PATH PRESENTATION 2
advertisement

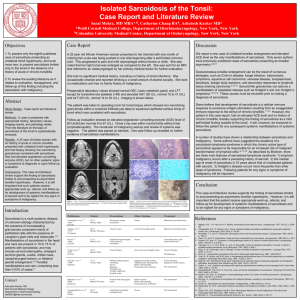
SARCOIDOSIS AKPABIO JESSICA 1003 INTRODUCTION Sarcoidosis is granulomatous disease(noncaseating in all tissues) 90% of cases involve hilar lymph nodes women are more affected than men peak ages 2535, 45-65. american blacks are affected 10 times more often than american whites PATHOGENESIS sarcoidosis is likely a disease of disordered immune response to genetically predisposed individuals to certain environmental agents evidence includes association with specific HLA genotypes eg HLA-A1 and HLA-B8 accumulation of oligoclonal activated CD4+ Tcells increased Th1 cytokine production(IL2 and interferone gamma) causing Tcell expansion and macrophage activation increased macrophage tumor necrosis factor(TNF) production leading to granuloma formation cutaneous anergy to common antigens eg tuberculin and candida polyclonal hypergammaglobulinemia MORPHOLOGY Granulomas are the characteristically noncaseating with tightly clustered epitheloid histiocytes and frequent multinucleate giant cells. schaumann bodies(laminated,calcified proteinaceous concretions) and asteroid bodies(stellate inclusions within giant cells) commonly occur but are not pathognomonic lungs exhibit diffuse,scattered granulomas,forming a reticulonodular pattern on x-ray films.pulmonary lesions tend to heal and only residual hyalinized scars may be seen lymph nodes are always involved commonly in the hilar and mediastinal regions tonsils are involved in 25-33% of cases spleen and liver are microscopically affected in 75% of patients (although gross splenomegaly and hepatomegaly occur in less than 20% of cases bone marrow involvement is seen in 20% of cases radiologically visible lesions have a pharyngeal predilection skin involvement occurs in 33% to 50% of patients as discrete subcutaneous nodules or erythematous scaling plaques or macules; mucous membrane lesions also occur eyes are affected in 20% to 50% of cases, including iritis,indocyclitis or choroid retinitis often with lacrimal gland inflammatory and reduced lacrimation,concurrent salivary gland involvement constitutes the Mikulicz syndrome PATHOPHYSIOLOGY T cells play a central role in the development of sarcoidosis, as they likely propagate an excessive cellular immune reaction. For example, there is an accumulation of CD4 cells accompanied by the release of interleukin (IL)–2 at sites of disease activity. This may manifest clinically by an inverted CD4/CD8 ratio. Pulmonary sarcoidosis is frequently characterized by a CD4+/CD8+ ratio of at least 3.5 in bronchoalveolar lavage fluid (BALF), although up to 40% of the cases present a normal or even decreased ratio, thus limiting its diagnostic value.Increased production of TH1 cytokines, such as interferon, is also a feature. Moreover, both tumor necrosis factor (TNF) and TNF receptors are increased in this disease. The importance of TNF in propagating inflammation in sarcoidosis has been demonstrated by the efficacy of antiTNF agents, such as pentoxifylline and infliximab,in treating this disease. In addition to T cells, B cells also play a role. There is evidence of B cell hyperreactivity with immunoglobulin production. Soluble HLA class I antigens levels in serum and BALF are higher in patients with sarcoidosis. These levels tend to be significantly higher in active than in inactive stages and correlate with angiotensin-converting enzyme (ACE) levels. Active sarcoidosis has also been associated with plasmatic hypergammaglobulinemia. B-cell accumulation has been shown in pulmonary lesions, and a beneficial effect with anti-CD20 monoclonal antibody therapy has been reported in select patients. Glycoprotein KL-6 and surfactant protein D (SP-D) derived from alveolar type II cells and bronchiolar epithelial cells are significantly increased in pulmonary sarcoidosis and correlate with the percentage of lymphocytes in BALF, reflecting an inflammatory response in sarcoidosis. However, there is no significant correlation between KL-6 or SP-D levels and chest radiography findings, ACE levels, or CD4/CD8 ratio in BALF. KL-6 has been shown to be predictive of increased pulmonary parenchymal infiltration. A study by Facco et al suggests