International Literature Search in Cardiology
advertisement

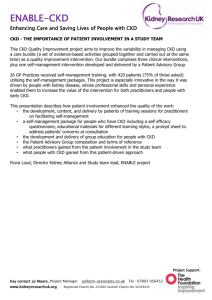
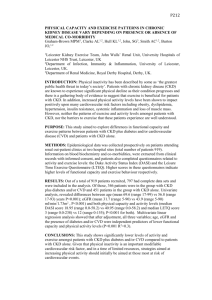
Comprehensive Publication Review: Dyslipidemia, Chronic Kidney Disease and Cardiovascular Disease Table of Contents Author(s) Publication Slides Attman P-O, et al Curr Opin Lipidol 2009 3 – 14 Nogueira J, et al Clin J Am Soc Nephrol 2007 15 – 24 Snyder JJ, et al Am J Nephrol 2009 25 – 32 Levin A, et al CMAJ 2008 33 – 46 Astor BC, et al Am J Epidemiol 2008 47 – 56 Matsushita K, et al Clin Epidemiol 2009 57 – 64 Shepherd J, et al J Am Coll Cardiol 2008 65 – 71 Fellström B, et al N Engl J Med 2009 72 – 78 Nakamura T, et al Pharmacol Res 2009 79 – 86 Türk TR, et al Nephrol Dial Transplant 2008 87 – 95 Baigent C, et al Kidney Int Suppl 2003 96 – 105 Dyslipidemia of Kidney Disease Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Dyslipidemia of Kidney Disease • Objective: To summarize current knowledge of the pathophysiology of renal dyslipidemia and the therapeutic options • Topics covered: – – – – Lipoprotein profile Causes Consequences Therapy Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Background on Dyslipidemia in CKD • With declining renal function, a complex series of various metabolic changes and adaptations occur • In advanced chronic kidney disease (CKD), the lipid profile is characterized by the following: – Markedly elevated triglycerides and triglyceride-rich apoB-containing lipoproteins – Decreased HDL-cholesterol (HDL-C) – Minimal to no change in LDL-cholesterol (HDL-C) • This profile has been linked to high incidence of cardiovascular (CV) morbidity and mortality Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Consequences of Renal Dyslipidemia • Cardiovascular disease (CVD) is the main cause of mortality during dialysis and after renal transplantation • The accelerated development of atherosclerosis and CVD in progressive renal disease is well documented • The prevalence of CVD is also high in renal patients in the early stages of CKD, long before the time of initiating dialysis Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Lipid-lowering Therapy for Renal Dyslipidemia • Lipid-lowering intervention has the theoretical potential to attenuate deleterious processes associated with CKD: – Accelerated atherosclerosis – Progression of renal functional impairment • However, to date, only a few studies have been specifically designed to address these issues Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Post-hoc Analyses of CKD Patients in Major Statin Trials Trial Lipid-lowering Agent Findings CARE Pravastatin HPS Simvastatin VA-HIT Gemfibrozil 4S Simvastatin AFCAPS/TexCAPS TNT Lovastatin Atorvastatin Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. • Both statin and fibrate treatment result in reductions of LDL-C or triglyceride levels or both • Both statin and fibrate treatment reduce the relative risk of CHD and overall CVD morbidity to the same extent as in patients with normal renal function Prospective Studies of Lipidlowering in Stage 4 CKD Trial Lipid-lowering Agent Findings 4D Atorvastatin AURORA Rosuvastatin ALERT Fluvastatin Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. • Statin therapy had no effect on CVD morbidity, all-cause mortality or CV mortality • Subgroup analysis suggested a reduction in the incidence of myocardial infarction (MI) • Extended follow-up (mean 6.7 years) showed that major CV events were significantly reduced Why Aren't Statins Powerfully Effective in Stage 4 CKD? • Statins are not very effective in reducing triglyceride-rich apoB- and apoC-containing lipoproteins • This is the major lipoprotein abnormality of advanced renal failure • We should therefore not expect statins to significantly attenuate renal dyslipidemia in advanced CKD Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Ongoing Studies of Lipid-lowering in CKD Full study title Treatments Primary outcome variable SHARP LORD Study of Heart and Renal Protection Lipid lowering and Onset of Renal Disease Simvastatin + ezetimibe vs. placebo Atorvastatin vs. placebo CVD morbidity Progression of kidney disease Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Attenuation of Progression of Renal Disease? • The TNT study (patients with coronary heart disease [CHD] ± CKD) suggested that high-dose atorvastatin seemed to be beneficial, increasing eGFR by ~ 1 mL/min • Meta-analyses based on small studies have suggested a positive effect of statin treatment on the progression of CKD • However: – Post-hoc analyses of larger lipid-lowering intervention trials have failed to show benefit or have been inconclusive – Confounding effects of concomitant antihypertensive therapy cannot be ruled out • The impact of lipid-lowering therapy on progression of renal disease remains to be established Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Risk Reduction with Statins in Renal Dyslipidemia Cardiovascular risk reduction by statins? GFR 100 Renoprotection by statins? 50 Adapted from Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. Dyslipidemia of Kidney Disease: Conclusions • Recent studies have shown important pathophysiological links between an increase of apoC-III-containing lipoproteins and the inflammatory processes that ultimately can result in accelerated vascular disease in CKD patients • For stage 1–3 CKD patients, lipid-lowering interventions should be beneficial – Further research is required for definitive answers • Statin treatment cannot reduce CVD in patients with renal failure on hemodialysis Attman PO, et al: Curr Opin Lipidol 2009; 20(4):293-9. The Unique Character of CVD in CKD and Its Implications for Treatment with Lipid-lowering Drugs Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. CVD in CKD: Implications for Lipid-lowering Treatment • Background: – There are very limited data to guide the use of lipidlowering drugs in CKD – Data from trials in the general population may not be generalizable