reputation
advertisement

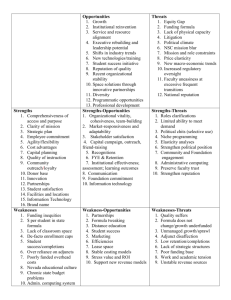
REPUTATION MATTERS! Building, Sustaining and Crisis-Proofing Reputation and Market Share Lewton,Seekins&Trester (Kathy, Steve & Ken) 14th National Forum on Customer-Based Marketing Strategies February 4, 2009 Las Vegas Reputation is real – so are crises! Both matter & can be managed Today we’re going to look at: • How reputations are built, nurtured and managed • How a crisis can impact reputation • And how a strong reputation helps an organization survive a crisis First, a sampler of crises past and present. . . Mt. Sinai New York 2002 “On top of the fiscal mess came the death of a man who had donated part of his liver in January 2002 . . . . .a state investigation found “woefully inadequate care . . . . Violations in 80 of 195 complaints patients had brought . . . . .The sum of it all has been a crisis of spirit.” “Today, most worrisome are the occupancy numbers.” New York Times Tenet 2003 “Amid widespread media coverage, Tenet said patient volume had declined 20 to 30% since the start of the investigation.” Modern Healthcare Duke 2003 “A Death at Duke “In the future, we can expect more publicity after major errors in medical care, especially when communication breaks down and trust is lost.” New England Journal of Medicine 3/20/03 “Ms Santillan’s plight also tarnished to some degree the reputation of one of the nation’s most renowned hospitals.” NY Times 2/22/03 And in just past six months . . . $13.5 awarded in hospital death; Jury faults doctors at Dana-Farber (Boston Globe) • “Dana-Farber did not issue an apology” Immigrants Facing Deportation by U.S. Hospitals (New York Times) • “Sister Margaret McBride, vice president for mission services at St. Joseph’s in Phoenix, which is part of Catholic Healthcare West, said families were rarely happy about the hospital’s decision to repatriate their relatives. But, she added, “We don’t require consent from the family.” And . . . . . . Top Psychiatrist Didn’t Report Drug Makers’ Pay (New York Times) • “Repeatedly assured by Dr. Nemeroff that he had not exceeded the limit, Emory did nothing.” And (truly) that just skims the surface Reputation matters “If you lose money for the firm, I will be very understanding. If you lose reputation for the firm, I will be ruthless.” Warren Buffett to Salomon Brothers employees Warren Buffet To Salomon Brothers employees Reputation has broad impact Affects employee recruitment, retention, performance and morale Ditto physicians, faculty Drives donations, grants, alumni support Attracts partnerships and alliances Supports or undercuts promotional efforts to build market share (Good service/bad hospital vs halo) Plays a role in decisions by managed care companies, foundations and more . . . . . Reputation can be managed Every organization HAS a reputation, even if no one knows what it is or tries to manage it Reputations can be created and nurtured, repaired and restored, managed and monitored And reputations can be damaged by poorly managed crises The Reputation Equation Reputation = Perception Perception = Reality + Awareness Reality = E2 Personal Experience + Trusted Endorsements In healthcare, E2 rules because reality reigns Promotion aside, the truth is that reality (as interpreted by personal experience and trusted sources) dictates patients’ choice in healthcare Latest Center for Studying Health System Change survey of 13,500 adults: • Choosing PCP: 50% F&F word of mouth, 38% MD recs • Choosing specialist: 69% PCP rec, 20% F&F, 18% another MD • Choosing hospital for procedure: 74% specialist rec, 14% another MD, 10% F&F Promotion can build awareness and amplify the reputation, but it can’t override nor create reality The HCO reputation management track record: C HCOs have the prerequisites for positive reputation given their lifesaving work Always assumed favorable reputations as a “given” Many did not actively work to sustain reputation based on performance Many focused more on promotion HCOs prone to crises • And many high profile crises have been handled badly Tarnish has affected the entire category Flash forward to 2009: All health care, all the time – and clearly Obama intends to keep it front & center Every sector is seen as a villain or potential villain (MDs, Rx, HMOs and yes, HCOs) • And we all provide enough fodder to make the concerns realistic The transition from white hat to black hat continues (nurses are tarnish exempt) And the public doesn’t know who or what to trust This is significant because without trust . . . The bond that is essential for human service organizations broken The impact can be massive • • • • From clinical outcomes To philanthropic support To over and re-regulation To patients not trusting caregivers So the time for reputation management and crisis protection is now! A good reputation is like money in the bank A solid reality-based reputation means the HCO has full account in the goodwill bank So when crises occur, as they will and do, the HCO’s reputation destroyed • But if the goodwill bank is empty, damage can be lethal Managing the crisis effectively will keep that reputation and the bank account intact • Alternatively, if the crisis is not managed effectively, even a big bank account can be overdrawn A closer look at building and protecting reputation Part One: Building a Reality-Based Reputation Building & Burnishing Reputation:The Basics 1. 