2013-gemc-res-lex-board_review_-_administration
advertisement

Project: Ghana Emergency Medicine Collaborative
Document Title: Administration: Ethics/ Medicolegal/ EMS/ etc.
Author(s): Joe Lex, MD (Temple University School of Medicine)
License: Unless otherwise noted, this material is made available under
the terms of the Creative Commons Attribution Share Alike-3.0 License:
http://creativecommons.org/licenses/by-sa/3.0/
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your
ability to use, share, and adapt it. These lectures have been modified in the process of making a publicly
shareable version. The citation key on the following slide provides information about how you may share
and adapt this material.
Copyright holders of content included in this material should contact open.michigan@umich.edu with
any questions, corrections, or clarification regarding the use of content.
For more information about how to cite these materials visit http://open.umich.edu/privacy-and-termsuse.
Any medical information in this material is intended to inform and educate and is not a tool for selfdiagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare
professional. Please speak to your physician if you have questions about your medical condition.
Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers.
1
Attribution Key
for more information see: http://open.umich.edu/wiki/AttributionPolicy
Use + Share + Adapt
{ Content the copyright holder, author, or law permits you to use, share and adapt. }
Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105)
Public Domain – Expired: Works that are no longer protected due to an expired copyright
term.
Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public
domain.
Creative Commons – Zero Waiver
Creative Commons – Attribution License
Creative Commons – Attribution Share Alike License
Creative Commons – Attribution Noncommercial License
Creative Commons – Attribution Noncommercial Share Alike License
GNU – Free Documentation License
Make Your Own Assessment
{ Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. }
Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b))
*laws in your jurisdiction may differ
{ Content Open.Michigan has used under a Fair Use determination. }
Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws
in your jurisdiction may differ
Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee
that your use of the content is Fair.
2
To use this content you should do your own independent analysis to determine whether or not your use will be
Administration: Ethics /
Medicolegal / EMS / etc.
Joe Lex, MD, FACEP, FAAEM, MAAEM
Associate Professor of Emergency Medicine
Temple University School of Medicine
Philadelphia, PA USA
3
4
5
Today’s Menu
•
•
•
•
•
•
•
Ethics
Medico-legal
EMS
Non-hospital settings
Disaster medicine
Wellness & impairment
Nuts & bolts
6
7
Ethics and The Law
• Societal values are incorporated
both within the law and within
ethical principles and decisions
• Good ethics makes good law
• Good law does not necessarily
make good ethics
• Significant overlap exists between
legal and ethical decision-making
8
Rights and Duties
• Active rights: right to act or not act
as one chooses
• Passive rights: right to not be acted
upon by others
• Duty: action required by rights of
others, law, higher authority, or
one’s conscience
9
Rights and Duties
• Without a duty to act, there can be
no rights
• Role / duty link occurs “whenever a
person occupies a distinctive place
or office in a social organization, to
which specific duties are attached
to provide for the welfare of
others...”
10
Values
• Standards by which human
behavior is judged
• Learned, usually at early age
– Observing behavior
– Secular, professional, religious
• In pluralistic society, clinicians
must be sensitive to alternative
beliefs and traditions
11
Professional Values
•
•
•
•
To save lives when possible
To relieve pain and suffering
To comfort patients and families
To protect staff and patients from
injury
12
Some Definitions
• Beneficence: duty to confer benefit
• Distributive justice: fairness in
allocation of resources, obligations.
• Personal integrity: adhering to
one’s own reasoned, defensible set
of values and moral standards
13
Beneficence vs Nonmaleficence
• Basic tenet: “First, do no harm”
• Derives from recognition that
physicians can harm as well as
help
• “given an existing problem, it may
be better not to do something, or
even to do nothing, than to risk
causing more harm than good.”