to those with CKD • Objectives: – To review the data that are pertinent to the CKD population – To update recommendations for use of lipid-lowering therapy in the CKD population Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Evidence for Lipid-lowering Therapy in CKD: Subgroup Analyses of Major Trials Study n Results Comments Pravastatin 4491 patients with pooling project eGFR 30-60 mL/min Pravastatin reduced risk Suggested benefit in of composite endpoint secondary prevention (time to MI, coronary setting death or revascularization; HR 0.77) Heart Protection Study 375 patients with serum creatinine 1.25 – 2.28 mg/dL (women), 1.48 – 2.28 mg/dL (men) Simvastatin reduced risk Supports benefit of of first major vascular treatment with statins event (HR 0.70) in relatively mild CKD ASCOT-LLA 6517 hypertensive adults with undefined "renal dysfunction" Atorvastatin lowered the Further supports a risk of nonfatal MI and role for statins in fatal CHD (HR 0.61) relatively mild CKD Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Completed Prospective Trials of Lipid-lowering Therapy in CKD Study n Results Comments ALERT 2102 renal transplant recipients No significant risk reduction for major adverse cardiac events Trial had insufficient power to detect primary endpoint difference 4-D 1255 hemodialysis patients with type 2 diabetes No significant risk reduction in composite of cardiac death, nonfatal MI, stroke Perhaps a higher dose of statin may have produced benefit PREVEND-IT 864 patients with microalbuminuria, creatinine clearance > 60% of normal No significant risk reduction in CV mortality or hospitalization for CV morbidity Study was unable to show a benefit of statin therapy early in the CKD spectrum UK-HARP-1* 448 patients with later-stage CKD (predialysis, dialysis or post-transplant) Statins produced sustained reduction in LDL with no evidence of toxicity Provides support for the safety of statins in CKD *Precursor to the larger SHARP study, currently ongoing. Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Potential Contributors to the Development of CVD in Patients with CKD Common to General Population Unique or Relatively Much More Important to the CD Population Aging Oxidative stress Volume overload High LDL-C Inflammation Anemia Low HDL-C Malnutrition Rapid volume changes with HD Hypertension Vascular calcification Rapid electrolyte changes in HD Diabetes Uremic cellular metabolic derangements Immunosuppressant drugs in transplantation Tobacco use LDL oxidation Endothelial dysfunction Physical inactivity Hypertriglyceridemia Altered nitric oxide balance Familial/inherited predisposition High IDL-C Advanced glycation end products Postmenopausal hormone changes Left ventricular hypertrophy Coagulation abnormalities Hyperhomocysteinemia Sleep disturbances Hyperuricemia Sympathetic overactivity Carnitine deficiency Cardiac microvessel disease Leptin Arrhythmic sudden death Recurrent intradialytic hypotension HD: hemodialysis; IDL: intermediate-density lipoprotein Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Alterations in Lipid Profiles in CKD Generally Increased Levels Generally Decreased Levels Triglycerids Lipoprotein(a) Apoprotein B VLDL-C IDL-C Total cholesterol LDL-C HDL-C Apoprotein A1 Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Updated Recommendations for Lipid-lowering Therapy in CKD • It is advisable to aggressively treat individuals who have an eGFR of 30 to 60 mL/min/1.73 m2 and have known CHD and probably those without known coronary disease – On the basis of the findings from the Pravastatin Pooling Project • It is reasonable to apply the currently accepted and footnoted guidelines (NCEP ATP-III) schema for treatment on the basis of LDL-C levels and LDL-C goals to those who have not yet reached end-stage renal disease (ESRD) Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Updated Recommendations for Lipid-lowering Therapy in CKD • It may be advisable to treat those with high risk for atherosclerotic cardiac events regardless of initial LDL level to achieve a marked (at least 30 to 40%) reduction in LDL • A lower goal LDL of 70 mg/dL may be a reasonable therapeutic option in patients with CKD • The increase in mortality in hemodialysis patients at lower cholesterol levels demands caution within this population Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. Updated Recommendations for Lipid-lowering Therapy in CKD • It is reasonable but not mandatory to consider a reduced GFR, proteinuria, and perhaps microalbuminuria to be a “CHD-risk equivalent” • Routine treatment of hemodialysis patients with diabetes may not be warranted • Ezetimibe is a reasonable choice for a second-line lipid-lowering therapy in the CKD population and probably in kidney transplant recipients Adapted from Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. CVD in CKD and Implications for Lipidlowering Treatment: Conclusions • As the severity and duration of uremia increase, the epidemiology, pathophysiology and response to treatment of CVD changes gradually from what is experienced in the general population to what is unique to the uremic milieu – It becomes much less clear whether lipid-lowering agents are of benefit as CKD advances, especially in dialysis patients • There is great potential for benefit of statins and other lipid-lowering agents in this population, but the need for further study is urgent Nogueira J, et al: Clin J Am Soc Nephrol 2007; 2(4):766-85. KDOQI Hypertension, Dyslipidemia, and Diabetes Care Guidelines and Current Care Patterns in the United States CKD Population: National Health and Nutrition Examination Survey 1999-2004 Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Hypertension, Dyslipidemia and Diabetes Care in CKD • Objective: To assess current CKD population health and adherence to recommendations in the United States • Subjects: 14,213 patients with CKD, aged ≥20 years – From the National Health and Nutrition Examination