The Spinal
Cord, Spinal Nerves,
and Spinal Reflexes
The spinal cord
• Gross anatomy
– 3 layers of meninges
– Epidural space (fat & vessels)
– CSF – subarachnoid space
– Terminates at L1/2 vertebral level
(conus medullaris)
• Dura extends to S2 vertebral
level
– Connects via filum terminale &
denticulate ligaments (pia)
– 31 pairs of spinal nerves (mixed)
• cauda equina
– Cervical & lumbar enlargements
Lumbar Tap
Spinal Cord Anatomy
• Conus medullaris – terminal portion of the spinal cord
• Filum terminale – fibrous extension of the pia mater; anchors
the spinal cord to the coccyx
• Denticulate ligaments – delicate shelves of pia mater; attach
the spinal cord to the vertebrae
• Spinal nerves – 31 pairs attach to the cord by paired roots
– Cervical nerves are named for inferior vertebra
– All other nerves are named for superior vertebra
• Cervical and lumbar enlargements – sites where nerves
serving the upper and lower limbs emerge
• Cauda equina – collection of nerve roots at the inferior end of
the vertebral canal
Cross-Sectional Anatomy of the Spinal Cord
• Anterior median fissure – separates anterior funiculi
• Posterior median sulcus – divides posterior funiculi
The 3 Meningeal Layers
• Dura mater:
– outer layer of spinal cord
– subdural space:
• between arachnoid mater
and dura mater
• Arachnoid mater:
– middle meningeal layer
– subarachnoid space:
• between arachnoid mater
and pia mater
• filled with cerebrospinal
fluid (CSF)
• Pia mater:
– inner meningeal layer
Structures of the Spinal Cord
• Paired denticulate
ligaments:
– extend from pia mater to
dura mater
– stabilize side-to-side
movement
• Blood vessels:
– along surface of spinal pia
mater
– within subarachnoid space
Cross-sectional anatomy
• Gray matter (cell
bodies, neuroglia, &
unmyelinated
processes)
– Posterior horns (sensory,
all interneurons)
– Lateral horns
(autonomic, T1-L2)
– Anterior horns (motor,
cell bodies of somatic
motor neurons)
• Spinal roots
– Ventral (somatic &
autonomic motor)
– Dorsal (DRG)
Cross-sectional anatomy
• White matter
– 3 funiculi (posterior, lateral,
anterior)
• Ascending, descending,
transverse
– Consist of “tracts” containing
similarly functional axons
• All tracts are paired
• Most cross over (decussate)
at some point
• Most exhibit somatotopy
(superior part of the tracts
are more lateral that
inferior body regions)
• Most consist of a chain of 2
or 3 successive neurons
Gray Matter: Organization
•
•
•
•
Dorsal half – sensory roots and ganglia
Ventral half – motor roots
Dorsal and ventral roots fuse laterally to form spinal nerves
Four zones are evident within the gray matter – somatic sensory
(SS), visceral sensory (VS), visceral motor (VM), and somatic
motor (SM)
White Matter in the Spinal Cord
• Fibers run in three directions – ascending, descending,
and transversely
• Divided into three funiculi (columns) – posterior,
lateral, and anterior
• Each funiculus contains several fiber tracts
– Fiber tract names reveal their origin and destination
– Fiber tracts are composed of axons with similar functions
•
•
•
•
Pathways decussate (cross-over)
Most consist of two or three neurons
Most exhibit somatotopy (precise spatial relationships)
Pathways are paired (one on each side of the spinal
cord or brain)
White Matter: Pathway Generalizations
3 Connective Tissue Layers
• Epineurium:
– outer layer
– dense network of collagen
fibers
• Perineurium:
– middle layer
– divides nerve into fascicles
