wheat from the Chaff Obtaining Useful Information from Pharmaceutical Representatives Based on: Shaughnessy AF, Slawson DC, Bennett JH. Separating the wheat from the chaff: identifying fallacies in pharmaceutical promotion. J Gen Intern Med 1994;9:563-8. The CAGE Questionnaire for Drug Company Dependence • Have you ever prescribed Celebrex ? TM • Do you get Annoyed by people who complain about drug lunches and free gifts? • Is there a medication loGo on the pen you're using right now? • Do you drink your morning Eye-opener out of a Lipitor coffee mug? If you answered yes to 2 or more of the above, you may be drug company dependent. TM Source: www.NoFreeLunch.org Drug Rep Bashing Pharmaceutical Advertising “The best defense the physician can muster against (misleading) advertising is a healthy skepticism and a willingness . . . to do his (sic) homework. He must cultivate a flair for spotting the logical loophole, the invalid clinical trial . . . and the unlikely claim. Above all, he must develop greater resistance to the lure of the fashionable and the new” P.R. Garai, 1964 Drug Advertising • “Promoting drugs to doctors these days is much like selling soap to customers. It’s all in the marketing” – Former CEO of Pfizer, in the Wall Street Journal • Advertising is an unabashed attempt to get someone to buy something. – F. Ingelfinger, former editor of NEJM • Advertising is “the science of arresting the human intelligence long enough to get money from it.” – S. Leacock. The Garden of Folly. ©1924. Drug Advertising • The goal of advertising is to inform, remind, or persuade the target audience • The difference? A select group (clinicians) controls consumption for millions (patients) 3 Drug Advertising • Information alone rarely changes behavior • Provides information, but has to generate an emotional response to work – Pride, fear, anger, ego gratification – all work • Target audience considers themselves rational and critical, requiring special techniques Pharmaceutical Representatives • Education experts • Extremely effective at changing behavior • Advertising budget exceeds entire cost of medical education for USA – a large proportion of this budget is spent on PRs Wolfe SM. J Gen Intern Med 1996;11:637-9. Other Sales Forces: Patients 200 160.8 146 150 125 100 78.2 50 0 Vioxx Budweiser Pepsi Nike Mukherjee D, Topol EJ. Am Heart J 2003;146:563-4. Million Dollars Other Sales Forces: Patients • Goal of DTC advertising: create a sales force of patients • Effective: 40% of patients get prescriptions for the drugs they ask for! Other Sales Forces: Colleagues • Wall Street Journal: “At small meetings, these physicianpitchmen tell their peers about diseases and the drugs to treat them, often pocketing $750 or more from the sponsor.” • 2004; 237,000 physician-led meetings • Speaker training – the new sales method • Trusted colleagues = good sales – Merck: Return on investment twice as high with MD-led discussion groups Hensley S, Martinez B. Wall Street Journal, July 15, 2005 The Evidence • Increased prescribing with increased contact – more costly prescribing – more nonrational prescribing – new drug prescribing – decreased use of generic drugs • More requests for formulary additions – “dose-related” increase with sponsored meals Wazana A. JAMA 2000;283:373-80. The Evidence • Company-sponsored speakers: – increased residents’ inappropriate treatment decisions – occurred even in residents who could not remember the speakers’ affiliations (“under the radar”) • CME: increases prescribing of sponsors’ drugs Wazana A. JAMA 2000;283:373-80. Pharmaceutical Representatives • Excellent source for “Patient-Oriented Evidence that Matters,” especially with an active approach • Experts on drugs they sell – sdf indications, dose, side effects, pharmacokinetics • Cannot provide information on when or for whom Usefulness Score • Validity: Moderate • Relevance: Moderate. Much irrelevant info. • Work: Low If validity or relevance is zero, usefulness is zero Coming to a Theater Near You The Drug Rep Always Rings Twice A 1-act, 6 scene play Based on: Somerset M, et al. Dramaturgical study of meetings between general practitioners and representatives of pharmaceutical companies. BMJ 2001;323:14814. The Plot • Scene 1: The exchange of status – Drug rep acknowledges subordinate status and then proceeds to take a superior role by giving of a present – “Here you go . . . A desk calendar to use. . .” • Scene 2: Introduction of the conflict – Find out what they know. Let them know they are entirely correct but have the potential to do better – “Are you aware of . . . “ The Plot • Scene 3: Bring in the dragon killer – Cite the benefits of the drug, using research evidence and always by mentioning an expert. – “Dr. __ at the university – he’s certainly switching over patients” • Scene 4: Doc takes center stage – The doc brings out his/her own armor to fight off the new information – “Yes, but . . .” The Plot • Scene 5: All glory, laud, and honor – Having created conflict, the drug rep re-establishes empathy with compliments and sympathy – “I know cost is an issue . . . you’re getting a lot of pressure . . .” • Scene 6: The rep sets the hook – Bring out more gifts, try to squeeze out more indebtedness – “Before I go I have something else for you . . .” The “Appeals Process” Correct Correct + Information Reasoning Correct Conclusion See: Johnson RH, Blair JA. Logical Self-Defense. 2nd ed. Toronto: McGraw-Hill Ryerson Limited. 