Invacare Matrx Back Power Point

Dedicated to seating and mobility solutions
• Assist wheelchair users in achieving their goals
• Respect lifestyle, function, posture, skin protection
• Provide simple, effective and safe seating solutions
Invacare Matrx Seating objectives
• Encourage postural stability and allow for functional movement
• Promote activity and support healthy resting postures
• Work for optimal support and pressure distribution
• Use additional external components only as needed.
Invacare Matrx Guiding Principles
• Consider breathing and swallowing
• Secondary complications: tissue trauma, pain, deformities, and contractures
• A full evaluation
• The position of the pelvis directly impacts the spine (and head, extremities)
• The pelvis is the foundation for seated function
• Determine if a posture is fixed or flexible
• Test seating solutions in motion
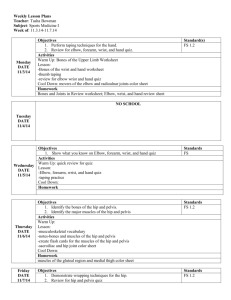
POSTERIOR PELVIC TILT WITH KYPHOSIS
POSTERIOR PELVIC TILT WITH HYPERKYPHOSIS
CLINICAL
Presentation
Hyperextesion of neck to elevate head
Shoulder blades slide forward and apart, impeding shoulder elevation
Flattened lumbar spine and hyperkyphosis of the thoracic spine
IT’s slide forward
Pelvis tilts posteriorly resulting in increased load on the sacrum
POSTERIOR PELVIC TILT WITH HYPERKYPHOSIS
Potential Causes
Wheelchair fit
Seat depth too long/short
Foot rest too high/low
Inadequate support for sacrum
In manual wheelchair, hard to reach wheels
Seat-to-floor height too high/low
Clinical
High or low tone in upper body
Limited hip flexion (< 90 degrees )
Weak muscles: abdominals/back extensors
Shortened/tight hamstrings
Lack of balance/postural control
POSTERIOR PELVIC TILT WITH HYPERKYPHOSIS
POTENTIAL
Solution
Flexible posture
Possible use of harness
Possible use of table/tray
Contoured cushion helps stabilize the pelvis in a neutral position
Stable back support that stabilizes the pelvis at the PSIS
Place a positioning belt beneath the ASIS or across thighs
POSTERIOR PELVIC TILT WITH HYPERKYPHOSIS
POTENTIAL
Solution
Fixed posture Use tilt to increase trunk extension and improve visual field
Contoured cushion to support the pelvis
Provide a contoured back to match shape of spine
Utilize lateral support for increased immersion and pressure distribution
If hip flexion is limited, open the back angle and/or adjust the cushion to achieve a level pelvis
ANTERIOR PELVIC TILT WITH HYPERLORDOSIS
ANTERIOR PELVIC TILT WITH HYPERLORDOSIS
CLINICAL
Presentation
Trunk overextended to prevent forward collapse
Pelvic to thigh angle less than 90 degrees
Possible that shoulder blades are pulled tightly together to maintain an upright position, limiting arm function
Increased lumbar curve and decreased contact with the back support
Pelvis tilted anteriorly (forward)
ANTERIOR PELVIC TILT WITH HYPERLORDOSIS
Potential Causes
Wheelchair Fit
Back support too upright
Excessive lumbar contouring
Clinical
Tight quadriceps/hip flexors
Weak abdominal musculature
Obesity
ANTERIOR PELVIC TILT WITH HYPERLORDOSIS
POTENTIAL
Solution
Flexible posture
Consider a chestbelt or harness
Make small, gradual changes to seat and/or back angle to reposition the pelvis and spine into a neutral position
Lower back support to tailbone to balance curvature of the lower spine
ANTERIOR PELVIC TILT WITH HYPERLORDOSIS
POTENTIAL
Solution
Fixed posture
Extra foam insert can be added to increase contact and contour
Angle back support forward to compensate limited hip extension
Lower rear seat height to help balance the trunk over the pelvis in an upright position
PELVIC OBLIQUITY AND SCOLIOSIS
PELVIC OBLIQUITY AND SCOLIOSIS
CLINICAL
Presentation
The spine is influenced by pelvic asymmetry, resulting in a scoliosis.
