(TDF/FTC) With DRV/r
advertisement
 With DRV/r")
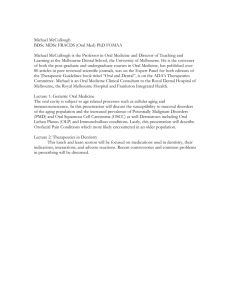
Maraviroc (MVC) Once Daily With Darunavir/Ritonavir (DRV/r) Compared to Tenofovir/Emtricitabine (TDF/FTC) With DRV/r: 48-Week Results From MODERN (Study A4001095) H.-J. Stellbrink,1 P. Pulik,2 J. Szlavik,3 D. Murphy,4 A. Lazzarin,5 J. Portilla,6 A. Rinehart,7 E. Le Fevre,8 A. Fang,9 S. Valluri,9 G. Mukwaya,10 J. Heera11 1ICH-Study Center, Hamburg, Germany; 2SPZOZ Wojewodzki Szpital Zakazny, Warsaw, Poland; 3Egyesittet Szent Istvan es Szent Laszio Korhaz-Rendelointezet, Budapest, Hungary; 4Clinique Medicale L'Actuel, Montreal, Canada; 5Ospedale San Raffaele, Divisione di Malattie Infettive, Milan, Italy; 6Hospital General Universitario de Alicante, Unidad de VIH, Alicante, Spain; 7-8ViiV Healthcare, 7Research Triangle Park, NC, USA; 8Brentford, United Kingdom; 9-11Pfizer Inc., 9New York, NY, USA; 10Medicines Development Group, New York, NY, USA; 11Groton, CT, USA 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Rationale for MVC + Boosted PI Regimen • Nucleoside toxicity-sparing • QD regimen/improved adherence • Low risk of resistance and preservation of treatment options if virologic failure occurs1 • Good penetration of MVC in CSF and genital secretions2-4 • MOTIVATE5 and PK studies support use of MVC 150 mg QD with selected ritonavir-boosted PIs6-8 • Prevalence of CCR5 tropic virus is greatest in treatment-naive individuals9 1. Portsmouth et al. IAC 2011. Abstract TUAB0103. 2. Tiraboschi et al. J Acquir Immune Defic Syndr. 2010;55:e35-e36. 3. Dumond et al. J Acquir Immune Defic Syndr. 2009;51:546-543. 4. Brown et al. J Infect Dis. 2011;203:1484-1490. 5. Jacqmin et al. CPT Pharmacometrics Syst Pharmacol. 2013;2:e64. 6. Vourvahis et al. IWCPHHT 2010, Abstract 37. 7. Calcagno et al. J Antimicrob Chemother. 2013;68:1686-1688. 8. Mora-Peris et al. J Antimicrob Chemother. 2013;68:1348-1353. 9. Hoffmann. Eur J Med Res. 2007;12:385-390. Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia . Study Design Trofile™ Phenotypic Assay (Monogram Biosciences) CCR5 tropic 1:1 randomization to treatment n≈402 TDF/FTC + MVC QD PBO + DRV/r (800/100 mg QD) 1:1 randomization to treatment n≈402 TDF/FTC + MVC QD PBO + DRV/r (800/100 mg QD) MVC (150 mg QD) + TDF/FTC QD PBO + DRV/r (800/100 mg QD) Screening Visit 1:1 randomization to tropism assay N≈1608 Genotypic Tropism Assaya (Siemens Healthcare Diagnostics) CCR5 tropic Screening (6 weeks) Eligibility Criteria • Antiretroviral treatment naive • Plasma HIV-1 ≥ 1000 c/mL • CD4 ≥ 100 cells/mm3 • No evidence of resistance to DRV, TDF, FTC • ≥ 18 years of age MVC (150 mg QD) + TDF/FTC QD PBO + DRV/r (800/100 mg QD) 0 48 wk Primary analysis 96 wk • Phase 3, randomized, double-blind • Primary endpoint: proportion of subjects with HIV-1 RNA <50 c/mL at wk 48 (MSDF)b by FDA snapshot algorithm • Non-inferiority study (NI margin of 10% between treatment groups) • 195 sites in 22 countries • Study was terminated on 04 Oct 2013 upon recommendation of IDMC aSiemens bMSDF: HIV-1 Coreceptor Tropism Assay is for research use only. Missing, Switch, Discontinuation = Failure. Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Subject Disposition Screening Visit 1:1 randomization to tropism assay N=1423 CCR5 tropic Received ≥ 1 dose of study drug n=797 TDF/FTC + DRV/r n=401 351 ongoing at 48-week analysis MVC + DRV/r n=396 323 ongoing at 48-week analysis Discontinuation All Screen Failures n=610a • 552 did not meet entrance criteria • 220 non-R5 virus • 264 tropism not reportable • 68 other criteria not met • 57 other reasons for screening failureb MVC TDF/FTC Adverse events 19 18 Insufficient clinical response 33 8 Lost to follow-up 8 7 No longer willing to participate 6 8 Other 7 9 73 50 TOTAL Screening (6 weeks) 0 48 wk Primary analysis 96 wk *Siemens HIV-1 Coreceptor Tropism Assay is for research use only. aAn additional 16 subjects were excluded from the study after the first randomization, but did not receive any study drug (total exclusions, n=626). bIncluded AE (n=1), lost to follow up (n=7), no longer willing to participate (n=20), protocol deviations (n=3), other (n=27). Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Baseline Characteristics MVC + DRV/r (n=396) TDF/FTC+ DRV/r (n=401) 37.0 (18–72) 35.0 (18–70) Male, n (%) 360 (90.9) 367 (91.5) Race, n (%) White Black Other 322 (81.3) 60 (15.2) 14 (3.5) 326 (81.3) 55 (13.7) 20 (5.0) Median CD4+ count, cells/mm3 (range) 352 (86–1295) 345 (34–1177) 38 (9.5) 45 (11.2) 4.42 (2.93–6.36) 4.42 (2.68–6.47) HIV-1 RNA ≥100,000 copies/mL, n (%) 81 (20.5) 83 (20.7) Clade, n (%) B Non-B 342 (86.4) 54 (13.6) 354 (88.3) 47 (11.7) Median age, years (range) CD4+ count <200 cells/mm3, n (%) Mean HIV-1 RNA, log10 copies/mL (range) Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Virologic and Immunologic Response Proportion of subjects with HIV-1 RNA <50 copies/mL TDF/FTC 86.8% 348/401 subjects MVC 77.3% 306/396 subjects Adjusted treatment difference (95% CI): -9.5% (-14.8%, -4.2%) BL 4 8 12 16 20 24 36 48 Week Mean CD4+ cell count changes at Week 48 (mean ± SD, cells/mm3) MVC + DRV/r 195.3 ± 175.7 TDF/FTC + DRV/r 193.9 ± 175.7 Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Proportion of subjects with HIV-1 RNA <50 copies/mL (%) Treatment Response at Week 48 by Key Subgroups No. of subjects Total 253 282 315 318 Baseline HIV-1 RNA 53 66 81 83 25 40 38 45 121 142 159 161 101 100 127 118 59 66 72 77 Baseline CD4+ Cell Count Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Comparable MVC Responses Were Observed in Populations Screened by Genotype and Trofile™ 146/181 (80.7%) 160/215 (74.4%) Genotype Trofile • The adjusted difference was 6.9% in the MVC arm in favor of the genotype assay (95% CI -1.3%, 15%) • There was no difference in response rate between assays in the TDF/FTC arm (160/185 [86.5%], genotype; 188/216 [87.0%], Trofile) Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Subjects with Protocol-Defined Treatment Failure (PDTF: Time of Failure) Subjects with PDTF, n (%)a HIV-1 RNA copies/mL at PDTF, n 50 to 200 201 to 400 401 to 1000 1001 to 10,000 10,001 to 50,000 MVC + DRV/r TDF/FTC + DRV/r (n=396) (n=401) 40 (10.1) 13 (3.2) 22 5 8 4 1 10 0 1 0 2 • Majority of subjects with PDTF (MVC + DRV/r, 68%; TDF/FTC + DRV/r, 77%) had HIV-1 RNA <400 copies/mL at PDTF • 7 subjects in both arms achieved HIV-1 RNA <50 copies/mL at last