Survey 1999-2004 • Assessments: Rates of hypertension and dyslipidemia management and diabetes control, stratified by CKD status and prior history of CVD Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Background • The US National Kidney Foundation published a series of guidelines in the 2000s – Aim was to slow CKD progression and reduce morbidity and mortality • CKD patients are more than 6 times more likely to die from CVD than to reach ESRD • Understanding of adherence to guidelines for CVD risk factors is crucial to evaluating overall health of these patients Adapted from Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Measured LDL-C Levels, by Stage of CKD % 100 90 80 70 3% 10% 24% 3% 10% 26% 4% 9% 24% 35% 31% 32% 40 20 0 Borderline high, 130-159 mg/dL Near optimal, 100-129 mg/dL 30 10 Very high, ≥190 mg/dL High, 160-189 mg/dL 60 50 ATC III cholesterol classification 28% 30% 31% None Stage 1 – 2 Stage 3 – 4 CKD stage Adapted from Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Optimal, <100 L High Cholesterol: Prevalence, Awareness, Treatment and Control No prior CVD No CKD High LDL-C prevalence1 Prior CVD CKD CKD stages 1-2 stages 3-4 No CKD CKD CKD stages 1-2 stages 3-4 32 46 81 90 84 83 Unaware 38 40 53 35 37 33 Aware, untreated 10 9 10 9 8 4 Aware, treated, not controlled 21 26 10 35 37 37 Aware, treated, controlled 31 26 11 21 18 26 Within HDL target range2 81 76 81 69 73 76 Lipid-lowering agent use3 20 21 22 41 48 55 High cholesterol Values are %. CKD = Chronic kidney disease; LDL = low-density lipoprotein; HDL = high-density lipoprotein. 1 Taking lipid-lowering agents, dieting, or not meeting National Cholesterol Education Program Adult Treatment Panel III LDL cholesterol targets. 2. National Cholesterol Education Program Adult Treatment Panel III, ≥40 mg/dL. Unadjusted. 3. Unadjusted Adapted from Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Odds Ratios for Control of High Cholesterol by CKD Stage: No History of CVD Reference: non-CKD = 1 High cholesterol* Awareness* Treatment* Control* LLA use 0.2 0.6 1.4 2.6 Odds ratio (log scale) *Significant interaction between history of CVD and CKD stage Adapted from Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. 5.0 CKD stage OR 1–2 1.25 3–4 5.03 1–2 0.89 3–4 0.35 1–2 0.89 3–4 0.39 1–2 0.75 3–4 0.14 1–2 0.90 3–4 0.84 Odds Ratios for Control of High Cholesterol by CKD Stage: History of CVD Reference: non-CKD = 1 High cholesterol* Awareness* Treatment* Control* LLA use 0.2 0.6 1.4 2.6 Odds ratio (log scale) *Significant interaction between history of CVD and CKD stage Adapted from Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. 5.0 CKD stage OR 1–2 0.41 3–4 0.39 1–2 0.75 3–4 0.85 1–2 0.75 3–4 1.02 1–2 1.28 3–4 1.69 1–2 0.90 3–4 0.84 Dyslipidemia in CKD: Conclusions • The U.S. National Kidney Foundation has identified many target areas for preventative care in the CKD population – Identifying risk factors such as dyslipidemia could improve morbidity and mortality • In later stage CKD, those with reported CVD history were more likely to be aware of, treated for, and in control of high cholesterol than those without CVD • Participants with CKD stages 1–2 were less likely to have controlled cholesterol if they had reported CVD history – This represents a care gap for earlier-stage patients – Further research is warranted to investigate these differences • There are many opportunities for improvement in the management of patients with CKD Snyder JJ, et al: Am J Nephrol 2009; 30(1):44-54. Guidelines for the Management of CKD Levin A, et al: CMAJ 2008; 179(11):1154-62. Review of Canadian Guidelines for the Management of CKD • Objective: To outline evidence-based recommendations from the Canadian Society of Nephrology guidelines on aspects of management of CKD • Topics covered: – Targets for various abnormalities – Strategies for treatment – Frequency of follow-up • Focus: For the purposes of this document, the focus is on CV abnormalities, specifically dyslipidemia Levin A, et al: CMAJ 2008; 179(11):1154-62. A Few Notes About the Canadian Guidelines for the Management of CKD • The recommendations are meant for pre-dialysis patients only • The target audience includes both general practitioners and specialists • The guidelines are part of a comprehensive national strategy management • The recommendations are aligned with guidelines of other national societies (e.g., Canadian Diabetes Association, Canadian Hypertension Education Program and Canadian Cardiovascular Society) Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Definition of CKD • The presence of kidney damage for a period greater than 3 months • Abnormal kidney function is noted if: – Estimated / measured GFR <60 mL/min/1.73 m2 – Estimated / measured GFR >60 mL/min/1.73 m2, accompanied by: • Abnormalities of urine sediment; or • Abnormal results of imaging tests; or • If the patient has had a kidney biopsy with documented abnormalities Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. CKD and CVD • CKD is estimated to affect between 1.9 million and 2.3 million Canadians – This is a major public health problem • CKD often coexists with CVD and diabetes – CKD is recognized as a risk factor for all-cause mortality and CVD – Most patients with CKD will die of events related to CVD before ESRD develops – An important focus of care for patients with CKD includes management of CVD risk factors Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Stages of CKD* Stage Description GFR, mL/min/1.73 m2 1 Kidney damage† with normal or increased GFR ≥90 2 Kidney damage† with mild decreased GFR 60–89 3 Moderately decreased GFR 30–59 4 Severely decreased GFR 15–29 5 Kidney failure <15 (or dialysis) * Kidney damage or GFR less than 60 mL/min/1.73 m 2 for 3 or more months. † Pathologic abnormalities or markers of damage, including persistent proteinuria, abnormalities in urine sediment (persistent presence of erythrocytes, erythrocyte casts, leukocytes or leukocyte