The lumbar curve will be convex on the oblique
(lower) side of the pelvis
One shoulder often higher on the weightbearing side
Palpation of the Iliac crest reveals that one side of the pelvis is lower than the other
Increased risk for pressure sore on lower IT
PELVIC OBLIQUITY AND SCOLIOSIS
Potential Causes
Wheelchair fit
Sling or stretched seat upholstery
Seat width too wide and/or arm supports too low
Cushion does not offer adequate support/contouring
Back angle does not accommodate for limited hip flexion
Back support too wide
Clinical
Pain
Issues with muscle tone/weakness
Limitations of hip movement
Scoliosis
PELVIC OBLIQUITY AND SCOLIOSIS
POTENTIAL
Solution
Flexible posture
Lateral support
Lateral support
Lateral trunk supports can be used to provide 3 or 4 points of support
Alternate approach – Deep contoured back with built-in support
Lateral support
Build up the cushion under the lower IT to balance obliquity
PELVIC OBLIQUITY AND SCOLIOSIS
POTENTIAL
Solution
Fixed posture
Backrest must be deep enough to support the trunk and may have to be mounted in a rotated position
Build up under the higher IT to balance weightbearing
PELVIC ROTATION
PELVIC ROTATION
CLINICAL
Presentation
One hip is usually adducted and internally rotated
One ASIS and hip is further forward in the seat
One hip is usually abducted and externally rotated
Note that asymmetry in the forward position of the knees can also be due to leg length discrepancy or a dislocated hip
PELVIC ROTATION
Potential Causes
Wheelchair fit
Poor wheel placement on manual chair
Seat-to-floor height too high for foot propulsion
Clinical
Limited hip flexion, abduction, adduction
Leg length discrepancy and/or dislocated /subluxed hip
Unable to reposition after foot propulsion
PELVIC ROTATION
POTENTIAL
Solution
Flexible posture
Contoured cushion helps stabilize the pelvis in a neutral position
In order to maintain a functional head and shoulder position, you may need to allow for some asymmetry in the pelvis
Align the pelvis and lower the backrest to stabilize at the PSIS level.
A pelvic positioning belt can help maintain hip alignment
PELVIC ROTATION
POTENTIAL
Solution
Fixed posture
Positioning the backrest so that it follows the contours of the pelvis will increase the surface contact area, give more support, and help prevent further rotation.
Consider using a cushion that can be adapted to accommodate functional leg length discrepancy
HIP ABDUCTION
HIP ABDUCTION
CLINICAL
Presentation
Can be on one or both sides
Movement of the femur away from midline
Legs are wide apart –
Can cause pressure against legrests.
HIP ABDUCTION
Potential Causes
Low or high tone
Shortened abductor muscles
Obesity
Inadequate seat depth
Seat width too wide
Posterior tilt in pelvis
HIP ABDUCTION
POTENTIAL
Solution
Flexible: Use a contoured cushion to support the pelvis in a neutral position.
If needed, use additional lateral support to realign the femurs
Fixed: Adapt a contoured cushion so that it conforms to the user’s posture. Modify the wheelchair configuration to prevent secondary pressure issues.
HIP ADDUCTION
HIP ADDUCTION
CLINICAL
Presentation
Movement of the femur toward the midline
HIP ADDUCTION
Potential Causes
Hammock effect from sling upholstery
High tone
Shortened/overactive hip adductors
Anterior tilt in pelvis
HIP ADDUCTION
POTENTIAL
Solution
Flexible: Use a contoured cushion that enhances abduction
Fixed: Modify abductor height to prevent pressure build up between knees
Cushion ridgidizer contoured to eliminate
“hammock effect” of sling upholstery