(axon bundles)
• Endoneurium:
– inner layer
– surrounds individual axons
Peripheral Distribution of Spinal Nerves
• Each spinal nerve
connects to the spinal
cord via two medial roots
• Each root forms a series of
rootlets that attach to the
spinal cord
• Ventral roots arise from
the anterior horn and
contain motor (efferent)
fibers
• Dorsal roots arise from
sensory neurons in the
dorsal root ganglion and
contain sensory (afferent)
fibers
Figure 13–7a
Spinal Nerves: Rami
• The short spinal nerves branch into three or
four mixed, distal rami
– Small dorsal ramus – to back
– Larger ventral ramus – to plexuses/intercostals
– Tiny meningeal branch – to meninges
– Rami communicantes at the base of the ventral
rami in the thoracic region – to/from ANS
Nerve Plexuses
• All ventral rami except T2-T12 form interlacing nerve
networks called plexuses
• Plexuses are found in the cervical, brachial, lumbar, and
sacral regions
• Each resulting branch of a plexus contains fibers from
several spinal nerves
• Fibers travel to the periphery via several different routes
• Each muscle receives a nerve supply from more than
one spinal nerve
• Damage to one spinal segment cannot completely
paralyze a muscle
Spinal Nerve Innervation: Back,
Anterolateral Thorax, and Abdominal Wall
• The back is innervated by
dorsal rami via several
branches
• The thorax is innervated
by ventral rami T1-T12 as
intercostal nerves
• Intercostal nerves supply
muscles of the ribs,
anterolateral thorax, and
abdominal wall
The 4 Major Plexuses of Ventral Rami
1.
2.
3.
4.
Cervical plexus
Brachial plexus
Lumbar plexus
Sacral plexus
Cervical Plexus
• The cervical plexus is formed
by ventral rami of
C1-C4 (C5)
• Most branches are cutaneous
nerves of the neck, ear, back
of head, and shoulders
• The most important nerve of
this plexus is the phrenic
nerve
• The phrenic nerve is the
major motor and sensory
nerve of the diaphragm
Brachial Plexus
• Formed by C5-C8 and T1
(C4 and T2 may also
contribute to this plexus)
• It gives rise to the nerves
that innervate the upper
limb
Trunks and Cords of Brachial Plexus
• Nerves that form brachial plexus originate from:
–
–
–
–
superior, middle, and inferior trunks
large bundles of axons from several spinal nerves
lateral, medial, and posterior cords
smaller branches that originate at trunks
Brachial Plexus: Nerves
• Axillary – innervates the
deltoid and teres minor
• Musculocutaneous – sends
fibers to the biceps brachii
and brachialis
• Median – branches to most
of the flexor muscles of
forearm
• Ulnar – supplies the flexor
carpi ulnaris and part of the
flexor digitorum profundus
• Radial – innervates
essentially all extensor
muscles
Lumbar Plexus
• Arises from (T12) L1-L4
and innervates the thigh,
abdominal wall, and
psoas muscle
• The major nerves are the
femoral and the
obturator
Sacral Plexus
• Arises from L4-S4 and
serves the buttock, lower
limb, pelvic structures,
and the perineum
• The major nerve is the
sciatic, the longest and
thickest nerve of the body
• The sciatic is actually
composed of two nerves:
the tibial and the common
fibular (peroneal) nerves
Nerve plexuses - Summary
• Cervical – C1-C4
– Phrenic nerve
• Brachial – C5 – T1 (roots/trunks/divisions/cords)
– Axillary, MC, median, ulnar, radial
• Lumbar – L1-L4
– Femoral, obturator
• Sacral – L4-S4
– Sciatic (common peroneal/tibial), pudendal
Dermatomes
• Area of skin innervated by the
cutaneous branches of a
single spinal nerve.
