Blood and Blood Vessels
advertisement

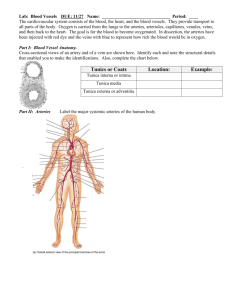
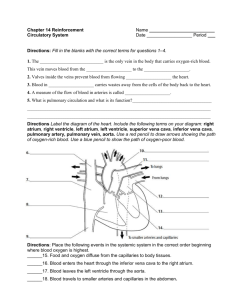
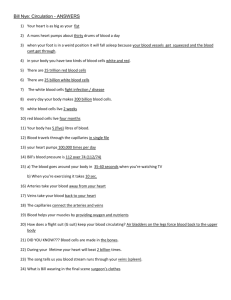
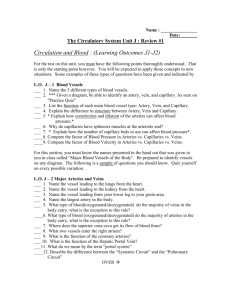
Blood and Blood Vessels Module 17.3: Red blood cell production and recycling • RBC production and recycling • Events occurring in red bone marrow • Blood cell formation (erythropoiesis) occurs only in red bone marrow (myeloid tissue) • Located in vertebrae, ribs, sternum, skull, scapulae, pelvis, and proximal limb bones • Fatty yellow bone marrow can convert to red bone marrow in cases of severe, sustained blood loss • Developing RBCs absorb amino acids and iron from bloodstream and synthesize Hb Module 17.3: Red blood cell production and recycling • Stages • Proerythroblasts • Erythroblasts • Actively producing Hb • After four days becomes normoblast • Reticulocyte (80% of mature cell Hb) • Ejects organelles including nucleus • Enters bloodstream after two days • After 24 hours in circulation, is mature RBC Module 17.3: Red blood cell production and recycling • Events occurring at macrophages • Engulf old RBCs before they rupture (hemolyze) • Hemoglobin recycling • Iron • Stored in phagocyte • Released into bloodstream attached to plasma protein (transferrin) • Globular proteins disassembled into amino acids for other uses • Heme biliverdin bilirubin bloodstream • Hemoglobin not phagocytized breaks down into protein chains and eliminated in urine (hemoglobinuria) Module 17.3: Red blood cell production and recycling • Events occurring at liver • Bilirubin excreted into bile • Accumulating bile due to diseases or disorders can lead to yellowish discoloration of eyes and skin (jaundice) • Events occurring at the large intestine • Bacteria convert bilirubin to urobilins and stercobilins which become part of feces • Give feces yellow-brown or brown coloration Module 17.3: Red blood cell production and recycling • Events occurring at kidneys • Excrete some hemoglobin and urobilins • Give urine its yellow color • Presence of intact RBCs in urine (hematuria) • Only after urinary tract damage Events Occurring in the Red Bone Marrow Start Developing RBCs absorb amino acids and Fe2+ from the bloodstream and synthesize new Hb molecules. Proerythroblasts then differentiate into various stages of cells called erythroblasts, which actively synthesize hemoglobin. Erythroblasts are named according to total size, amount of hemoglobin present, and size and appearance of the nucleus. Events in the life cycle of RBCs Events Occurring in Macrophages Macrophages in liver, spleen, and bone marrow Fe2+ Fe2+ transported in circulation RBC formation by transferrin Heme Amino acids Average life span of RBC is 120 days 90% Biliverdin Bilirubin 10% Bilirubin bound to albumin in bloodstream Cells destines to become RBCs first differentiate into proerythroblasts. Old and damaged RBCs In the bloodstream, the rupture of RBCs is called hemolysis. Hemoglobin that is not phagocytized breaks down, and the alpha and beta chains are eliminated in urine. When abnormally large numbers of RBCs break down in the bloodstream, urine may turn red or brown. This condition is called hemoglobobinuria. Ejection of nucleus After roughly four days of differentiation, the erythroblast, now called a normoblast, sheds its nucleus and becomes a reticulocyte (re-TIK-ū-lō-sīt), which contains 80 percent of the Hb of mature RBC. After two days in the bone marrow, reticulocytes enter the bloodstream. After 24 hours in circulation, the reticulocytes complete their maturation and become indistinguishable from other mature RBCs. New RBCs released into circulation Liver Bilirubin Events Occurring in the Kidney Absorbed into the circulation Excreted in bile Hb Events Occurring in the Liver Bilirubin Urobilins Urobilins, sterconilins Events Occurring in the Large Intestine Eliminated in feces Eliminated in urine Figure17.3 Module 17.3 Review a. Define hemolysis. b. Identify