14
Malfeasance / Nonmaleficence
• Malfeasance: hostile, aggressive
action taken to injure the patient’s
interests
15
Autonomy
• Recognizes adult person’s right to
accept or reject recommendations
for medical care, even to the extent
of refusing all care, if that person
has appropriate decision-making
capacity
16
Autonomy
• Counterweight to long-practiced
paternalism
– Practitioner determined what was
“good” for patient, regardless of
whether patient agreed
• Coercion: threat or use of violence
to influence behavior or choice
17
Truth-Telling
• Absolute honesty: some people
feel that the patient has the right to
know the truth, no matter what the
circumstances
• Being honest does not mean being
brutal; truth is best tempered with a
modicum of compassion
18
Futility: Definition
• Intervention is effective in <1% of
identical cases, based on medical
literature (e.g. ED thoracotomy)
• Physiologic futility: known anatomic
or biochemical abnormalities will
not permit successful medical
interventions
19
Futility
• Proposed intervention will not
achieve patient's goals for medical
therapy in accordance with the
patient's values
• Futility concept should never be
used to deny care to dying patients
20
Using Newly Dead for Teaching
• It is unethical to prolong
resuscitative efforts to practice or
teach procedures or to complete
research protocols
21
Definition of Death
• Cardiopulmonary “death” not
necessarily inevitable, irreversible
• Brain death: irreversible failure of
clinical function of the whole brain
– Apnea
– Profound coma, unresponsiveness
– Absence of brainstem reflexes
22
Definition of Death
• In the ED, cardiopulmonary death
is the only death that can be
recognized
• Use of term brain dead is to be
avoided
23
Withholding Resuscitation
• In most EMS systems, verbal
requests to limit resuscitation are
not accepted, because of the
concern that out-of-hospital
providers cannot confirm that these
represent the patient’s current
wishes
24
Referral to Medical Examiner
•
•
•
•
•
•
Traumatic death
Death due to natural disaster
In police custody / jail inmates
Suspicion of homicide / suicide
Suspicion of poisoning
Sudden, unexplained death not
clearly related to prior disease
25
Newborns Left in ED
• Most states have laws allowing a
mother to leave a newborn infant at
a “safe-haven” in an attempt to
reduce the numbers of infanticides
and abandonments of children in
unsafe places
• Know laws in your state
• Every ED should have a policy
26
Translation Services
• Federal and state laws require use
of translators in health care setting
• Patient should be made aware of
availability of these services
• If not available: translation by
phone in same language
27
Duty to Third Parties
• Tarasoff: physician owes duty to a
foreseeable third party when aware
of reasonable risk to that individual
• Obligation to warn or protect others
against a variety of dangers:
communicable diseases, impaired
drivers
28
Viewing Resuscitation
• Nearly all survivors who witnessed
ED resuscitative efforts found it
helpful
– Grieving was facilitated
– Fewer episodes of flashbacks
– Lower levels of anxiety, grief,
depression, post-traumatic avoidance
behavior
29
30
Informed Consent
• Part of every patient / physician
interaction
• Legal standard under which
physicians educate patients (those
who have capacity to make
medical decisions or their legal
caretakers) about proposed
treatments and alternatives
31
Informed Consent
• General consent for treatment:
generally understood to cover
history taking, standard exams,
and basic procedures (blood
analysis, venipuncture)
• Does not provide consent for more
detailed, risky, invasive procedures
32
Informed Consent
• Allows patient to make decisions
consistent with personal values
• Based on belief that it fosters twin
concepts of patient well-being and
autonomy
33
Exceptions to Informed Consent
• Emergencies
• Therapeutic privilege
• Public health imperatives:
treatment of certain diseases
• Patient waiver of consent
• In ED: emergencies and public
health imperatives applicable
34
Capacity
• Definition varies among
jurisdictions
• In general, “individual’s ability to
make a decision based on
personal values and
comprehension of the likely
consequences of that decision”
35
Capacity Competence
• Competence often incorrectly used
interchangeably with capacity
• Legal term indicating a ruling by a
court that a person is unable to
manage his or her own affairs
36
Against Medical Advice
• Document capacity: with examples
• Discuss risks reviewed with patient
• Offer alternative treatments if
available
• Involve family, friends, or clergy in
decision
• Document treatment and follow-up
provided
37
Against Medical Advice
• Explain any potentially problematic