casts) or abnormal results in imaging studies (evidence of scarring or small kidneys on ultrasound or bilateral cystic changes consistent with polycystic kidney disease) Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Canadian CKD Guidelines: Shared Care Is Recommended • The guidelines were developed to facilitate shared care of patients with CKD by GPs and specialists (including internists, endocrinologists, cardiologists and nephrologists) • Most cases of nonprogressive CKD can be managed in primary care without referral to a nephrologist Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Scenarios in Which Referral to a Nephrologist Should Be Considered • Acute kidney failure • Persistent eGFR <30 mL/min/1.73 m2 • Progressive decline of kidney function • Ratio of urine protein to creatinine >100 mg/mmol (about 900 mg/24 h) • Urine albumin to creatinine ratio >60 mg/mmol (about 500 mg/24 h) • Inability to achieve treatment targets • Rapid changes in kidney function Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Recommendations for Screening for Dyslipidemia in CKD • A fasting lipid profile (total cholesterol, LDL-C, HDL-C and triglyceride) should be measured in adults with stage 1–3 CKD • A fasting lipid profile should be measured in adults with stage 4 CKD only if the results would influence the decision to initiate or alter lipid-modifying treatment Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Canadian CKD Guidelines: Recognition of Common Comorbidities and Risk Factors • Groups at particular risk of developing CKD: – – – – CVD Diabetes Specific ethnicities Family history of CKD • There is a high prevalence of dyslipidemia at every stage of CKD Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Recommendations for Monitoring Dyslipidemia in CKD • Lipid profiles should be measured after an overnight fast (ideally ≥12 h duration) • Total cholesterol, LDL-C, HDL-C and triglycerides should be measured • Fasting lipid profiles should be measured no sooner than 6 weeks after initiation or change in pharmacologic therapy • Thereafter, lipid profiles should be monitored every 6–12 months if the results could influence subsequent therapeutic decisions Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Recommendations for LDL Lowering in CKD Stage of CKD Recommendations • Statin therapy should be initiated according to existing lipid guidelines for the general population Stages 1–3 • Clinicians should consider titrating the dose of statin according to lipid guidelines for the general population Stage 4 • Clinicians should consider initiating statin therapy for patients with stage 4 CKD and titrating the dose to achieve an LDL-C level <2.0 mmol/L and a ratio of total cholesterol to HDL-C <4.0 Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Recommendations for Monitoring for Adverse Effects of Medication • Serial monitoring of creatinine kinase and alanine aminotransferase: – Not required for asymptomatic patients with CKD taking a low to moderate dose of statin (≤20 mg/d of simvastatin or atorvastatin, or an equivalent dose of another statin) – Should be measured every 3 months for patients with stage 4 CKD who are taking a moderate to high dose of statin (≥40 mg/d of simvastatin or atorvastatin, or an equivalent dose of another statin) • A statin and fibrate should not be coadministered to patients with stage 4 CKD because of the risk of rhabdomyolysis Adapted from Levin A, et al: CMAJ 2008; 179(11):1154-62. Guidelines for the Management of CKD: Conclusions • The complexity of CKD clearly requires a better understanding of the absolute and relative value of identifying and treating the myriad clinical and laboratory abnormalities • It is critical that we better define the importance of these conditions for each stage of CKD • We must ensure that patients with CKD and any other risk factor for CVD receive aggressive treatment, and that a sense of therapeutic nihilism does not overcome our judgment and clinical care • The lack of evidence should encourage us to advocate for the design of and enrolment into randomized control trials that answer questions relevant to this population Levin A, et al: CMAJ 2008; 179(11):1154-62. GFR, Albuminuria and Risk of Cardiovascular and All-cause Mortality in the US Population Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34 GFR, Albuminuria and the Risk of CV and All-cause Mortality in the US Population • Objective: To evaluate the separate and combined effects of decreased GFR and albuminuria on CV and all-cause mortality • Subjects: 14,586 adults from NHANES III • Methodology: – GFR was estimated from standardized serum creatinine levels – Albuminuria was defined by the urinary albumincreatinine ratio – Incidence rate ratios for mortality were adjusted for major CVD risk factors and C-reactive protein (CRP) Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. GFR, Albuminuria and the Risk of CV and All-cause Mortality: Background • Patients with CKD are much more likely to die of CVD than to experience kidney failure • Experts have recommended using CKD in CV-risk stratification and treatment guidelines • Defining and staging kidney disease relies on combining information on kidney damage and decreased renal filtration – Most prospective studies examine one or the other, but not both • The risk associated with varying levels of albuminuria by level of kidney function has not been quantified in large cohort studies Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. GFR, Proteinuria and CV Risk • Lower GFR predicts CV events and mortality in: – Patients with existing CVD – Patients at high risk of CVD – The general population • Leakage of protein in the urine (proteinuria or albuminuria) is a sensitive indicator of: – Early kidney damage (especially in diabetes) – GFR decline – Higher risk of CVD and mortality Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. Differences in Demographic Characteristics by Baseline eGFR (1 of 