the products formed during the breakdown of heme. c. In what way would a liver disease affect the level of bilirubin in the blood? Module 17.4: Blood types • Blood types • Determined by presence or absence of cell surface markers (antigens) • • • • Are genetically determined glycoproteins or glycolipids Can trigger a protective defense mechanism (immune response) Identify blood cells as “self” or “foreign” to immune system More than 50 blood cell surface antigens exist • Three particularly important • A, B, Rh (or D) Module 17.4: Blood types • Four blood types (AB antigens) 1. Type A (A surface antigens) • 2. Anti-B antibodies in plasma Type B (B surface antigens) • 3. Anti-A antibodies in plasma Type AB (Both A and B surface antigens) • 4. No anti-A or anti-B antibodies in plasma Type O (no A or B surface antigens) • Both anti-A and anti-B antibodies in plasma The characteristics of blood for each of the four blood types Type A Type B Type A blood has RBCs with surface antigen A only. Type B blood has RBCs with surface antigen B only. Surface antigen A If you have Type A blood, your plasma contains anti-B antibodies, which will attack Type B surface antigens. Type AB Type O Type AB blood has RBCs with both A and B surface antigens. Type O blood has RBCs lacking both A and B surface antigens. If you have Type AB blood, your plasma has neither anti-A nor anti-B antibodies. If you have Type O blood, your plasma contains both anti-A and anti-B antibodies. Surface antigen B If you have Type B blood, your plasma contains anti-A antibodies. Figure17.4 1 Module 17.4: Blood types • Rh surface antigens • • • Separate antigen from A or B Presence or absence on RBC determines positive or negative blood type respectively Examples: AB+, O– Figure17.4 3 Module 17.4 Review a. What is the function of surface antigens on RBCs? b. Which blood type(s) can be safely transfused into a person with Type O blood? CLINICAL MODULE 17.5: Newborn hemolytic disease • Newborn hemolytic disease • Genetically determined antigens mean that a child can have a blood type different from either parent During pregnancy, the placenta restricts direct transport between maternal and infant blood • • • Anti-A and anti-B antibodies are too large to cross Anti-Rh antibodies can cross • Can lead to mother’s antibodies attacking fetal RBCs CLINICAL MODULE 17.5: Newborn hemolytic disease • First pregnancy with Rh– mother and Rh+ infant • During pregnancy, few issues occur because no anti-Rh antibodies exist in maternal circulation During birth, hemorraging may expose maternal blood to fetal Rh+ cells • • Leads to sensitization or activation of mother’s immune system to produce anti-Rh antibodies Rh– mother First Pregnancy of an Rh– Mother with an Rh+ infant Rh+ fetus The most common form of hemolytic disease of the newborn develops after an Rh– women has carried an Rh+ fetus. During First Pregnancy Problems seldom develop during a Maternal blood supply first pregnancy, because very few fetal and tissue cells enter the maternal circulation then, and thus the mother’s immune system is not stimulated to produce anti-Rh antibodies. Placenta Fetal blood supply and tissue Exposure to fetal red blood cell antigens generally occurs during delivery, when bleeding takes place at the placenta and uterus. Such mixing of fetal and maternal blood can stimulate the mother’s immune system to produce anti-Rh antibodies, leading to sensitization. Hemorrhaging at Delivery Maternal blood supply and tissue Fetal blood supply and tissue Roughly 20 percent of Rh– mothers who carried Rh+ children become sensitized within 6 months of delivery. Because the anti-Rh antibodies are not produced in significant amounts until after delivery, a woman’s first infant is not affected. Rh antigen on fetal red blood cells Maternal Antibody Production Maternal blood supply and tissue Maternal antibodies to Rh antigen Figure17.5 CLINICAL MODULE 17.5: Newborn hemolytic disease • Second