that Th17 cells may play a role in the pathogenesis and progression of sarcoidosis; these cells were noted to be present in the blood, BALF samples, and lung tissue from patients with sarcoidosis, particularly in those with the active form of the disease. SYMPTOMS Symptoms vary according to what organ is infected they include generalized symptoms; fatigue fever swollen lymph node,weight loss lung symptoms; persistent dry cough, shortness of breath,wheezing,chest pain skin symptoms; blurred vision,eye pain, severe redness, sensitivity to light others include; swollen and painful joints nasal stiffness hoarse voice pain in hands and feet or other bony areas( due to formation of cyst in bones) SIGNS kidney stone formation enlarged liver arrhythmias pericarditis heart failure hearing loss meningitis seizures dementia depression Pulmonary findings on physical examination are as follows: • Usually normal • Crackles may be audible • Exertional oxygen desaturation may be present Dermatologic manifestations may include the following: • Erythema nodosum • A lower-extremity panniculitis with painful, erythematous nodules (often with Löfgren syndrome) • Lupus pernio (the most specific associated cutaneous lesion) • Violaceous rash on the cheeks or nose (common) • Maculopapular plaques (uncommon) Ocular involvement, which may lead to blindness if untreated, may manifest as follows: • Anterior or posterior granulomatous uveitis (most frequent) • Conjunctival lesions and scleral plaques Other possible manifestations are as follows: • Osseous involvement • Heart failure from cardiomyopathy (rare) • Heart block and sudden death • Lymphocytic meningitis (rare) • Cranial nerve palsies and hypothalamic/pituitary dysfunction (rare) Löfgren syndrome (fever, bilateral hilar lymphadenopathy, and polyarthralgias): Common in Scandinavian patients, but uncommon in African-American and Japanese patients ETIOLOGY Doctors don't know the exact cause of sarcoidosis. Some people appear to have a genetic predisposition to developing the disease, which may be triggered by exposure to specific bacteria, viruses, dust or chemicals. Researchers are still trying to pinpoint the genes and trigger substances associated with sarcoidosis. Normally, your immune system helps protect your body from foreign substances and invading microorganisms, such as bacteria and viruses. But in sarcoidosis, some immune cells collect in a pattern of inflammation called granulomas. As granulomas build up in an organ, the function of that organ can be affected. RISK FACTORS While anyone can develop sarcoidosis, factors that may increase your risk include: • Age and sex. Sarcoidosis often occurs between the ages of 20 and 40. Women are slightly more likely to develop the disease. • Race. African-Americans have a higher incidence of sarcoidosis than do white Americans. Also, sarcoidosis may be more severe and may be more likely to recur and cause lung problems in African-Americans. • Family history. If someone in your family has had sarcoidosis, you are more likely to develop the disease yourself. DIAGNOSIS • X-ray, to check for evidence of lung damage or enlarged lymph nodes in your chest,pulmonary infiltrates • CT scan, if complications are suspected. • PET or MRI, if sarcoidosis seems to be affecting your heart or central nervous system • Blood tests, to assess your overall health and how well your kidneys and liver are functioning. • Lung function tests, to measure lung volume and how much oxygen your lungs deliver to your blood. • Eye exam, to check for vision problems that may be caused by sarcoidosis. Staging of sarcoidosis is as follows: • Stage 0: Normal chest radiographic findings • Stage I: Bilateral hilar lymphadenopathy • Stage II: Bilateral hilar lymphadenopathy and infiltrates • Stage III: Infiltrates alone • Stage IV: Fibrosis Biopsies Your doctor may order a small sample of tissue (biopsy) be taken from a part of your body believed to be affected by sarcoidosis to look for the granulomas commonly seen in the condition. Biopsies can most easily be taken from your skin or the outer membrane of your eye. Tissue is sent to a laboratory for analysis. Lung biopsies or lymph node biopsies can be obtained through a procedure (bronchoscopy) in which a thin, flexible tube containing a camera is inserted down your throat. COMPLICATIONS • Lungs. Untreated pulmonary sarcoidosis can lead to irreversible damage to the tissue between the air sacs in your lungs, making it difficult to breathe. • Eyes. Inflammation can affect almost any part of your eye and can eventually cause blindness. Rarely, sarcoidosis also can cause cataracts and glaucoma. • Kidneys. Sarcoidosis can affect how your body handles calcium, which can lead to kidney failure. • Heart. Granulomas within your heart can interfere with the electrical signals that drive your heartbeat, causing abnormal heart rhythms and, in rare instances, death. • Nervous system. A small number of people with sarcoidosis develop problems related to the central nervous system when granulomas form in the brain and spinal cord. Inflammation in the facial nerves can cause facial paralysis. TREATMENT Steroid treatment Corticosteroids are the mainstay of therapy. Generally, prednisone given daily and then tapered over a 6-month course is adequate for pulmonary disease. Earlier recommendations suggested an initial dose of 1 mg/kg/d of prednisone; however, more recent expert opinions endorse a lower dose (eg, 40 mg/d), which is tapered to every-other-day long-term therapy over several weeks. In one study, treatment of acute exacerbations of pulmonary sarcoidosis with steroid doses as low as 20 mg of prednisone for a median of 21 days improved spirometry back to baseline and improved clinical symptoms.[54] Most patients who require long-term steroids can be treated using 10-15 mg of prednisone every other day. Some data suggest that corticosteroid use may be associated with increased relapse rates. However, data suggest early treatment of stage II sarcoidosis with oral prednisolone for 3 months followed by inhaled budesonide for 15 months improves 5-year pulmonary function and reduces the need for future steroid treatment.[55] High-dose inhaled corticosteroids may be an option, but conclusive data are lacking. Inhaled corticosteroids, in particular, can be used in patients with endobronchial disease. Although corticosteroids are used for symptom relief and remain the mainstay of therapy, their efficacy in this disease is unclear. Since many patients' conditions improve spontaneously, showing a true benefit to therapy requires a careful control arm. The best study addressing corticosteroids was the recently completed multicenter trial from Britain sponsored by the British Thoracic Society. In this nonrandomized study, 55 patients were selectively observed or treated with corticosteroids. Additionally, patients who were thought to have an immediate indication for steroids were treated. The trial required a 6-month run-in period to exclude patients who improved spontaneously. At the end of the trial, the groups treated with long-term steroids fared better on some measures than did the patients who were observed and treated with short bursts of steroids Nonsteroid treatment Noncorticosteroid agents are being increasingly tried. Common indications for the initiation of such agents include steroid-resistant disease, intolerable adverse effects, or patient desire not to take corticosteroids. Methotrexate (MTX) has been a successful alternative to prednisone and is a steroid-sparing agent. Chloroquine and hydroxychloroquine are antimalarial drugs with immunomodulating properties, which have been used for cutaneous lesions, hypercalcemia, neurological sarcoidosis, and bone lesions. Chloroquine has also been shown to be efficacious for the treatment and maintenance of chronic pulmonary sarcoidosis. Cyclophosphamide has been rarely used with modest success as a steroid-sparing treatment in patients with refractory sarcoidosis. Azathioprine is another second-line therapy, which is best used as a steroid-sparing agent rather than as a single-drug treatment for sarcoidosis. Chlorambucil is an alkylating agent that may be beneficial in patients with progressive disease unresponsive to corticosteroids.