entries in the chart such as nursing
notes or abnormal laboratory
values
• For example, if the patient has an
elevated serum alcohol level,
document that the patient is
clinically sober and has capacity
38
Against Medical Advice
• Obtain patient’s signature: if
refuses to sign, document that fact
• State that an offer of care at any
time was provided to the patient
39
Treatment of Minors
• Generally considered to be anyone
<18 years of age
• Society and legal system have
adopted views that, in some
circumstances, older children may
make many medical decisions
independent of their parents
40
Treatment of Minors
• Emergencies
• Treatment of certain diseases and
conditions that are in the best
interest of the minor or society
• Minors emancipated under law
• Best interests of child are not being
addressed by parents
41
Treatment of Minors
• All states: STDs
• Nearly all states: alcohol or
substance abuse
• Many states: prenatal and
pregnancy-related care
• Sexual or physical abuse generally
permitted
42
HIPAA
• Health Insurance Portability and
Accountability Act
• PHI: Protected Health Information
• HIPAA allows covered entities to
use PHI without authorization for
purposes of treatment, payment,
and operations
43
HIPAA Do’s
1. Talk freely with patient’s primary
physician
2. Discuss PHI with consultants and
other members of the patient’s
health care team
3. Use PHI for reimbursement and
operational issues
44
HIPAA Do’s
4. Release records to the patient or
an authorized representative
5. Discuss patient PHI with family or
friends if the patient is in an
emergency situation, unable to
consent, and the information
would be beneficial to the patient
45
HIPAA Don’ts
1. Discuss patients or PHI in public
or unsecured areas
2. Leave computers with access to
PHI logged on and unattended
3. Discuss PHI in front of others
without permission
46
HIPAA Don’ts
4. Speak loudly when discussing
PHI, particularly in public areas
5. Look at records for which you
have no legitimate purpose as a
provider
47
Patient Transfer
• EMTALA: Emergency Medical
Treatment and Active Labor Act
• Applies to hospitals participating in
US federally financed Medicare
program
48
Patient Transfer
• All patients must receive medical
screening exam and be stabilized
before considering transfer to
another facility
• Receiving hospital must accept
transfer
49
EMTALA Obligations
• Provide a “medical screening
exam,” performed by “qualified
medical personnel,” to look for an
“emergency medical condition” for
all patients, who “come to the ED”
seeking care for medical condition
50
“medical screening exam”
• Process required to reach, with
reasonable clinical confidence, the
point at which it can be determined
whether an emergency medical
condition does or does not exist
• Must be same for every patient
presenting with similar symptoms
or complaints
51
“medical screening exam”
• Nurse triage does not meet
obligation to provide a medical
screening examination
• May not delay examination and
stabilizing treatment to inquire
about method of payment or
insurance status
52
“qualified medical personnel”
“The examination must be
conducted by an individual who is
determined qualified by hospital
bylaws or rules and regulations”
• Does not specify what type of
provider (registered nurse, medical
doctor, physician’s assistant, etc.)
should perform the medical
screening examination
53
“emergency medical condition”
• Acute symptoms of sufficient
severity, including severe pain,
such that absence of immediate
medical attention could place
individual’s health at risk
• Pregnant woman with contractions:
insufficient time to transfer patient
before delivery
54
“come to the ED”
• If on hospital property and makes a
request, or has a request made on
his / her behalf
• Prudent layperson would believe
that patient needs evaluation or
treatment
55
“come to the ED”
• Hospital property: “physical area
immediately adjacent to the
provider’s main buildings, other
areas and structures that are not
strictly contiguous to the main
buildings but are located within 250
yards of the main buildings.”
56
Stabilized
• “treatment as necessary to assure,
within reasonable medical
probability, that no material
deterioration of the condition is
likely to result from or occur during
the transfer of an individual from a
facility or that…the woman has
delivered the child and placenta”
57
Receiving Hospitals
Hospital with specialized capabilities or
facilities such as (but not limited to) burn
units, trauma units, or regional referral
centers may not refuse to accept a
transfer from a referring hospital
anywhere in the U.S. when the patient in
question requires the specialized
capabilities and the receiving hospital has
the capacity to treat the patient.