• All segments except C1 have
dermotomal distribution
• UE typically from C5-T1
• LE typically from L1-S1
Figure 13–8
5 Patterns of Neural Circuits in Neuronal Pools
1. Divergence:
–
spreads
stimulation to
many neurons
or neuronal
pools in CNS
2. Convergence:
–
brings input
from many
sources to
single neuron
Figure 13–13a
5 Patterns of Neural Circuits in Neuronal Pools
3. Serial processing:
–
moves information
in single line
4. Parallel processing:
–
moves same
information along
several paths
simultaneously
Figure 13–13c
5 Patterns of Neural Circuits in Neuronal Pools
5. Reverberation:
–
–
positive feedback mechanism
functions until inhibited
Figure 13–13e
Reflex activity
• 5 components of
a reflex arc
– Receptor
– Sensory neuron
– Integration center
(CNS)
– Motor neuron
– Effector
4 Classifications of Reflexes
1. By early development
–
Innate or Acquired
2. By type of motor response
–
Somatic or Visceral
3. By complexity of neural circuit
–
Monosynaptic or Polysynaptic
4. By site of information processing
–
Spinal or Cranial
Spinal Reflexes
• Range in increasing order of complexity:
– monosynaptic reflexes
– polysynaptic reflexes
– intersegmental reflex arcs:
• many segments interact
• produce highly variable motor response
Monosynaptic Reflexes
• Have least delay
between sensory
input and motor
output:
– e.g., stretch
reflex (such as
patellar reflex)
• Completed in
20–40 msec
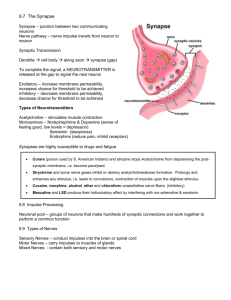
Muscle Spindles
• The receptors in stretch
reflexes
• Bundles of small,
specialized intrafusal
muscle fibers:
– innervated by sensory and
motor neurons
• Surrounded by extrafusal
muscle fibers:
– which maintain tone and
contract muscle
Postural Reflexes
• Postural reflexes:
– stretch reflexes
– maintain normal upright posture
• Stretched muscle responds by contracting:
– automatically maintain balance
Polysynaptic Reflexes
• More complicated than monosynaptic reflexes
• Interneurons control more than 1 muscle
group
• Produce either EPSPs or IPSPs
The Tendon Reflex
• Prevents skeletal muscles from:
– developing too much tension
– tearing or breaking tendons
• Sensory receptors unlike muscle spindles or
proprioceptors
Withdrawal Reflexes
• Move body part away
from stimulus (pain or
pressure):
– e.g., flexor reflex:
• pulls hand away from hot
stove
• Strength and extent of
response:
– depends on intensity
and location of stimulus
Reciprocal Inhibition
• For flexor reflex to work:
– the stretch reflex of antagonistic (extensor)
muscle must be inhibited (reciprocal inhibition) by
interneurons in spinal cord
Crossed Extensor Reflexes
• Occur simultaneously,
coordinated with flexor
reflex
• e.g., flexor reflex causes
leg to pull up:
– crossed extensor reflex
straightens other leg
– to receive body weight
– maintained by
reverberating circuits
Integration and Control
of Spinal Reflexes
• Though reflex behaviors are automatic:
– processing centers in brain can facilitate or inhibit
reflex motor patterns based in spinal cord
• Higher centers of brain incorporate lower,
reflexive motor patterns
• Automatic reflexes:
– can be activated by brain as needed
– use few nerve impulses to control complex motor
functions
– walking, running, jumping
Superficial reflexes
• Stroking of the skin elicits muscle contraction
– Involves functional upper motor pathways as well as cord level
reflex arcs
• Plantar reflex (L4-S2)…Babinski is normal in infants
– Usually indicative of CNS damage in adults
• Abdominal reflex (T8-T12)
– Absent with corticospinal lesion
Spinal Cord Trauma: Transection
• Cross sectioning of the spinal cord at any level
results in total motor and sensory loss in
regions inferior to the cut
• Paraplegia – transection between T1 and L1
• Quadriplegia – transection in the cervical
region
 0
0