dose • No treatment-emergent resistance to any study drug was observed a • • • • • • Protocol-defined treatment failure criteria: Decrease in plasma HIV-1 RNA <1 log10 from baseline after Week 4, unless plasma HIV-1 RNA is <50 copies/mL, or Plasma HIV-1 RNA >1.0 log10 above the nadir value after Week 4, where the nadir is the lowest plasma HIV-1 RNA concentration, or Plasma HIV-1 RNA ≥50 copies/mL at any time after Week 24, or Plasma HIV-1 RNA ≥50 copies/mL after suppression to <50 copies/mL on two consecutive visits, or Decrease in plasma HIV-1 RNA <2 log10 from baseline on or after Week 12, unless plasma HIV-1 RNA is <50 copies/mL (post Amendment 2) and <400 copies/mL (post Amendment 3) All PDTFs required confirmation within 28 days of the initial event. Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract #. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Treatment-Emergent Adverse Events, Malignancies, and Laboratory Abnormalities MVC + DRV/r Most common AEs (>5% of subjects), n (%) Diarrhea Nasopharyngitis Upper respiratory tract infection Rash Nausea Fatigue Cough Bronchitis Gastroenteritis Depression Insomnia Malignancies, n (%) Grade 3/4 laboratory abnormalities, n (%) Alanine aminotransferase (ALT) Total bilirubin Creatine kinase Cholesterol (n=396) TDF/FTC + DRV/r (n=401) 81 (20.5) 40 (10.1) 36 (9.1) 32 (8.1) 29 (7.3) 26 (6.6) 24 (6.1) 23 (5.8) 20 (5.1) 18 (4.5) 14 (3.5) 7 (2.0)a 130 (32.4) 47 (11.7) 33 (8.2) 25 (6.2) 42 (10.5) 40 (10.0) 26 (6.5) 21 (5.2) 15 (3.7) 26 (6.5) 25 (6.2) 2 (0.7)b 7 (1.8) 3 (0.8) 13 (3.3) 8 (2.0) 5 (1.3) 1 (0.2) 14 (3.5) 6 (1.5) aMVC: Kaposi’s Sarcoma (n = 3), Castleman’s Disease (n = 1), Basal Cell Carcinoma (n = 1), Hodgkin’s Lymphoma (n = 2; one case assessed as possibly treatment-related by investigator). bTDF/FTC: Kaposi’s Sarcoma (n=1), Testis Cancer (n=1) Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Summary and Conclusions • MVC 150 mg QD in 2-drug therapy regimen demonstrated statistically lower • • • • rates of viral suppression when compared to a 3-drug regimen of TDF/FTC + DRV/r in antiretroviral-naive subjects over 48 weeks – IDMC recommended that the study be terminated in October 2013 Within each arm, there was comparable efficacy by tropism assay used for screening The majority of PDTFs failed with HIV-1 viral load <400 copies/mL There was no treatment-emergent resistance in either arm There was comparable safety and no unexpected safety findings • The efficacy of MVC + PI/r as stable switch therapy is under evaluation in the ongoing MARCH study Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Acknowledgments • Subjects and their supporters • Charles Craig, Research Virology Consulting and The Research Network • Marilyn Lewis, The Research Network • Colleagues at ViiV Healthcare and Pfizer Stellbrink et al. IAC 2014; Melbourne, Australia. Abstract TUAB0101. 