2. 3. 4. 5. An integrated process Audience identification Audience research Message development Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve Building & Burnishing Reputation:The Basics 1. An integrated process 2. 3. 4. 5. Audience identification Audience research Message development Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve 1. A complex universe with many players Donors, grantors Prospective employees, faculty Patients Families/ Visitors Government Consumers Employees Management Reputation Customer Focus Faculty Students Volunteers Community Media And precisely because there are many players . . . . . Managing reputation requires an integrated approach involving multiple functions: • • • • • • • PR Marketing Alumni Development Employee relations Physician relations And . . . . . Integration does not mean a single control point It does require a collaborative, inclusive team approach • Get the right people at the table – someone has to make the first move • Focus on institutional objectives • Agree on master audience list • Use research data to: – Identify current communications channels – Identify appropriate messages – Shape strategies and tactics AND then . . . . . Develop a comprehensive plan With core messages And messages tailored by audience Clearly identified tactics, many that will reach multiple audiences Implementation responsibilities based on expertise, experience and interest And make this planning process part of the regular strategic plan process for the entire institution so that “they” buy-in And execute (the plan, not each other) Goal is to ensure no audience is overlooked or ignored And that there’s no duplication of effort Build in monitoring and benchmarking Keep the team together to track, make midcourse corrections, evaluate, revise plan Building & Burnishing Reputation:The Basics 1. An integrated process 2. Audience identification 3. Audience research 4. Message development 5. Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve 2. Audiences: Who ARE those guys? Before we can decide which audiences matter the MOST when it comes to building, enhancing a reputation, we first need the complete list HCOs have a tendency to overlook some key audiences (or not even realize they exist) Those audiences that are on the radar screen are often viewed too broadly, as large, homogenous groups (“physicians”), when in reality they are comprised of many subsegments Start with: Employees • Current, retirees, past, families Physicians • Faculty, voluntary attendings, referrers, potential referrers Patients • Current, former, families Governance Payors Medical students, residents, fellows Med school alums Donors, grantors Non-MD referral sources Media Community • Civic, business leaders; neighbors, organizations And don’t forget: Volunteers Vendors UNIVERSITY • Faculty, staff, students/families, alumni PETA et al KOLs nationally Associations “Consumers” • Many may be part of another audience already and thus are getting your messages • Important to consider differences between segments (age, ethnicity, income/ education, diagnosis, attitudes, healthstyles, gender) and when/how to segment even further (not all “women” share same concerns, issues, needs) While all audiences matter . . . . Some are either lethal weapons or can be your advanced life support when it comes to reputation, especially in crises, because they speak from personal experience • • • • • • • • Employees Patients Physicians Employees Patients Employees Physicians Employees . . . . . . Key audiences must not only know you . . . . . But also must love you (or at least like or respect you) That means building relationships And that process begins with understanding the audience And that means research Building & Burnishing Reputation:The Basics 1. An integrated process 2. Audience identification 3. Audience research 4. Message development 5. Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve 3. Reputation planning research helps us discover: Who are our stakeholders (audiences) that can impact or be impacted by our reputation? What do they know and feel about us now? What do we need to tell them to build awareness, credibility, support (message)? How do we reach and motivate them (strategies and tactics) Audience research is the core of reputation management You can’t start creating messages without knowing what stakeholders • • • • • • Know Believe Feel Want/ don’t want Need Value Once you have this data, you can do the classic gap analysis Identify gaps between current and desired reputation And set out to fill those gaps Research has special role in HCO setting . . . . . Because the decision-makers are data driven (H1) Because it provides a benchmark against which to measure Because it provides a road map for each stakeholder group • What messages work, don’t work And the core research program should also include: Employee attitude/opinion studies Ditto for physicians/faculty Routine consumer awareness/preference benchmarks as well as major studies Referring physician/provider surveys Community/opinion leader perception audits Multi-faceted patient satisfaction program And all of this data helps us develop MESSAGES!!! Building & Burnishing Reputation:The Basics 1. An integrated process 2. Audience identification 3. Audience research 4. Message development 5. Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve 4. Oh, yeah, the MESSAGE (we’ll get to that after we decide on ads vs. Twitter vs. stadium signage) The reason many communications campaigns fail is simply because the message doesn’t work, for one of four basic reasons: • • • • They don’t understand it (Comprehension) They don’t believe it (Credibility) They don’t care about it (Relevance) It doesn’t touch their emotions (Resonance) C2, R2 Comprehension – do they get it? HCOs are huge abusers of jargon • Acronyms, science terms, insider info (Magnet) And we pile on the FACTS, FACTS, FACTS And we often rely on print channels when the “average” consumer audience includes: • • • • Illiterates Semi-literate Anti-literate Poor vision, hearing Credibility – do they believe it? Overpromising, directly or indirectly Overendorsing Overqualifying Overhyping things that have no inherent credibility to the average consumer • Ratings, rankings • Awards • Credentials that are unintelligble to the consumer (FANA, FACHE, CRRRRRRT, etc.) Relevance – does it matter to THEM? Do they care about: • Service or product or procedure they figure they’ll never ever need or use • Who manufacturers anesthesia equipment • Lots of high tech terms • Hospital that’s two hours away • We, us, our . . . . . . . all about YOUR assets rather than their real-life needs and how they will benefit Resonance – does it touch their feelings? For a message to move audience to action, it has to touch heads and hearts • Real people with real stories • Showing rather than telling • Don’t be afraid of what we think of as the same old types of words and visual images IF they resonate with your audience Only one way to ensure messages will work Test, test, test • In your market(s) • With your target audienceS • With a talented moderator/interviewer who can play word games An even closer look at reputation: performance & relationships Building & Burnishing Reputation:The Basics 1. 2. 3. 4. An integrated process Audience identification Audience research Message development 5. Key strategy: Building reputation via performance and relationships • • • • With all of our customers, especially patients With our employees With our physicians With the communities we serve We must focus on performance Reputation is built on reality (remember the equation) And reality means how we perform, how we do our work, how we take care of and build relationships with our core stakeholders: patients, employees, physicians and community Promotion is an important part of burnishing reputation because it builds awareness – but the foundation is performance So marketing/PR must be integrally involved in organizational performance, not just relegated to promotion or communications 5. Key strategy: Building reputation via performance and relationships With all of our customers, but especially patients With our employees With our physicians With the communities we serve Patient satisfaction (still a work in progress according to HCAPS) Patients are “expert endorsers,” and their opinions are based on their experiences Thus, their satisfaction is essential in terms of shaping reputation Management of function requires group effort • PR/marketing should support/staff the function to ensure that data is translated into action Requires coordination with all operating units – rarely does a problem have a single owner Patient satisfaction is a mission, not a program A question of culture It starts with the “quest for excellence” Quality care and optimal outcomes require satisfying patients. • There are strong correlations between patient satisfaction and clinical performance, and patient satisfaction and outcomes The marketing/public relations role begins at the top Marketing/PR officer often needs to help make the case for culture change First, the CEO; then tackle the rest of the gang: • Bring data – – – – – Ongoing phone surveys (core benchmarking tactic) Quick response feedback system Focus groups Expectation/gap analysis Print survey, primarily for good will • Bring strategy, models and tools If you have a crisis, leverage it If you don’t have a crisis • Lead by inspiration • Model the competition The marketing/public relations role also includes: Culture management Keep the platform burning Provide measurement tools • Manage the survey • Shoppers • Other feedback mechanisms (Web, callbacks) Spread the message • Successes AND failures/challenges • Metrics outcomes and benchmarks Keep it on top management’s agenda Make it stick - even if you’re big, complex & decentralized Clear vision, definitions and standards New processes to support new cultures • HR policies and practices critical • Reliable tracking systems • Accountability mechanisms Disciplined, methodical rollout plan with standardized communications The Ritz-Carlton Formula Make management visible Imprint the standards Lineups: everyday, everyone (more on that) Put employee satisfaction first 5. Key strategy: Building reputation via performance and relationships With all of our customers, especially patients With our employees With our physicians With the communities we serve Employee relations Foundation of reputation program • Employees can support or undercut all messages to other stakeholders • Employee behavior drives patient satisfaction, market share (and quality, cost containmnet, etc.) • Too important to be left to HR • Can be managed collaboratively with HR Employee communications Requires multiple channels • Education/literacy variations • Employee preferences • Repetition important Face to face with supervisor remains #1 preferred channel • Publications, e-mail, videos, etc., can be used to reinforce, explain details The Huddle: A breakthrough communications tool Systematic process for assuring group discussions every day Case in point: Oakwood Healthcare, Detroit MI Guiding principles Simplicity: 5 to 10 minute meeting Consistency: everyone, everyday, every shift Interactivity: discuss Service First! Standards Motivational: reinforce personal values Fun: engender team spirit Do you rely on huddles for information? Patient loyalty scores: cause and effect? Other major gains Pre Post Change Consumer Top-of-mind Awareness 36.3% 44.2% 7.9 Consumer Preference 31.2% 41.6% 10.4 Market Share 35.3% 38.9% 3.6 -2% 1% 3pts Profitability Chain of success starts with satisfied employees The VanRinsven formula for victory Hire right Do “onboarding” by top leadership in person Create “emotional engagement” Show employees AND physicians that an environment of engagement is in THEIR best interest 5. Key strategy: Building reputation via performance and relationships With all of our customers, especially patients With our employees With our physicians With the communities we serve Physician relations matter Physician opinion vital in maintaining reputation AND REMEMBER THE STUDY: They DELIVER the patients HCOs often take a pieces/parts approach to HD relationships: very fragmented in terms of responsibility for managing • Many people can be involved, but someone has to own responsibility for the process Physician relationships Must be based on MDs #1 concern: RESPECT Must be driven from the top down Walking the talk is critical Most MDs, when asked carefully, will admit don’t want ultimate, total control – but they absolutely DO want input, to be listened to Physician communications 10.0 Brutally brief Actionable RELEVANT In the format THEY choose • Maybe combination of email, blast FAX and yes, even snail mail • We NEED them to get the info Peer to peer is critical for credibility And they still want the respect of face to face time with admins And the old standby – repetition – is absolutely critical with this audience 5. Key strategy: Building reputation via performance and relationships With all of our customers, especially patients With our employees With our physicians With the communities we serve • An area long ignored by most HCOs because it seems “old-fashioned” • It isn’t Twitter but it is critically important in times of shrinking resources • So we want to spend extra time here It’s back to our roots “Hospitals exist with the tacit permission of the communities they serve” And the only force that ever stopped the WalMart juggernaut was organized community opposition So it’s time for total immersion in the community, building trust by being there, being credible and demonstrating caring Back to the very basics Relationships put a face on the organization, we personalize it • It’s harder to dislike organizations where you know the people • And in crises, people who know you tend to believe you CR should be seen as a primary PR function – NOT as an add on to someone else’s job Not budget intensive when compared to other functions, but it does take staffing • Takes commitment from senior management – personal time commitment CR 101 begins with the basics Advisory Boards are foundational strategy • IF you use them effectively – – – – – – Have a role and goal Cast a broad net Create a solid structure Listen – and then respond Make them “insiders” Use them as loyal advocates And the old stand-bys still work! The All NEW Speakers Bureau • Give it a jazzy name, a logo, a brochure, a champion and you’ve got SB for a new decade • HCOs have what consumers want: nice smart people who know a lot about health care and community organizations podium, audiences – Seek out platforms that match marketing strategy – Prep and train speakers, send out with HCO’s core messages – Evaluate and monitor – Seize the day – breaking news And the old stand-bys still work! Bring ‘em in – HCOs fascinate the public And there are other ways to get the