1991. Appeals – Rational/Non Rational • Rational: All relevant information, true facts, sound reasoning connecting facts to conclusion • Non-rational: Fallacy of Logic Non-Rational Appeal • “Cefawhatzitcalled” is effective against 98% of bacteria causing sinusitis • “Cefawhatzitcalled” is the best drug for treating sinusitis • You should use my drug for your patient Fallacies of Logic • • • • • • 6 Appeal to authority Bandwagon effect Red herring Appeal to pity Appeal to curiosity Error of omission Appeal to Authority • “Dr. ____ from ____ University uses this drug” • The fallacy: basing a decision on an authority’s decision, not on the authority’s reason for making the decision Bandwagon Effect • “This is the most prescribed ____ in the U.S.” • The fallacy: – A derivative of the appeal to authority – Not knowing reasons why the drug is the most prescribed – The Ford Escort is the best selling car in the world . . . Red Herring • This drug: – Has a unique carboxyl group on the terminal chain – Is safer in the event the patient also overdoses on acetaminophen (Tylenol) – Penetrates the bacterial cell wall better • The fallacy: interesting (or not) but irrelevant information Appeal to Pity • “Can’t you help me out by trying . . .” • “Doesn’t every patient deserve a trial . . .” • The fallacy: Basing a decision on emotions (pity, wishful thinking), rather than evidence Appeal to Curiosity • “Let me show you this brief demonstration of how our drug works” • “Our antibiotic is a zwitterion . . .” • The fallacy: Similar to the red herring appeal, the demonstration or highlighting of a non-clinical uniqueness captivates the mind Error of Omission • “I’m glad you asked me that question. . .” • The fallacy: Omitting information necessary for making a totally informed decision – STEPS: Safety, Tolerability, Effectiveness, Price, Simplicity Other Techniques • Testimonial – Experts – Self-testimonial 6 Other Techniques • Testimonial • Relationship building – “Face-time” is crucial 6 Other Techniques • Testimonial • Relationship building • Reinforcement – Message comes in “under the radar” – Pens, pads, trinkets – Office survey for reinforcers Shaughnessy AF. JAMA 1988;260:926. 6 Other Techniques • Testimonial • Relationship building • Reinforcement • Cognitive dissonance – Creating – Relieving 6 Other Techniques • Testimonial • Relationship building • Reinforcement • Cognitive dissonance • Food – More receptive to messages while eating Janis I. J Pers Soc Psychol 1965;1:181-6. 6 Other Techniques • Testimonial • Relationship building • Reinforcement • Cognitive dissonance • Food 6 • Gifts Gifts • Acceptance establishes relationship with attendant obligation • Culturally programmed to return “gift” • Goal of advertising- “emotional response” Chren MM, Landefeld CS, Murray TH. doctors, drug companies, and gifts. JAMA 1989;262:3448-3451. Sunshine Policy “What would my patients think if they knew they were paying for this (Cruise on the river, dinner at the Clifton, box seats) ?” AMA Opinion E-8.061 Gifts to Physicians from Industry What Can We Do? • Identifying non-rational does not ensure protection • Common (mis)belief: “can receive . . . and not be influenced” • “. . . implies lack of judgment . . .” • The more unaware, the more vulnerable • Visceral response, not intellectual FDA Commissioner • “An enormous potential exists for misleading advertisement to reach physicians and influence prescribing decisions” -- David Kessler, MD (Kessler DA. Ann Intern Med 1992;116:950-1). • Proving information is secondary goal, primary goal is to sell product – 12% of statements incorrect, easily correctable – one fourth of clinicians aware Ziegler MG. JAMA 1995;273:1296-8. Taking the right “STEPS” when evaluating new information S= T= Safety Tolerability look for “pooled drop-out rates” E= Effectiveness -- Studies showing that the new drug is better than your current choice examples: aspirin vs tPA in acute stroke, adequate vitamin D dose to prevent fractures. P= S= Price Simplicity of use Preskorn SH. Advances in antidepressant therapy: the pharmacologic basis. San Antonio: Dannemiller Memorial Educational Foundation, 1994 STEPS- Clinical Example Should ezetimibe be used to treat hypercholesterolemia? Safety: • No safety issues • No rhabdomyolysis in comb. with statins STEPS- Clinical Example Tolerability: • No particular issues • Pooled dropout rate 5% (= placebo) STEPS- Clinical Example Effectiveness: • LDL-C 18-25% when used alone • Ezetimibe + 10 mg simvastatin: LDL-C to same degree as higher doses of simvastatin alone • But . . . – No research showing its effectiveness in death, stroke, CV disease – No research in patients with other illnesses STEPS- Clinical Example Price: • $75/month • Less than simvastatin, atorvastatin • Simv. 10 mg + ezetimibe > simvastatin 40 mg (at least now) Simplicity • QD • No dosage adjustments • Can be given with or without food STEP- Clinical Example Should SSRIs be the drug of first choice for the treatment of depression? – Anderson IM, Tomenson BM. Treatment discontinuation with SSRIs compared with tricyclic antidepressants: A meta-analysis. BMJ 1995;310:1433-8. – 62 RCTs, double-blind comparing efficacy and tolerability Measured Outcomes • Efficacy: Hamilton Depression Rating scale • Tolerability: Pooled drop-out rates Results • Efficacy: favored Tricyclics • Tolerability: favored SSRIs – drop-out rates nearly equal, 30.8% vs 33.4% • NNT 10 vs 9 • What about safety? – suicide rates equal • Price: Large difference, but need to consider total cost of care Information Mastery • Rely on PR for data, not decisions • Look for “Patient-Oriented Evidence that Matters”, the reasons to choose one drug over another – STEPS 4 • Take responsibility for validity • Take active approach, teach PR your needs Pharm Rep Curriculum: The Process PR Given Appointment Evaluation Process Explained PR Presents Information During 1st half of Lunch Conference Representative Leaves, Residents Complete Evaluation The Process (continued) Discussion focusing on Process Dubious Info. questioned Sales Techniques Identified Fallacies Pinpointed Conclusions Drawn Feedback Given to Representative