58
Receiving Hospitals
• Should the accepting hospital find
that the transfer was not
appropriate or improperly
motivated, it is both their duty and
remedy to report the transferring
hospital for a potential violation
• Failure to report an EMTALA
violation is itself a violation
59
Reportable
• Assault: gunshot and stab wounds,
sexual assault, physical assault
• Communicable diseases: venereal,
high contagious (hepatitis,
pertussis, influenza)
• Abuse
– Mandatory for child, elderly
– Domestic partner: varies by state
60
Reportable
• Deaths: already covered
• National Practitioner Data Bank:
– Disciplinary action following formal
peer review
– Any amount paid in judgment of
written malpractice claim
61
High Risk of Diagnostic Error
• Chest pain /
missed MI
• Wounds: FB,
nerve / tendon
• Fractures
• Abdominal pain
(includes AAA,
appendicitis)
• Pediatric fever
•
•
•
•
•
•
•
Meningitis
CNS bleed
Stroke
Embolism
Trauma
Spinal cord
Ectopic
pregnancy
62
Malpractice
• Four components:
–Duty
–Breach of duty
–Harm
–Proximate cause
63
Mitigate Risk
•
•
•
•
•
•
•
Communicate respectfully
Value your patient’s time
Thank the patient
Document thought process legibly
Manage patient expectations
No absolutes
Discharge with time / action
specific instructions
64
65
Manpower
• First responders: often first to
arrive at medical emergency,
• Typically police officer, firefighter,
first aid team
• Can perform CPR, immobilize
spine, control hemorrhage, other
basic interventions while awaiting
ambulance
66
Manpower
• Plan 1 ambulance response / day
for every 10,000 people in area
served
• 75% of EMTs are volunteers,
especially in rural areas
• When paid, salaries are 50% of
budget
67
Manpower
• EMT-B: trained to take care of
immediate life-threats
• Administer oxygen, perform CPR,
use an AED, control hemorrhage
• Extricate, immobilize, transport
emergency victims
68
Manpower
• EMT-I: training includes additional
patient assessment plus insert IV,
interpret basic ECG, administer
some cardiac medications
69
Manpower
• EMT-P: highest EMT skill level
• Greater training, broader scope of
practice
• Function under a designated
physician's medical license
70
Communications
• Use of 911 as nationwide
emergency telephone number in
US facilitated public access to
emergency medical care
• Emergency call takers: collect
information from caller, dispatch
appropriate medical resources,
offer first aid information
71
Communications
• Most EMTs operate under standing
orders and patient care protocols
developed by physicians
• Communications: weakest link
in most disaster responses
• EMS communication systems must
have built-in redundancy
72
Transportation
• Most important: ambulance design
allows providers to provide airway
and ventilatory support while
transporting patient safely
73
Transportation
• BLS ambulances: appropriate
equipment for EMT-B level
– Oxygen, bag-mask ventilation
devices, immobilization & splinting
devices, dressings for wound care
– Do not carry medication
– Cannot transport patients requiring
IVs or cardiac monitoring
– Some carry AEDs
74
Transportation
• ALS ambulances: equipped for
EMT-Ps or other advanced health
care personnel
– IV supplies, IV medication, intubation
devices, cardiac monitoring and
defibrillation
– Other specialized techniques unique
to specific areas: hypothermia
application after cardiac resuscitation
75
Transportation
• Ground transportation appropriate
for majority of patients, especially
in urban and suburban areas
• Helicopter should be considered
for critically ill patients when
ground transport time dangerously
long or if in difficult terrain
76
Public Safety Agencies
• EMS systems need strong ties with
police / fire departments
• Public safety agencies can provide
first responder services
– Often first on scene of emergency
• EMS provide medical support to
police and fire departments in
hazardous circumstances
77
Equipment: Defibrillators
• Early defibrillation: most important
factor in surviving cardiac arrest
• Paramedic-staffed ALS services
typically carry manual monitor /
defibrillators, often with additional
functions
– 12-lead ECG, external cardiac
pacing, synchronized cardioversion
78
Equipment: Defibrillators
• Increasing percentage of BLS
services carry AEDs
• Analyzes rhythm determines if
rhythm meets defibrillation criteria
informs operator that shock is
advised charges capacitor