consumers into you facility Offer free meeting space – and tack on a mini-tour to one of your hot service lines For target audiences, supplement the (well trained and monitored) tour guide with a physician in a hot specialty Outsiders IN: The Influentials Program Invite the right people -- create a powerful database • Yes, the usual suspects (mayor, council, C of C, biz CEOs) BUT go further • Look at ALL segments of your community (education, arts, social services, labor unions, minority groups, etc.) and do the research to find the leaders • Who are people who can influence several hundred other people? – Clergy, activists, Junior League president, etc. Insider influencers Treat influentials like the special people they are: private, first-class dinner hosted by CEO, chairman of the Board Exciting presentation by compelling physician on a hot or timely topic After the party’s over . . . . . the work has just begun • Frequent personal updates from CEO (letters, one-onones, etc.) • “Insider” status – they hear the news FIRST • Find ways to involve them based on their needs • Mini-internships or “go alongs” can be very effective Insiders Out: The Ambassadors Program Community liaisons can be the best communications channel ever! • Takes time and careful management, but pays huge dividends The true value of this program becomes evident when you have a crisis and need to get truth to the community OR when you have an issue and need to build grassroots support Outside ambassadors Find the people in your HCO who know the people out in the community • Begin with audit of who’s involved in what – and don’t just ask management Invite participation, outline role clearly, provide incentives • Most important incentive is feeling of “contribution” • “Ambassador” title and a plaque also help! Outside ambassadors Liaisons’ primary role: LISTEN • Early warning system for emerging issues or anti-HCO sentiment • Need easy mechanism for getting info and feedback to PR • Personalized facet of environmental scanning, to add real life reality to the data When needed, liaisons can also deliver messages – but must be done without compromising their status in the group Inside and Outside: Partnerships Sponsorships -- $$ in return for a logo (one among many) on a 5K Walk T-shirt • ROI negligible Partnerships – long-term side-by-side commitment that builds trust and relationships • You’re OUT THERE, being visible and credible • Your people work side by side with other community leaders • The ultimate win/win The Partnership Paradigm: It takes hard work “Mission” goes real-time Begin with the community’s need (not the HCO’s agenda) You may need to lead the community needs assessment (which is a great position) ID problems which can be solved at local level Focus on healthy communities Partnership principles Pick the problems that you are most suited to address • The HCO can provide brains, or brawn or bucks – or all three Find one or more appropriate partners (generally local, but other sources can support with funding – i.e., RX companies) • Media outlets can be great partners – just be equitable Manage the partnership like a business – measurable objectives, biz plan, monitoring and evaluation And make sure the Board is involved, too Board members are from and of the community – built-in credibility • Board CR Committee should take the lead – Opinion leader visits, briefing lunches/breakfasts • All Board members should have briefing cards and info updated regularly And finally – don’t neglect health education/prevention programs • Whether inside out, or outside in, they impact reputation and market share PART TWO: Managing a Crisis to Protect Reputation Media relations: Last step in building reputation, first step in protecting it Once the foundation programs are in place, and relationships strengthened, a proactive media program is a valuable tool The upside of media coverage: – Credibility, reach (broad and narrow), cost effectiveness The downsides: • Lack of control (timing, full story, accuracy) • Contradictory messages may be included • Frequency – only one hit per outlet – although multiple hits create bandwagon effect Today’s media environment: Is incredibly intense 24/7 means there is no “down time” Incredibly competitive Sensational sells (“If it bleeds, it leads”) Reporters are cranky, harried, tired, underpaid, feel unloved • Pushed around by editors and news directors Media Relations 1 and 2.0 Commitment to honesty, candor, access • Commitment from senior management is essential first step Designated media relations function • Protocols and policies • Full-time manager and staff • TRAINED spokespeople Media Relations 1 and 2.0 Healthcare is STILL a hot topic – we’ve got the human interest, the drama, the politics, the costs • Great fodder for coverage – good and not so Reporters, editors, producers NEED sources and resources Desksides, e-mail access help lay groundwork, build relationship Stay in touch without expecting coverage Controlled vehicles (SMTs, RMTs, VNRs, ANRs, etc.) can help deliver the story to national audience Social media – despite