[8] Tumor necrosis factor-alpha (TNF-alpha) inhibitors. These medications are most commonly used to treat the inflammation associated with rheumatoid arthritis. They can also be helpful in treating sarcoidosis that doesn't respond to other treatments. e.g. infliximab, pentoxifylline CASE STUDY 29-year-old black woman was referred from a community hospital for evaluation of bilateral infiltrates on chest radiograph and worsening shortness of breath. She had had a few weeks of nonproductive cough, exertional dyspnea, fever, night sweats, and weight loss. She had had no clinical response to intravenous cefoperazone and oral trimethoprim/sulfamethoxazole. He had smoked one pack of cigarettes a week for 10 years. She had a history of multiple sexual contacts. She denied any history of tuberculous exposure, recent travel, or occupational exposure. Physical examination revealed a temperature of 100.6°F, respiratory rate 32/min, pulse rate 120/min, and blood pressure 120/80 mm Hg. She appeared ill and in obvious respiratory distress. Head, eye, ear, nose, and throat examination was unremarkable. The neck was supple with no lymphadenopathy. There were no rashes or skin lesions. Heart sounds were normal, with no murmurs or gallops. Bilateral crackles were present on chest auscultation. Examination of the abdomen, extremities, and neurologic function was unremarkable. Arterial blood gas measurements on room air were PaO2 47 mm Hg, PaCO2 33 mm Hg, and pH 7.41. Complete blood count revealed a hemoglobin value of 16.4 g/dL, white blood cell count 5,800/mm3(68.3% neutrophils, 16% lymphocytes, 12.2% monocytes, 2.1% eosinophils, 1.4% basophils), and platelet count 312,000/mm3. Serum urea nitrogen, creatinine, electrolytes, prothrombin time, and partial thromboplastin time were normal. Serum lactate dehydrogenase was 314 IU/L (normal, 100 to 205 IU/L), alkaline phosphatase was 241 IU/L (normal, 36 to 125 IU/L), aspartate aminotransferase was 48 IU/L (normal, 2 to 50 IU/L), and serum albumin was 3.1 g/dL. A chest radiograph revealed extensive bilateral parenchymal infiltrates, with bilateral pneumothorax and pneumomediastinum (Fig 1). High-resolution computed tomography (CT) of the chest revealed diffuse bilateral infiltrates with a ground glass appearance, bullous disease, areas of cavitation, and bilateral pneumothorax (Fig 2). Conventional CT of the chest revealed mild to moderate bilateral pleural effusion. No mediastinal or hilar lymphadenopathy was seen. Chest radiograph shows extensive bilateral parenchymal infiltrates with pneumothorax (white arrows) and pneumomediastinum (black arrows). High-resolution computed tomography of chest shows diffuse bilateral infiltrates with ground glass appearance, bullous disease, areas of cavitation, and bilateral pneumothorax. A face mask with inspired oxygen of 40% was provided. Admitting house staff initiated intravenous trimethoprim/sulfamethoxazole and oral prednisone 60 mg a day for possible Pneumocystis cariniipneumonia. A chest tube was inserted in the right pleural cavity. Pleural fluid analysis revealed a pH of 7.84, white blood cell count 7,449/mm3 (13% neutrophils, 86% lymphocytes, and 1% eosinophils), red blood cell count 141,000/mm3, total protein 6.5 g/dL (serum total protein, 8.5 g/dL), lactate dehydrogenase 504 IU/L (serum lactate dehydrogenase, 314 IU/L), and glucose 61 mg/dL (serum glucose, 79 mg/dL). Sputum, blood, and pleural fluid cultures were negative for microorganisms. Simple spirometry revealed severe restrictive lung impairment, with forced expiratory volume in 1 second (FEV1) of 1.34 L (42% predicted), forced vital capacity (FVC) of 1.51 L (41% predicted), and FEV1/FVC ratio of 89 (104% predicted). Open lung biopsy resulted in the diagnosis of sarcoidosis, and trimethoprim/sulfamethoxazole was discontinued. The patient showed dramatic clinical improvement after 4 weeks of oral prednisone 40 mg/day, with an improvement in restrictive lung impairment (FEV1 2.15 L [68% predicted], FVC 2.71 L [74% predicted], and FEV1/FVC 79% [93% predicted]). Follow-up chest radiograph revealed complete reexpansion of the lungs and near-resolution of the parenchymal disease, with no recurrence of pneumothorax to date. Recovery was complete, without sequelae on chest radiograph REFERENCES ROBBINS PATHOLOGY BY KUMAR, ABBAS INTERNAL MEDICINE BY DAVIDSON www.mayoclinic.org www.webmd.com www.emedicine.medscape.com