defibrillates when operator pushes
appropriate button
79
Equipment: Defibrillators
• AEDs only shock ventricular
fibrillation and very fast ventricular
or supraventricular tachycardias
(>180 beats/min)
• Easy to use and effective:
promoted for first-responder public
safety personnel and for publicaccess defibrillation by laypersons
80
Equipment: Vascular Access
• Same as hospital: tourniquets,
cleaning agent, IV catheters, IV
fluid bags, and IV tubing
• Intraosseous access devices
increasingly popular if difficult
vascular access
81
Equipment: Spine Boards
• Preservation of integrity of spinal
column and cord of paramount
importance in prehospital setting
• Carrying boarded patients hard on
EMTs and paramedics
• Evaluating boarded patient more
expensive, time-consuming in ED
82
Equipment: Cervical Collars
• Two pieces, back and front
• One piece folded into shape
• Collars alone not adequate for
cervical immobilization
• Adequate immobilization: strapped
on back board and secured with
head blocks and head straps
83
Extremity Immobilization
• Field fractures splinted for patient
comfort, ease of transport
• Air splints adequate for most distal
fractures
• Sling and swathe
• Tie legs together with cravats
• Wrap pillow around extremity,
secure with tape
84
Helicopter Transport
• 867 helicopters in use in U.S. as of
early 2010
• Cost: $750,000 to >$5 million each
• Annual operating costs >$2 million
• Generally transport patients 1000
to 3500 feet above ground level
• Altitude-related problems tend to
be mild / non-existent
85
86
Mass Gatherings
• Considered to be events that have
at least 1000 people
• Same principles for athletic events
with <1000 people, cruise ships,
airplanes, wilderness environments
• Incidence of usage of medical
care: 4 to 440 patients per 10,000
87
Mass Gatherings
• Key to successful medical
response: reliable communication
among medical personnel, event
organizers, outside resources
• All events should have identified
physician medical director who is
responsible for developing medical
action plan
88
Ultra-Distance Athletic Events
• Common situation: management of
fluid and electrolyte repletion
• Massive sodium loss from sweat
• Overhydration with free water
• Risk factors for developing severe
hyponatremia (<125 mEq/L):
exercise time >4 hours, female
sex, low body mass index
89
Commercial Airline Flights
• Special mass gathering scenario
• Unique factors: lower O2 partial
pressure, potential exposure to dry
air, chemical irritants, virulent
airborne particles, venous stasis
• May aggravate normal health
behaviors through alcohol
ingestion, dehydration
90
Commercial Airline Flights
• Airline crew members educated in
basic first aid and CPR
• Most large commercial flights have
passengers with medical training
• Assuming care rendered is
voluntary, Good Samaritan laws
should provide protection from
medical malpractice liability
91
FAA Mandated Equipment
First Aid
Bandages
Antiseptic
Ammonia
Splints
Tape
Scissors
Equipment
Stethoscope
Gloves
Sphygmomanometer BVM
Oral airways
AED
Syringes
Needles
IV Tubing
92
FAA Mandated Equipment
Medications
NSAIDs
Epinephrine
Antihistamine Lidocaine
Atropine
Nitroglycerin
Aspirin
Normal Saline
Bronchodilator Oxygen
Dextrose
93
Cruise Ship Medicine
• ~10 million people travel on cruise
lines each year
• Average passenger age ~55 years
• Large vessels: >2000 passengers
and 1000 crew
• Most common complaints:
shortness of breath, minor injuries
94
Cruise Ship Medicine
• Typical week-long cruise with 1100
passengers: estimated average of
4 potentially life-threatening
conditions, with one patient
terminating the cruise early as a
result
95
96
Disaster
• World Health Organization: sudden
ecologic phenomenon of sufficient
magnitude to require external
assistance
• Overwhelms resources of region or
location in which it occurs
97
Disasters
• When normal ED procedures may
be interrupted by an event, there
must be policies and procedures in
place to activate a disaster
response, direct the mobilization of
personnel and equipment, and
permit rapid triage, assessment,
stabilization, and definitive care
98
Disasters
• External: physically separate from
hospital
– e.g., transportation, industrial
accident
• Internal: within confines of hospital
– e.g., bomb scare, laboratory accident
involving radiologic agents, power
failure, fire, etc.