the hype, the jury is STILL out • Powerful channels, yes; for HC messages . . . . .? Two kinds of interviews: risky and risky A crisis or negative story has built-in risks But even “normal” interviews can get out of control “It’s always a risk to speak to the press; they are likely to report what you say” Hubert Humphrey To stay in control: Preparation is ESSENTIAL • What do you want readers/listeners to know, think, feel • What are your messages and proof points • Get it down on paper • Avoid JARGON • Simplify, simplify, simplify To get your message across: Think in headlines • Do NOT begin at the beginning --- use pyramid approach. • Then comes key fact, supporting facts and proof points. Anticipate what questions reporter will ask – positive and negative. “If you dread it, you’ll get it” During the interview: If you don’t know the answer, say so and promise to get the information. Don’t get provoked, don’t fake answers and DON’T LIE or say “No comment.” • Explain why you can’t answer – patient privacy,legal restrictions, etc. Don’t overanswer – answer and then stop talking. ALWAYS put the patient and family first. Express sorrow and compassion. A crisis only exacerbates risk A crisis in a healthcare organization is NOT an external disaster that the HCO must respond to • That’s by-the-book and you can plan and drill for it – and it’s not “your” crisis A crisis is something that happens within the hospital that can damage reputation • And it’s something that happens unexpectedly, vs. a long-simmering issue that can be managed Such as: Any nominees? CPR = Advanced media relations It’s not “if” a crisis happens – it’s when and how soon and how BAD is it • Medical errors are inevitable • Patients/families now understand why and how to take their stories public • HCOs still seem to be caught off guard, to respond with arrogance and reinforce preexisting negative stereotypes And CPR is needed because: It’s life or death • Media coverage is instant • Web coverage is instant-er The outcomes are critical • Litigation • Damage to reputation • Loss of confidence among patients, physicians and EMPLOYEES • Loss of productivity • Undercut all your marketing efforts When the crisis comes, it is a CRISIS Crisis PR may be only 2% of a PR job, but it can often be make or break • Reputation can be irrevocably damaged – not by the medical or institutional mistake, but by how the institution reacts and responds • The public WILL forgive mistakes – but NOT dishonest, disingenousness, arrogance Some make CPR sound simple But it’s not • No cookie cutter approach that works in every case • A plan is only a piece of paper without institutional buy-in • Situations can be anticipated, but real life can be different • It‘s about people – unpredictable people – and in health care, it’s about life/death It begins with a mindset Strategic communications process in place Full buy-in of senior management CPRO part of senior management team Detailed operational plan Pre-existing conditions: strong credibility and good relationships with media And also requires: Effective internal and stakeholder communications channels already in place and fully road tested Spokespersons already trained and tested • One MUST be an MD, ideally not the CEO And a full account in the goodwill bank Jack Welch and Fraser Seitel on crisis management – the wrong way 1. 2. 3. 4. 5. 6. 7. Ignore the problem as it festers, or deny it once it happens Containment – give it to someone else to solve Tell half truths or LIE Let bad news dribble out Assign blame MEA CULPA x 10 Paralysis Johns Hopkins 2001 “Hopkins officials reacted with outrage to the suspension of research, calling the action unwarranted, unnecessary, paralyzing and preciptious.”* NYTimes *Three days after accepting “full responsibility” for the death of a young woman in a clinical trial What organizations want from PR: The 4 C’s Companies in Crisis want Calm Counsel from their in-house team and consultants • Our collective wisdom abased on accumulated experience • Our third party objective viewpoint – unemotional, providing clear guidance based on expertise • Arms, legs and warp speed communications counsel and tactics that can turn things around Companies in Crisis want Calm Counsel So we must provide that counsel • Sometimes they may act on it sometimes they may ignore it • Even if our advice is not heeded, we still have go do our ultimate best to help the organization survive and ideally, move on to propser • But above all else, what’s needed is calm . . . Or the illusion of calm What’s expected Team that is THERE 24/7, on site, with no whimpers • Energy, realism, optimism • A team that sees the BIG picture – All the audiences – The real issues and the IMPACT • A team that’s one step ahead What’s needed A team that will help management • Moderate their emotional responses, so anger, fear or bitterness don’t drive decisions • Face facts with straight talk, even if it’s not what senior management wants to hear • Keep all the balls in the air – remember the things they may forget • Put out the fire AND keep the plane in