3) Total Estimated Mean GFR (mL/min/1.73m2) ≥ 90 60-89 15-59 p value Mean age, yrs 44.2 38.5 52.8 70.4 < 0.001 Female sex, % 52.1 51.4 52.5 60.7 < 0.001 Race / ethnicity, % < 0.001 Non-Hispanic White 76.0 70.6 86.1 86.5 Non-Hispanic Black 11.1 13.6 6.2 8.3 Mexican-American 5.2 6.8 2.3 1.3 Other 7.7 9.0 5.4 4.9 Diabetes, % 4.8 3.4 6.2 15.8 Prevalent CHD, % 7.6 4.1 10.9 38.4 Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. <0.001 Differences in Demographic Characteristics by Baseline eGFR (2 of 3) Total Estimated Mean GFR (mL/min/1.73m2) ≥90 60–89 15–59 Hypertension category, % p value <0.001 Optimal 47.1 54.4 36.1 13.3 Prehypertension 34.9 33.6 37.9 32.0 Stage 1 hypertension 13.4 9.6 18.9 33.3 Stage 2 hypertension 4.6 2.4 7.1 21.4 Use of antihypertensive medication, % 12.7 6.8 17.9 52.3 Smoking status <0.001 <0.001 Never smoker 45.7 45.3 46.5 44.6 Former smoker 25.8 21.3 33.3 41.6 Current smoker 28.5 33.4 20.2 13.9 Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. Differences in Demographic Characteristics by Baseline eGFR (3 of 3) Total Body mass index, kg/m2 26.5 Estimated Mean GFR (mL/min/1.73m2) ≥90 60–89 15–59 26.2 27.1 27.6 Physical activity, % p value <0.001 <0.001 Inactive 25.1 25.7 22.6 34.4 Moderately active 53.6 51.4 57.6 58.1 Active 21.3 22.9 19.8 7.5 LDL-C level (mg/dL) 123.5 118.4 131.6 144.1 0.003 HDL-C level (mg/dL) 50.8 51.0 50.5 48.9 0.005 Triglyceride level (mg/dL) 145.9 139.1 153.9 194.6 <0.001 C-reactive protein level 0.002 <0.22 mg/dL 71.5 73.7 69.6 51.6 0.22–0.99 mg/dL 21.1 19.6 22.8 31.7 ≥1.0 mg/dL 7.4 6.7 7.6 16.7 Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. Adjusted Incidence Rates of CV Mortality, by Kidney Function 5 Adjusted incidence rate (per 100 person-years) Normal 4 Microalbuminuria Marcoalbuminuria 3 2 1 0 >90 60–89 Estimated GFR (mL/minute/173 m2) Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. 15–59 Adjusted Incidence Rates of Allcause Mortality, by Kidney Function 10 Adjusted incidence rate (per 100 person-years) Normal 8 Microalbuminuria Macroalbuminuria 6 4 2 0 >90 60–89 Estimated GFR (mL/minute/173 m2) Adapted from Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. 15–59 GFR, Albuminuria and the Risk of CV and All-cause Mortality: Conclusions • Lower eGFR and higher urinary ACR independently predict CV and all-cause mortality – The presence of both abnormalities confers even greater risk – Elevated risks remained strong after adjustment for potential confounders – Similar results were seen among persons with and without diabetes • These data support the use of CKD in risk stratification and treatment guidelines • The reasons for the increased risk of CVD in CKD are not fully understood – Persons with CKD have a higher prevalence of several CVD risk factors, including dyslipidemia Astor BC, et al: Am J Epidemiol 2008; 167(10):1226-34. Change in eGFR Associates with CHD and mortality Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Background: Rationale for the Study • There are many studies documenting an independent association between baseline kidney function and future CV events • Little is known about the impact of sequential changes in kidney function on future CV risk • There is some evidence that suggests that: – Deterioration in kidney function is associated with CVD – Change in kidney function may be a better CV risk marker than baseline kidney function Adapted from Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Impact of Changes in eGFR Over Time on CHD and Mortality • Objective: To investigate whether changes in eGFR associated with risk for CHD and all-cause mortality • Subjects: 13,029 participants of the Atherosclerosis Risk in Communities (ARIC) Study • Methodology: – The investigator examined the impact of both intermediate (3-year) and long-term (9-year) changes in eGFR – Results were also analyzed after adjustment for covariates Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Annual Change in eGFR from Baseline to Year 3 .10 Density .08 .06 .04 .02 0 -60 -50 -40 -30 -20 -10 0 10 20 30 % annual change in eGFR between visit 1and visit 2 Adapted from Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. 40 Characteristics of Patients with Largest Declines in eGFR • Participants with the largest declines in eGFR: – Were more likely to be women – Were more likely to be black – Had higher average systolic BP but lower LDL-C and higher HDL-C than patients with more stable eGFR – Had the highest mean baseline eGFR Adapted from Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Adjusted Incidence Rates for CHD by Quartiles of % Annual Change in eGFR Adjusted incidence rate of CHD per 1,000 person-years 25 20 15 10 3-year change 5 9-year change 0 Q1 Q2 Q3 Quartiles of % annual change in eGFR Adapted from Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Q4 Adjusted Incidence Rates for All-cause Mortality by Quartiles of % Annual Change in eGFR Adjusted incidence rate of all-cause mortality per 1,000 person-years 25 20 15 10 3-year change 5 9-year change 0 Q1 Q2 Q3 Quartiles of % annual change in eGFR Adapted from Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Q4 Impact of Changes in eGFR Over Time on CHD and Mortality: Conclusions • A steeper than average decline in eGFR (i.e., >5%/year) was associated with a higher risk for all-cause mortality independent of eGFR and other known risk factors at baseline or follow-up – This was more relevant for individuals with mildly or moderately reduced eGFR (30 to 89 mL/min per 1.73m2) • The results after adjustment for covariates suggests the observed effect is independent of the deterioration in traditional risk factors • There may be clinical value in sequential eGFR data, often measured in routine care, even among individuals with mildly reduced eGFR • The causative mechanisms by which impaired kidney function contributes to CHD and other causes of mortality are not fully elucidated Matsushita K, et al: J Am Soc Nephrol 2009; 20(12):2617-24. Intensive