99
Disaster Characteristics
• Event large number of minimally
injured patients presenting to the
nearest hospitals: minutes
• Then prehospital transport of most
affected patients to same hospitals:
peak at 2-3 hours
• ~80% self-transported by car, van,
police vehicle, cabs, foot, etc.
100
Joint Commission Requirements
• The Joint Commission (formerly
JCAHO) requires that member
hospitals have a written plan for
timely care of casualties arising
from both external and internal
disasters, and the hospital must
document the training and exercise
of these plans
101
Training / Disaster Drills
• Help familiarize staff with their
disaster roles and responsibilities
• Point out weaknesses or omissions
in the plans that require additions
or revisions
• The Joint Commission requires two
drills a year to reflect incidents
likely to occur in the community
102
Training / Disaster Drills
• From full-scale community-wide
simulations with moulage victims,
to tabletop triage scenarios, minidrills that test only certain
components of the disaster plan
(such as call-up of personnel), and
test of communications
103
Surge Capacity
• Ability to increase hospital bed
capacity over normal limits
• May include doubling patients in
rooms, converting acute care ward
to intensive care level unit, opening
previously closed wards, or caring
for patients in typically nonclinical
locations, such as the cafeteria
104
Communications System
• Good communications critical in
any disaster / mass casualty
• Without clear communications best
disaster plans fail
• Difficult to achieve for a variety of
reasons
• Cellular telephones, in particular,
are often overwhelmed in disasters
105
Communications System
• Disaster planning must include a
multi-tiered plan for communication
– Intrahospital: blackboard, two-way
radios, messengers/couriers
– Interhospital: citizen band groups,
cellular telephones, satellite
telephones, two-way radios
106
Decontamination
• Performed in area outside of
clinical care area of the ED
• Typically external to ED but may
be in internal locations
• Allow for removal of clothing and
cleansing of skin and hair of
patients exposed to a chemical or
radioisotope
107
Triage
• Patient entry restricted to only one
location, the triage area
• Primary function: rapid assessment
of incoming casualties, registration
and identification, assignment of
management priorities, distribution
to appropriate treatment areas
108
Treatment
•
•
•
•
•
Resuscitation
Minor treatment
Presurgical holding / surgical triage
Psychiatric care
Morgue facilities
109
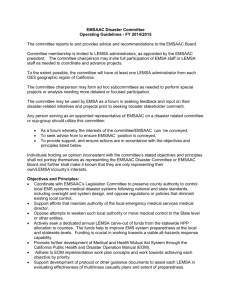
Field Triage
Start triage
Is patient breathing?
Yes
No
Open patient’s airway. Is
patient breathing?
≥30 breaths
per minute
No
Yes
Dead or dying
Immediate care
Immediate care
No
Control bleeding
Immediate care
No
Immediate care
< 30 breaths
per minute
Is radial pulse
present?
Yes
Assess mental
status. Can patient
follow commands?
Yes
Delayed care
110
ED Disaster Response
• Notify nurse / physician in charge
• Discharge / transfer nonemergent
• All available litters / wheelchairs to
ambulance entrance
• Security diverts nonessential
vehicles one way flow only
111
Disaster Triage at ED
• Triage establishes priorities for
care, determines clinical treatment
area
• Triage at ED entrance, even if
done at scene
• Do most good for greatest number
• Care at triage: manually opening
airway, control external bleeding
112
Disaster Triage at ED
• Most common triage classification
in U.S. assigns patient to colorcoded category depending on
injury severity and prognosis
– Red: first priority, most urgent
– Yellow: second priority, urgent
– Green: third priority, non-urgent
– Black: dead / expectant
113
Natural Disasters
Because standard amenities, such
as power, running water, and
sanitation methods may be
unavailable for extended periods of
time, all medical disaster planning
must include practical, simple
alternatives to technologies that are
likely to fail during a disaster.