the air and headed to its destination Crises come in two varieties The true surprise – urgent, big blow up, trains JUST collided Smoldering – the homegrown train wreck • Been creeping up for months but was ignored or denied • Started as something manageable but wasn’t managed, so it just grows and grows like the bread dough in Lucy’s oven And there are two responses to managing crisis comms: Utopia: there’s a plan, and the crisis fits the plan Reality: the crisis is a unique little firestorm ..... BUT the institution is prepared with all the tools in place AND has rehearsed via scenario drills The Basics: The Team Established in advance – crisis is no time for saying “Should we call XXX” or answering “But what about ME?” • • • • • • • • • CEO HR Legal Operations Risk management IT possibly Security PR Others PRN Establish chain of command and tie-breaker The Basics: The Plan Must be in sync with HCO values, mission Detailed P&P to insure that potential crises are reported! • And make sure employees are oriented and trained Detailed info on who does what when • For example, when senior manager hears about a crisis situation – who gets called FIRST? CEO? PR? Lawyer? Figure it out now. Implementation instructions Resource and contact info – updated weekly The Basics: The Essential Info Master list of all key audiences • Contact database Allies database Systems – phones, pagers, Blackberries • With fall-back plans when systems crash Media logistics Fact sheets already printed “Dark” section on website, ready to go The Basics: Pre-Screened Spokespersons SpokespersonS must be: • • • • • • Credible Mediagenic Coachable, trainable Constantly available Calm, calm, calm – unemotional, ego-free Stamina Weigh the merits of CEO, COO, MD, PR TRAIN, train, train, and train The Basics: Anticipate and Rehearse Issues anticipation • The predictable and generic • The “that could be US” opportunities Routinely (at least quarterly) put the team through a crisis drill with a scenario “torn from the headlines” Scenario drills deliver “Working” these issues provides ideal time to: • Kill the “no comment” mentality • Try out spokespersons and decision-makers – role play • Confront the “WE DON’T MAKE MISTAKES LIKE THAT” mentality • Thrash things out with legal in advance Scenario drills deliver Allow for: • • • • Assessing probability Identifying potential audiences by scenario Assessing severity and risks Determining – in advance – what the answer to the first question Scenario drills also: Allow you to show CEO et al examples of good CPR and bad • Start with the classics -- Nixon, Exxon vs. Iacoccoa, Tylenol • Then use current/recent hospitals Allow you to road test your team, your plan, spot any inbred issues and deal with them And provide time to teach your team the RULES CPR: The cardinal rules Never, ever, ever lie – the truth will ALWAYS COME OUT • The “You Tube” generation • Any employee can dial NY Times And never speculate • Educated guesses that turn out to be wrong – look like lies to the public • “I don’t know” can’t come back to bite you like a lie or speculation can Respond quickly and calmly CPR: The crisis is NOW When the crisis happens, the first pulse to take is your own Bring in outside counsel • Internal staff simply cannot be objective and immune to emotion • Outside counsel can confront CEO, MDs, angry Board chairman, et al CPR: The crisis is NOW ID and prioritize the affected audiences • Employees and closest in audiences are always first, usually forgotten – Employees in an info vacuum = rumors – Employees receiving bad or misleading info = critics – Employees receiving frequent updates and info = community info representatives • Validate your statements to media • ID and counter rumors • Able to be productive and do their jobs • Then – who else is affected??? CPR: The crisis is NOW Get the facts – divide up the work if needed Assess the damage potential • Overreaction is dangerous – poll if needed • But in a 24/7 news environment, with patients/advocates who see the role coverage can play, assume it will go public sooner rather than later Frame the messages FIRST, before obsessing about channels • Do NOT write by committee! CPR: The crisis is NOW The message must: • Focus on the harmed party – NOT “we” • Be utterly candid – “I don’t know that now” is OK, no comment is not • Begin with statement of compassion – Know how to apologize or at least express regret • Accept blame if an error has been made – Assume there WILL be a lawsuit someday – Worry about court of public opinion NOW CPR: The crisis is NOW The message must also SHOW as well as say • Prove it! • What steps are you going to take? • What steps have already been taken? CPR: The crisis is NOW Get to your internal audiences BEFORE they see the coverage and stay in touch • • • • • Employees Board, governance Physicians KEY community opinion leaders Patients, past patients Stay below radar – e/vmail, CEO phone calls, employee meetings – but assume everything will go public USE your website!!!! The Crisis Interview GET THE FACTS ASAP Know the first question they will probably