Lipid Lowering with Atorvastatin in Patients with CHD and CKD: the TNT Study Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Intensive Statin Therapy in Patients with CHD and CKD (TNT Sub-analysis) • Objective: To investigate the effects of intensive lipid lowering with atorvastatin in patients with CHD, with and without pre-existing CKD • Subjects: 10,001 patients with established CHD – Including 3107 patients with mild-to-moderate CKD – Post-hoc subanalysis of the TNT study • Methodology: – Subjects were randomized to double-blind therapy with atorvastatin 80 mg/day or 10 mg/day – Patients with CKD were identified at baseline by eGFR (Modification of Diet in Renal Disease [MDRD] equation) <60 mL/min/1.73 m2 – Primary efficacy outcome: Time to first major CV event Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Observations About Baseline Characteristics • Patients with CKD were older, and there were more women and fewer smokers than among patients with normal eGFR • Pre-existing CV morbidity at baseline was generally greater in patients with CKD than in patients with normal eGFR • There were no imbalances in baseline characteristics by randomized treatment assignment Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Time to First Major CV Event Among Patients with CKD at Baseline 20 % of patients with major CV events Patients with CKD at baseline Atorvastatin 10 mg Atorvastatin 80 mg 15 HR=0.68 (95% CI 0.55, 0.84) P=0.0003, ARR=4.1%, NNT=24 10 5 0 0 No. of CKD patients at risk Atorva 10 mg 1505 Atorva 80 mg 1602 1 2 3 Time (Years) 4 5 6 1468 1579 1422 1539 1367 1495 1310 1450 687 701 0 0 Adapted from Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Time to First Major CV Event Among Patients with no CKD at Baseline 20 % of patients with major CV events Patients with normal eGFR at baseline Atorvastatin 10 mg Atorvastatin 80 mg 15 HR=0.85 (95% CI 0.72, 1.00) P=0.049, ARR=1.4%, NNT=74 10 5 0 0 No. of CKD patients at risk Atorva 10 mg 3324 Atorva 80 mg 3225 1 2 3 Time (Years) 4 5 6 3263 3180 3192 3113 3114 3044 3036 2963 1557 1579 0 0 Adapted from Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Primary and Secondary Event Rates in Patients with CKD and Patients with Normal eGFR P-value for heterogeneity Event rate 80 mg 10 mg Major cardiovascular event All Patients* Patients with CKD Patients with normal eGFR 434 (8.7%) 149 (9.3%) 254 (7.9%) 548 (10.9%) 202 (13.4%) 307 (9.2%) P=0.113 1405 (28.1%) 489 (30.5%) 857 (26.6%) 1677 (33.5%) 574 (38.1%) 1027 (30.9%) P=0.225 334 (6.7%) 110 (6.9%) 198 (6.1%) 418 (8.3%) 157 (10.4%) 226 (6.8%) P=0.040 1078 (21.6%) 356 (22.2%) 676 (21.0%) 1326 (26.5%) 431 (28.6%) 828 (24.9%) P=0.285 196 (3.9%) 74 (4.6%) 111 (3.4%) 250 (5.0%) 104 (6.9%) 139 (4.2%) P=0.281 122 (2.4%) 49 (3.1%) 71 (2.2%) 164 (3.3%) 84 (5.6%) 72 (2.2%) P=0.011 275 (5.5%) 121 (7.6%) 147 (4.6%) 285 (5.6%) 112 (7.4%) 160 (4.8%) P=0.629 284 (5.7%) 112 (7.0%) 132 (4.1%) 282 (5.6%) 113 (7.5%) 124 (3.7%) P=0.401 Any cardiovascular event All Patients* Patients with CKD Patients with normal eGFR Major coronary event All Patients* Patients with CKD Patients with normal eGFR Any coronary event All Patients* Patients with CKD Patients with normal eGFR Cerebrovascular event All Patients* Patients with CKD Patients with normal eGFR CHF with hospitalization All Patients* Patients with CKD Patients with normal eGFR Peripheral artery disease All Patients* Patients with CKD Patients with normal eGFR All-cause mortality All Patients* Patients with CKD Patients with normal eGFR 0.4 0.6 0.8 1.0 1.2 1.4 1.6 Hazard ratio (95% CI) Atorvastatin 80 mg better Atorvastatin 10 mg better Adapted from Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Intensive Statin Therapy in Patients with CHD and CKD : Conclusions • This post-hoc analysis of the TNT study extends the CV benefit of aggressively lowering LDL-C to a highrisk patient population with mild-to-moderate CKD and stable CHD • Patients with CHD and mild-to-moderate CKD may differ from those with more advanced renal failure or ESRD • These data support the use of high-dose statin therapy to achieve lower target LDL-C levels for optimal prevention of CV events in high-risk patient groups • CKD should not preclude use of a statin Shepherd J, et al: J Am Coll Cardiol 2008; 51(15):1448-54. Rosuvastatin and CV Events in Patients Undergoing Hemodialysis Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Rosuvastatin and CV Events in Patients Undergoing Hemodialysis (The AURORA Study) • Objective: To determine whether statins reduce the incidence of CV events in patients undergoing hemodialysis • Subjects: 2776 patients, 50 to 80 years of age, undergoing maintenance hemodialysis • Methodology: – Subjects were randomly assigned to receive rosuvastatin 10 mg daily or placebo – Combined primary end point: CV death, nonfatal MI or nonfatal stroke Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Mean Change in LDL-C 120 Placebo 100 Mean LDL-C (mg/dl) 80 60 Rosuvastatin 40 20 0 0 No. at risk Placebo 1372 Rosuvastatin 1375 1 2 3 4 5 543 553 298 315 70 61 Year 1248 1243 1005 994 719 719 Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Rosuvastatin vs. Placebo: Primary Composite Endpoint Cumulative incidence of the primary end point (%) 40 35 Placebo 30 Rosuvastatin 25 20 15 Hazard ratio, 0.96 P=0.59 10 5 0 0 No. at risk Placebo 1384 Rosuvastatin 1390 1 2 3 4 5 809 826 534 551 153 148 Year 1163 1152 952 962 Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Rosuvastatin vs. Placebo: Components of the Primary Endpoint Rosuvastatin (n=1389) Event CV death Nonfatal MI Nonfatal stroke No. of pts. 324 91 53 No. of events / 100 pt-yrs 7.2 2.1 1.2 Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Placebo (n=1384) No. of pts. 324 107 45 HR (95%CI) p value 7.3 1.00 (0.851.16) 0.97 2.5 0.84 (0.641.11) 0.23 1.1 1.17 (0.791.75) 0.42 No. of events / 100 pt-yrs Rosuvastatin vs. Placebo: Adverse Events No. of patients (%) Adverse events (AEs) p value Rosuvastatin (n=1389) Placebo (n=1384) Any AE 1338 (96.3) 1332 (96.7) 0.56 Any serious AE 1140 (82.1) 1159 (84.1) 0.80 Serious AE requiring permanent discontinuation of study drug 438 (31.5 442 (32.1) 0.78 AE leading to death 640 (46.1) 662 (48.0) 0.49 Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Rosuvastatin and CV Events in Patients Undergoing Hemodialysis: Conclusions • In patients undergoing hemodialysis, the initiation of treatment with rosuvastatin: – Lowered the LDL-C level – Lowered the concentration of hsCRP – Had no significant effect on the composite primary end point of death from CV causes, nonfatal MI or nonfatal stroke • The trial did not meet its primary endpoint Fellström BC, et al: N Engl J Med 2009; 360(14):1395-407. Co-administration of Ezetimibe Enhances Proteinuria-lowering Effects of Pitavastatin in CKD Patients Partly Via a Cholesterol-independent Manner Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Renoprotection with Ezetimibe in Nondiabetic CKD Patients with Dyslipidemia • Objective: To investigate whether coadministration of ezetimibe with pitavastatin could augment renoprotective properties of pitavastatin • Subjects: 20 non-diabetic patients with stage 1 or 2 CKD and dyslipidemia • Methodology: – Patients were randomly assigned to either 2 mg pitavastatin once or 2 mg pitavastatin + 10 mg ezetimibe once daily – Assessments: Effects of therapy on plasma lipids and on proteinuria Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Reduction in Total Cholesterol with Pitavastatin ± Ezetimibe Total cholesterol (mg/dL) 300 250 Pitavastatin 2 mg 243,6 Pitavastatin 2 mg + ezetimibe 10 mg 239,0 200 172,2 150 154,2 100 50 0 Before treatment Adapted from Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. After treatment Reduction in LDL-C with Pitavastatin ± Ezetimibe 180 167,9 160 162,6 LDL-C (mg/dL) 140 120 97,9 100 80 82,2 60 40 20 0 Before treatment After treatment Adapted from Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Reduction in Serum ADMA Levels with Pitavastatin ± Ezetimibe 0,62 Pitavastatin 2 mg 0,60 Serum ADMA (nmol/mL) 0,60 0,58 Pitavastatin 2 mg + ezetimibe 10 mg 0,59 0,56 0,54 0,52 0,52 0,51 0,50 0,48 0,46 Before treatment After treatment Adapted from Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Reduction in Proteinuria with Pitavastatin ± Ezetimibe 1600 Proteinuria (mg/d) 1400 1512 1508 Pitavastatin 2 mg Pitavastatin 2 mg + ezetimibe 10 mg 1200 1042 1000 800 786 600 400 200 0 Before treatment Adapted from Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. After treatment Discussion: Cholesterolindependent Effects of Ezetimibe • These findings support previous studies, which found that: – Ezetimibe decreased serum ADMA levels and improved renal damage in non-diabetic stage 1 – 2 CKD patients with dyslipidemia in a cholesterolindependent manner • Possible mechanisms of ezetimibe benefit on renal parameters: – Anti-oxidative properties – Direct effect on endothelial function Adapted from Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Ezetimibe in Non-diabetic CKD Patients with Dyslipidemia: Conclusions • Co-administration of ezetimibe enhanced proteinuria-lowering effects of pitavastatin in nondiabetic CKD patients, partly via a cholesterolindependent manner • Ezetimibe may have pleiotropic actions that could contribute to renoprotective properties of this lipidlowering agent Nakamura T, et al: Pharmacol Res 2009 Aug 8. [Epub ahead of print]. Ezetimibe Treatment in Hypercholesterolemic Kidney Transplant Patients is Safe and Effective and Reduces the Decline of Renal Allograft Function: a Pilot Study Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Ezetimibe in Hypercholesterolemic Kidney Transplant Patients: Background • Ezetimibe has shown efficacy in the treatment of hypercholesterolemia in renal transplant patients • This is the first study investigating the effect of ezetimibe on renal function in kidney transplant recipients Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Ezetimibe in Hypercholesterolemic Kidney Transplant Patients • Objective: To prospectively investigate the effect of ezetimibe on renal function in kidney transplant recipients • Subjects: 56 patients with statin-resistant hypercholesterolemia (total cholesterol >200 mg/dL) after renal transplantation • Methodology: – Study patients received additional ezetimibe therapy (10 mg/day) for 12 months (n=56) – A group receiving statin therapy (n=28) alone served as controls – Investigators assessed changes in total cholesterol and LDL-C concentrations, as well as in creatinine clearance. Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Changes in Total Cholesterol: Statin ± Ezetimibe in Kidney Transplant Patients 20 10 mg/dL Control 0 Ezetimibe treated -10 p=0.001 -20 -30 0 3 6 9 Months Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. 12 Changes in LDL-C: Statin ± Ezetimibe in Kidney Transplant Patients 0 -10 mg/dL Control Ezetimibe treated -20 -30 p=0.002 -40 0 3 6 9 Months Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. 12 Changes in Creatinine Clearance: Statin ± Ezetimibe in Kidney Transplant Patients 7 6 5 4 3 2 1 0 -1 -2 -3 -4 -5 -6 -12 (MDRD equation) Control Ezetimibe treated p=0.025 -9 -6 -3 0 3 6 9 12 mg/dL/1.73m2 mg/dL (Cockcroft-Gault formula) 7 6 5 4 3 2 1 0 -1 -2 -3 -4 -5 -6 -12 Months Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Control Ezetimibe treated p=0.033 -9 -6 -3 0 Months 3 6 9 12 Multivariate Analysis for Change in Creatinine Clearance Dependent Variable: Delta Creatinine Clearance Cockcroft-Gault MDRD Treatment group 0.0187 0.0195 Tacrolimus 0.1261 0.0958 Cyclosporine 0.6763 0.2722 Acute rejection 0.0773 0.2147 Donor age 0.5287 0.2071 HLA mismatches 0.0874 0.0922 Months after transplantation 0.6818 0.8832 Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Other Observations with Ezetimibe in Kidney Transplant Patients • The investigators reported that: – Ezetimibe therapy was “nearly without side effects” in