114
Disease Burden: Trauma
• Acute phase: direct trauma from
collapsing structures, flying debris
• Second spike: clean-up phase
• Most is minor
• Adequate anesthesia, blood
products, surgical equipment and
ability to sterilize them, ICU
capacity, operating rooms
115
Disease Burden: Infections
• Combination of communicable
disease and population
malnutrition is major cause of
morbidity and mortality in most
disasters, with majority of deaths
occurring in acute postevent phase
116
Disease Burden: Infections
• Respiratory illness ~20% of natural
disaster deaths in children <5yo
• Flood / tsunami: aspiration
pneumonia from inhaled
contaminated water
• Most outbreaks several weeks
postdisaster, spreads through
shelters and settlement camps
117
Disease Burden: Infections
• Both disaster victims and rescue
workers at risk for respiratory
illness due to crowded conditions
and compromised sanitation
• Tuberculosis presents a special
challenge for public health officials
118
Disease Burden: Infections
• ~40% of deaths in acute postevent
phase (80% children): diarrhea
• Water quality and availability,
sanitation, and cleaning materials
• Incidence of GI disease often
peaks several weeks after disaster,
infections are generally mild
119
Disease Burden: Chronic
• Inability to properly control chronic
diseases, such as hypertension,
diabetes, asthma, or coronary
artery disease, may well be the
biggest unanticipated health threat
to a postdisaster population
120
Disease Burden: Mental
• Often-overlooked is psychological
burden
• Post Hurricane Katrina survivors:
rates of post-traumatic stress
disorder were 10 times expected
population incidence and on par
with rates in returning Vietnam War
veterans
121
122
Impairment
• Exists when physician’s
professional performance is
adversely affected due to illness
(physical or mental), aging,
alcoholism, chemical dependence
• Generally pattern rather than single
event
123
Impairment
• Prompt and careful intervention
• Perform immediately after
precipitant event
• Nonthreatening, nonjudgmental
confrontation
• Document impaired behaviors
• Plan intervention goals in advance
• Prevent relapse
124
Wellness
• Positive work environment
• Progressive shifts of reasonable
length (<10 hours)
• Management strategies for difficult
/ violent patients
• Strengthen / maintain interpersonal
relationships: family, social
• Be financially responsible
125
126
Observation Medicine
• Extension of ED services to
address unmet patient needs
• Observation: 80% of patients sent
home without hospitalization
• Cost to evaluate and treat is half
that incurred by admission
• in inadvertent release home of
patients with serious disease
127
Observation Medicine
• Designated area to provide shortterm services for up to 24 hours
• Chest pain unit, clinical decision
unit, rapid diagnostic treatment unit
• NOT a holding unit
– Patients admitted to hospital are held
passively until inpatient hospital bed.
