Caulfield - Cranial Nerves
advertisement

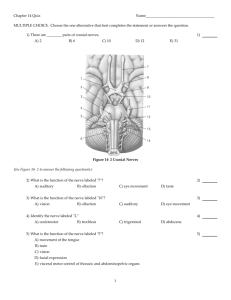
Clivus Bone Metastasis: Review of Cranial Nerves Morning Report July 8, 2009 Chris Caulfield Clivus Bone Clivus Metastases: Report of seven patients and literature review Of 46 patients that had surgery for clivus bone tumors in a 12 year period, seven patients proved to have metastasis Wide variety of primary tumors: Lung Adenocarcinoma (2) Prostate Carcinoma (2) Skin Melanoma (1) HCC (1) Lung Squamous Cell Carcinoma (1) Clivus Metastases: Report of seven patients and literature review All patients had Sixth Cranial Nerve Palsy Also had presentation with palsy of CN VII, XII, and headaches Upon further literature review, 27 additional examples were identified with prostate and thyroid being most common In spite of radiotherapy and chemotherapy, the mean survival was 12 months CRANIAL NERVES CRANIAL NERVES Olfactory Nerve (CN I) — examined by having the patient occlude one nostril and identify a common strong scent (coffee, peppermint, cinnamon). Optic Nerve (CN II) – examined by performing Visual Fields (all four quadrants of each eye), Visual Acuity (using Snellen Eye Chart/Card), and Fundoscopy (evaluate optic disc and retinal vessels). Pupillary Light Reflex. Evaluate papillary constriction with direct response and consensual response of opposite eye. CRANIAL NERVES Extraocular Movements: Oculomotor Nerve (CN III), Trochlear Nerve (IV), Abducens Nerve (VI) Oculomotor Nerve (CN III): evaluate for ptosis as it controls the striated muscle in levator palpebrae superioris Controls all extraocular muscles except for the superior oblique muscle and the lateral rectus muscle (“Down and Out”) Ptosis and “Down and Out” CRANIAL NERVES Extraocular Movements: Oculomotor Nerve (CN III), Trochlear Nerve (IV), Abducens Nerve (VI) Oculomotor Nerve (CN III): evaluate for ptosis as it controls the striated muscle in levator palpebrae superioris Controls all extraocular muscles except for the superior oblique muscle and the lateral rectus muscle (“Down and Out”) Edinger-Westphal nucleus supplies parasympathetic fibers to the eye via the ciliary ganglion, controlling the sphincter pupillae muscle (affecting pupil constriction) and the ciliary muscle (affecting accomodation). Pupillary Light Reflex CRANIAL NERVES Trochlear Nerve (CN IV): innervates the superior oblique muscle of the eye; nerve palsy usually causes horizontal diplopia Abducens Nerve (CN VI): innervates the lateral rectus muscle of the eye, nerve palsy usually causes diplopia Diplopia CN IV CN VI CRANIAL NERVES Trigeminal Nerve (CN V) is responsible for sensation in the face as well as the motor function of mastication Ophthalmic nerve (CN V1) carries sensory information from the scalp and forehead, the upper eyelid, and the nose (including the tip of the nose). Maxillary nerve (CN V2) carries sensory information from the lower eyelid and cheek, the upper lip, the upper teeth and gums, the palate and roof of the pharynx. Mandibular nerve (CN V3) carries sensory information from the lower lip, the lower teeth and gums, the chin and jaw. Dermatome Distribution of the Trigeminal Nerve CRANIAL NERVES Facial Nerve (CN VII) controls muscles of facial expression, and via the chorda tympani nerve, supplies parasympathetic fibers to submandibular glands and sublingual glands as well as taste sensation to anterior two-thirds of the tongue. Perform wrinkling of the brow, closing eyes tightly, smiling, puffing out the cheeks to test branches of the facial nerve. With an UMN, only the lower part of the face on the contralateral side will be affected, due to the bilateral control to the upper facial muscles. With a LMN, complete CN VII palsy resulting in both upper and lower facial weakness on the same side of the lesion (Bell’s palsy) LMN vs UMN Lesion CRANIAL NERVES Vestibulocochlear Nerve (CN VIII) responsible for transmitting sound and balance; assess by holding fingers a few inches away from ear canal and rubbing them together softly. Glossopharyngeal Nerve (CN IX) receives sensory fibers from oropharynx and special sensory fibers of taste from the posterior one-third of the tongue; sends motor fibers to palate and is responsible for gag reflex. Vagus Nerve (CN X) sends motor fibers to palate and parasympathetic fibers down to second segment of the transverse colon. Nerve palsy results in hoarse voice, difficulty in swallowing, loss of gag reflex, and uvula deviation away from side of lesion. Palatal movement (CN IX and X) — Ask the patient to say "aaah" and observe whether the two sides of the palate move fully and symmetrically. CRANIAL NERVES Spinal Accessory Nerve (CN XI) — responsible for head rotation and shoulder elevation by innervating the sternocleidomastoid and trapezius muscles. Nerve palsy results in ipsilateral loss of muscle function and could also result in atrophy or fasciculations. Hypoglossal Nerve (CN XII) — responsible for tongue movement; if there is loss of function/unilateral paralysis, the tongue will deviate toward the affected side. Spinal Accessory Nerve Hypoglossal Nerve Palsy How do these neurological deficits relate? Right Eye Ptosis Weakness of Facial Muscles on Right Tongue Deviation to the Right Side Vision Problems on Right Side/Diplopia Miosis Loss of Taste Dysarthria How are these presentations of ptosis different? How are these presentations of ptosis different? Horner’s Syndrome CN III Palsy PTOSIS Important to distinguish the ptosis caused by Horner's syndrome from the ptosis caused by an oculomotor (CN III) palsy. Horner’s Syndrome: ptosis occurs with a constricted pupil, due to a loss of sympathetics to the eye. CN III Palsy: ptosis occurs with a dilated pupil, due to a loss of innervation to the sphincter pupillae muscle. HORNER’S SYNDROME Lesion anywhere along the sympathetic pathway causing classic neurological signs of ptosis, miosis, and anhidrosis Arm pain and/or hand weakness typical of brachial plexus lesion suggests a lesion in the lung apex Pancoast Tumor involves the lung apex and causes compression of a sympathetic ganglion HORNER’S SYNDROME