ask and have your answer ready Begin with expression of sympathy if appropriate Admit the error if there was one (you’re going to settle anyway) Remember who’s listening • • • • Patient, family Employees, physicians Referring physicians Community, potential patients CPR: The crisis is NOW Monitor media coverage – correct rumors or misinformation Monitor public opinion, formally and informally Know when to go back to “normal” mode Make sure management is still flying the plane! Case in point: The Duke situation Looking from the outside in – which is precisely the perspective of the institution’s key audiences CORE PROBLEM was how caregivers managed (not) relationship with patient’s family • “Conflict between caregivers and the patient’s supporters” -- Dr. Davis • The story “suddenly” became public – should not have been a surprise Duke Let situation fester and worsen Tried to use in-house staff to manage emotional, angry physicians Initial comments bad – “We do hundreds of these, we don’ t make mistakes, this is a tragedy for US” Spokespersons not charismatic WW syndrome • “Patient’s supporters” (they are a FAMILY) • “These things happen” Duke Did things by the book, but didn’t seem to comprehend how that plays to public • Refused second opinion on brain death Never seemed to get it together • After Jessica died, spokesperson said “he could not confirm” whether 2nd opinion was requested • Doctors and admins “not available for comment” • ’60 Minutes’ not bad – until the end, when surgeon said ‘these things happen’ – sounding cold, irresponsible Duke is not an isolated case HCOs (especially academic medical centers) generally tend to believe they are infallible • “This could not have happened” • “We do not make mistakes like this” • “We have procedures in place and followed them” The public thinks: It did. You did. So what? It’s now a brand new world The medical error issue will not go away, even without cases like Jessica “Inappropriate” deaths are inevitable and unavoidable, as are all kinds of other errors Media smell blood in the water HCOs that are deficient in good patient relationship skills increase the likelihood of family going public So the next Duke could be you Have the conversations, the scenario planning, the bitter fights over who will speak, what will be said – NOW AND strengthen and refine that performance-centered, reality-based reputation building program so that the goodwill bank will be as full as possible when the crisis hits! Bonus Points: Legislative Relations as an Extension of CR Legislative relations is a natural extension of CR Make it a priority • Needs to be a clearly designated role of member of management team (with responsibilities ranging from ongoing legislative interactions to internal briefings/training and legislative databases) • Translate the hospital’s legislative position on national issues for local press and editorial boards • Make a government relations report a standing agenda item at Board and management staff meetings Legislative relations . . . . Make it a priority • Involve trustees and management staff in setting the policy agenda • Take trustees and key managers on legislative visits to the state and national capitols • Regularly brief all members of the “family” — employees, physicians, volunteers, vendors/suppliers, patients. Don’t wait until they’re needed to write letters or make calls. Legislative relations . . . . Building real relationships with legislators and staff • Know the health care organization’s legislators — federal, state, and local • Identify “who knows whom” — which people in the HCO (not just management) have personal relationships with legislators and can serve as intermediaries and endorsers Legislative relations . . . . Building relationships • Set up ROUTINE meetings with the CEO and the health care organization’s legislators and city officials • Get to know the legislators’ staff members — field reps at their local offices and administrative assistants in the statehouse and federal offices Legislative relations . . . . Building relationships • Be helpful — offer legislators the chance to address the HCO’s employees, medical staff , board members, or other influential gatherings • Make sure your trade association keeps you posted on the key issues and positions of your state and federal representatives • Consider establishing key contact programs, modeled after those used by corporations Legislative relations . . . . Continue the relationship • Conduct briefings for legislators at the health care organization at least yearly — and – Make your schedule fit theirs. – Provide updates on changes and achievements, and share your position on pending or potential issues • Take the lead in getting HCO competitors to work together on key issues Legislative relations . . . . Instread of focusing your message on what the HCO needs – instead focus on how what you want will affect people – the voters “Pre-qualify” potential partners and advocates • Through issues management function, identify supporters • Build relationships before they’re needed – through CR 101