this population – Ezetimibe’s positive effects on endothelial function may be an explanation for the drug’s positive effects on renal function • Previous studies have indicated a direct positive effect of ezetimibe on endothelial function Adapted from Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Ezetimibe in Hypercholesterolemic Kidney Transplant Patients: Conclusions • Ezetimibe treatment in renal transplant patients was effective in lowering LDL-C and total cholesterol and is nearly without side effects • There was also a better preservation of renal function after 12 months of additional treatment with ezetimibe compared with the control group continuing high-dose statin therapy – Previous reports show benefits of statin therapy in renal transplant patients but not always a better preservation of renal function – The cholesterol-lowering effect of ezetimibe is one possible explanation for its positive effect on renal function – Benefit of ezetimibe on endothelial function may also play a role • Further studies with renal function as primary endpoint are required to investigate the influence of ezetimibe on kidney transplants Türk TR, et al: Nephrol Dial Transplant 2008; 23(1):369-73. Study of Heart and Renal Protection (SHARP) Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. Background: Rationale for the SHARP Study • Patients with established CKD are at high risk of CV events; the benefits of cholesterol-lowering therapy might be expected to be substantial in this population – There is evidence, however, that the benefits in the general population may not translate to patients with CKD – Safety is not well established in CKD • Patients with CKD have generally been excluded from previous lipid-lowering trials • There is an important need for reliable direct evidence for cholesterol-lowering therapy in CKD Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. What Do We Know About the Impact of LDL-lowering in CKD? • LDL may not play as large a role in mediating CV risk in CKD as it does in the general population – Investigators have reported a negative association between blood total cholesterol and mortality in CKD – Only ~1/4 of cardiac mortality in CKD is directly attributable to MI (dependent on LDL); the other causes (cardiac arrest, arrhythmia, heart failure) are less dependent on LDL – The long-term safety of LDL lowering in CKD remains unclear Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. Association Between Cholesterol and CV Mortality General population 100 Diabetic 10 Non-diabetic Total mortality, % per annum CV mortality, % per annum 100 Hemodialysis patients 10 1 1 Total cholesterol, mmol/L Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. Total cholesterol, mmol/L Causes of CV Mortality in CKD ~25%: Directly attributable to MI (potentially avoidable with cholesterol reduction) ~75%: Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. Other causes (cardiac arrest, arrhythmia, heart failure) Not as dependent on cholesterol reduction Pilot Study of Lipid Lowering in Patients with CKD: UK-HARP I • Objective: To test the efficacy and safety of simvastatin and aspirin in CKD • Subjects: 448 patients with CKD (242 predialysis, 73 on dialysis, 133 with functioning transplant) • Interventions: Patients randomized in a 2x2 factorial design to simvastatin vs. placebo and aspirin vs. placebo for 1 year • Simvastatin results: – Simvastatin 20 mg reduced LDL-C by 26% vs. placebo – Simvastatin was not associated with excess risk of elevated liver transaminases or serious myopathy vs. placebo Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10 and Baigent C, et al: Am J Kidney Dis 2005 45(3):473-84. Pilot Study of Lipid Lowering in Patients with CKD: UK-HARP II • Objective: To compare the efficacy and safety of simvastatin and simvastatin + ezetimibe in CKD • Subjects: 203 patients with CKD (152 predialysis, 33 on peritoneal dialysis, 18 on hemodialysis) • Interventions: Patients randomized to simvastatin 20 mg + ezetimibe 10 mg or simvastatin 20 mg + placebo for 6 months • Results: – Simvastatin + ezetimibe decreased LDL-C by an additional 21% vs. simvastatin alone – There were no serious adverse events caused by study treatments Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. and Landray M, et al: Am J Kidney Dis 2006; 47(3):385-95. The Study of Heart and Renal Protection (SHARP) • Objectives: To assess the effects of lowering cholesterol on major vascular events and on the rate of progression to ESRD among patients with CKD • Subjects: ~9,000 patients with CKD (6,000 predialysis, 3,000 on dialysis) • Interventions: Simvastatin / ezetimibe combination vs. placebo • Assessments: – Effect of LDL lowering on time to first vascular event (primary) – Effect of treatment on progression to ESRD – Effect of treatment on various mortality and morbidity endpoint Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. Rationale for the Treatment Agents in SHARP • Patients with CKD generally have average (or below-average) LDL-C levels – They may require a regimen that can produce a substantial proportional reduction to produce a worthwhile reduction in events – Use of higher doses of statins may increase the risk of muscle toxicity – Ezetimibe is a well-tolerated agent that has demonstrated additional LDL-lowering efficacy when added to statin therapy – The regimen chosen for SHARP was, therefore, simvastatin + ezetimibe Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10. SHARP: Conclusions • There is currently a lack of evidence supporting an association between dyslipidemia and increased CVD in patients with CKD • It remains unclear what proportion of cardiac disease in CKD is atherosclerotic and, hence, potentially modifiable with cholesterol-lowering therapy • In the coming years, SHARP and other studies in patients with renal disease should help to answer these outstanding questions Adapted from Baigent C, et al: Kidney Int Suppl 2003; (84):S207-10.