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia Acknowledgments: MODERN Study Investigators Dr Jose Maria Gatell Artigas Daniel Podzamczer Palter Dr Joaquin Portilla Sogorb Dr Juan Julian Gonzalez Garcia Assoc Prof Antonio Rivero Roman Prof Dr Gerd Faetkenheuer Dr Andreas Plettenberg Prof Dr Johannes Richard Bogner Prof Dr Juergen K Rockstroh Prof Dr Jan van Lunzen Dr Heiko Karcher Prof Dr Hans-Juergen Stellbrink Dr Howard Alan Grossman Dr Javier Osvaldo Morales-Ramirez Dr David Michael Asmuth Dr David Michael Mushatt Dr Melanie Ann Thompson Dr Joan M. Duggan Dr Christopher Michael Polk Dr William Keith Henry Dr Miguel M. Mogyoros Catherine Butkus Small Dr Shubha J. Kerkar Dr Carl Jack Fichtenbaum Dr Paul Alan Benson Dr William David Hardy Dr Roberto Baun Corales Dr Armin Rieger Dr Gordon Elwood Crofoot Jr. Dr Michael Grant Sension Dr Jihad Slim Dr Jacek Gasiorowski Professor. Dr Waldemar Halota Dr Rodger David MacArthur Dr Jan Sven Fehr Dr Marcel Stoeckle Eugénio Teofilo Dra. Rosário Serrao Dr Teresa Branco Dr Emanuel G. Vlahakis Stephen Kegg Dr Christoph Stephan Dr Edmund Lydons Wilkins Dr Jason Andrew Flamm Dr Janos Szlavik Dr Chloe Meave Orkin Dr Stephen Eliot Follansbee Dr Alan Hinwai Man Dr Keikawus Arasteh Dr Gabriele L. Knecht Dr Hans Jaeger Dr Dushyantha Thilak Jayaweera Dr Robin Henry Dretler Dr Lizette Santiago Dr Jennifer Christy Bartczak Dr Steven Santiago Dr Jose Andres Montero Dr Gary Blick Dr Bienvenido Gamulo Yangco Dr Norman Peter Markowitz Dr David Michael Parenti Dr Margaret Ann Fischl Alyssa Shon Dr Dawd Said Siraj Dr Mamta K. Jain Dr Barbara Heeter Wade Dr Bruce Stephen Rashbaum Dr Barbara J. Hanna Dr Catherine Maria Creticos Dr Shannon Ray Schrader Dr Louis Marshall Sloan Dr Craig Allan Dietz Dr Jerome A. Ernst Dr Carmen D. Zorrilla Dr Michael Bruce Wohlfeiler Dr Ruth Soto-Malave Dr Thomas Bryan Campbell Dr Jeffery Linn Meier Dr Julia Betzabe Garcia-Diaz Dr Peter Gregory Gulick Dr Michael John Kozal Dr Susan Swindells Dr Sharon Lynn Walmsley Dr Daniel B. Murphy Dr Jean-Guy Baril Dr Jason Brunetta Dr Jonathan Benjamin Angel Dr Brian Conway Dr David Philip Wright Dr Anthony Martin Mills Dr Ivan Melendez-Rivera Dr Clifford Arbery Kinder Dr Kathleen King Casey Dr Joseph Clayton Gathe Jr Dr Donna Mildvan Dr Jorge Ernesto Rodriguez Dr Babafemi Olapoju Taiwo Dr Michael Switow Saag Dr Peter P. Shalit Dr Daniel Jay Skiest Prof Dr Hansjakob Furrer Prof Dr Pietro Vernazza Dr Jan Gerstoft Svend Stenvang Pedersen Matti Ristola Prof Jacques Reynes Dr Antoine Cheret Dr Jean-Michel Molina Prof Christine Katlama Prof Pierre-Marie Girard Dr Lelia Escaut Prof Francois Raffi Dr Laurent Cotte Prof Clifford L. Leen Dr Christiane Cordes Dr David Rey Dr Gilles Olivier Pialoux Dr Mark T. Bloch Prof Ilja Mohandas Hoepelman Dr Mark Richard Nelson Dr Piotr Pulik Dr Lars R. Mathiesen Dr David Alfred Baker Dr Mark Denis Kelly Prof Margaret Anne Johnson Dr Manuela Doroana Dr Daniel Benjamin Klein Prof Yves Levy Prof Philippe Morlat Dr Thierry Prazuck Dr Ian Geoffrey Williams Dr Stephen Taylor Juan Berenguer Berenguer Dr Martin J. Fisher Dr Anders Thalme Dr Hernando Knobel Freud Prof Nathan Clumeck Prof Bernard Vandercam Prof Dr Michel Moutschen Dr Kinda Schepers Prof Dr Linos Vandekerckhove Dr Eric Florence Prof Magnus Gisslen Prof Andrew Carr Dr Tim Read Dr Leo Flamholc Dr Pere Domingo Pedrol Dr Julian HJ Elliott Dr Anders Blaxhult Maria Jose Rios Villegas Prof Patrick Yeni Prof Adriano Lazzarin 20th International AIDS Conference; July 20-25, 2014; Melbourne, Australia