128
Observation Medicine
Typical complaints for evaluation
• Abdominal pain
• Chest pain
• Deep vein thrombosis
• Upper gastrointestinal bleeding
• Syncope
• Transient ischemic attack
129
Observation Medicine
Typical complaints for treatment
• Asthma
• Atrial fibrillation
• Congestive heart failure
• Dehydration
• Pneumonia
• Pyelonephritis
130
Observation Medicine
Trauma complaints for observation
• Blunt abdominal injury
• Penetrating abdominal injury
• Blunt chest trauma
• Penetrating chest injury
131
Ultrasound
• Emergency ultrasound is one of
three competency assessments
required of EM residents by the
Residency Review Committee for
Emergency Medicine
132
Ultrasound
•
•
•
•
Trauma (FAST)
Pelvic
Cardiac
Abdominal
vascular
• Biliary
• Renal
• Extremity vascular
•
•
•
•
•
Thoracic / tracheal
Ocular
Soft tissue
Musculoskeletal
Transcranial
Doppler
• Testicular
• Procedure guidance
133
Multiculturism
• 2000: 12% of U.S. population
foreign born, 20% spoke language
other than English at home
• 2030: Hispanics will to 20%
• Racial and ethnic minorities in US
> 40%
134
Multiculturism
• Patients with limited English
proficiency more likely to defer
needed services, leave against
medical advice, miss
appointments, fail to adhere to
treatment regimens, lack a regular
provider
135
Disparities
• Hispanics and African Americans
receive fewer analgesics for
extremity fractures and for
musculoskeletal pain
• Opioids less likely to be prescribed
to African Americans (23%) and
Hispanics (24%) for pain relief than
whites (31%)
136
Disparities
• Mechanisms used to cope with
stress of racism shown to backfire
by adding to health risks: smoking,
substance abuse, overeating
• Disparities profiling can result in
both under- and overdiagnosis and
thus contribute to medical error
137
Alternative Care
• 1997: US population made ~629m
visits to alternative health care
providers
• 243 million more visits than to
conventional health care providers
• 44% used at least one
complementary alternative therapy
138
Role: The Good Patient…
…is acutely ill but waits patiently
until called without complaining,
requesting pain medications,
getting angry, or being disruptive
…understands the triage system and
provides a clear, concise, pertinent
history with enough information for
accurate diagnosis
139
Role: The Good Patient…
…does not take up physician time
with minor complaints, feelings, or
tangentially related information
…who does not speak English
brings someone to interpret,
someone who can bridge the
cultural divide and help with
transportation upon discharge
140
Role: The Good Patient…
…accepts invasive examinations
and procedures without protest,
agrees to admission or to a
discharge plan, does not require
long explanations of rationale for
treatment, and has a support
system in place for a safe
discharge
141
Role: The Good Patient…
…does not moan, scream for a
nurse or doctor, or act violently
…does not have family members
who are emotionally upset, stir up
trouble, or challenge providers
... share a trust, understanding, and
belief in scientific technological
medicine and its value
142
Role: The Good Patient…
…uses seat belts, maintains
personal hygiene and normal
weight, takes prescribed
medications, avoids drugs and
cigarettes, and exercises
…help maintain the flow through the
emergency department; “bad
patients” obstruct the flow
143
Role: The Good Patient…
…gets better
…“bad patients” keep coming back,
have chronic recurrent conditions,
and have confusing or difficult to
resolve problems
144
Why Do Patients Abuse Us?
1. Individuals seen in the ED don’t
need an appointment to get care
2. EDs provide sophisticated
medical technology
3. EDs operate 24 hours a day
4. ED services are often covered by
health insurance, while other
options are not
145
Why Do Patients Abuse Us?
5. EDs have a tradition of free care
6. Many communities lack culturally
competent private practitioners
7. EDs are often close to inner-city
neighborhoods, whereas many
primary care providers have
abandoned the city center
environs for the suburbs
146
147
Conclusions
• Significant overlap exists between
legal and ethical decision-making
• Physician owes duty to third party
when aware of reasonable risk to
that individual (Tarasoff)
• Capacity: individual’s ability to
make decision based on personal
values and comprehension of
consequences of that decision
148
Conclusions
• All states allow treatment of minors
for sexually transmitted diseases
• EMTALA mandates the all patients
must receive medical screening
exam and be stabilized before
transfer to another facility
• Failure to report an EMTALA
violation is itself a violation
149
Conclusions
• Competence is not the same as
capacity
• The four components of
malpractice are: duty, breach of
duty, harm, proximate cause
• Good communication skills
mitigates much malpractice
150
Conclusions
• On-scene physician who wishes to
direct care by EMS must be able to
prove identity and licensure
• Primary advantage of helicopter
transport is to reduce times
• Disaster is present when needs of
the casualties exceed available
resources
151
Conclusions
• Triage is classification of patients
into treatment priorities and is a
fluid process
• The guiding principle of disaster
triage: greatest amount of good for
the greatest number of people
• Four categories of triage: critical,
priority, delayed, expectant
152
Conclusions
• The Joint Commission requires two
disaster drills annually to reflect
incidents likely to occur in the
community
153
154