pregnancy with Rh– mother and Rh+ infant • Subsequent pregnancy with Rh+ infant can allow maternal anti-Rh antibodies to cross placental barrier • Attack fetal RBCs and cause hemolysis and anemia • • = Erythroblastosis fetalis Full transfusion of fetal blood may be necessary to remove maternal anti-Rh antibodies Prevention • • RhoGAM antibodies can be administered to maternal circulation at 26–28 weeks and before/after birth • • Destroys any fetal RBCs that cross placenta Prevents maternal sensitization Rh– mother Second Pregnancy of an Rh– Mother with an Rh+ Infant Rh+ fetus If a subsequent pregnancy involves an Rh+ fetus, maternal anti-Rh antibodies produced after the first delivery cross the placenta and enter the fetal bloodstream. These antibodies destroy fetal RBCs, producing a dangerous anemia. The fetal demand for blood cells increases, and they begin leaving the bone marrow and entering the bloodstream before completing their development. Because these immature During Second Pregnancy RBCs are erythroblasts, HDN is also known as erythroblastosis fetalis. Fortunately, the Maternal blood supply mother’s anti-Rh antibody production can and tissue be prevented if such antibodies (available under the name RhoGAM) are administered to the mother in weeks 26–28 of pregnancy and during and after delivery. These antibodies destroy any fetal RBCs that cross the placenta before they can stimulate Fetal blood supply a maternal immune response. Because and tissue maternal sensitization does not occur, no anti-Rh antibodies are produced. Hemolysis of fetal RBCs Maternal anti-Rh antibodies Figure17.5 CLINICAL MODULE 17.5 Review a. Define hemolytic disease of the newborn (HDN). b. Why is RhoGAM administered to Rh– mothers? Module 17.6: White blood cells • White blood cells (leukocytes) • Spend only a short time in circulation • Mostly located in loose and dense connective tissues where infections often occur • Can migrate out of bloodstream • • • • • Contact and adhere to vessel walls near infection site Squeeze between adjacent endothelial cells = Emigration Are attracted to chemicals from pathogens, damaged tissues, or other WBCs = Positive chemotaxis Module 17.6: White blood cells • White blood cell types 1. Granular leukocytes (have cytoplasmic granules) • • • Neutrophil Eosinophil Basophil 2. Agranular leukocytes (lacking cytoplasmic granules) • • Monocyte Lymphocyte • Changing populations of different WBC types associated with different conditions can be seen in a differential WBC count Module 17.6: White blood cells • Granular leukocytes • Neutrophils • Multilobed nucleus • Phagocytic cells that engulf pathogens and debris • Eosinophils • Granules generally stain bright red • Phagocytic cells that engulf antibody-labeled materials • Increase abundance with allergies and parasitic infections • Basophils • Granules generally stain blue • Release histamine and other chemicals promoting inflammation The structure and function of white blood cells (leukocytes) GRANULAR LEUKOCYTES Neutrophil Eosinophil Basophil WBCs can be divided into two classes Shared Properties of WBCs • WBCs circulate for only a short portion of their life span, using the bloodstream primarily to travel between organs and to rapidly reach areas of infection or injury. White blood cells spend most of their time migrating through loose and dense connective tissues throughout the body. AGRANULAR LEUKOCYTES Monocyte Lymphocyte • All WBCs can migrate out of the bloodstream. When circulating white blood cells in the bloodstream become activated, they contact and adhere to the vessel walls and squeeze between adjacent endothelial cells to enter the surrounding tissue. This process is called emigration, or diapedesis (dia, through; pedesis, a leaping). • All WBCs are attracted to specific chemical stimuli. This characteristic, called postive chemotaxis (kē-mō-TAK-sis), guides WBCs to invading pathogens, damaged tissues, and other active WBCs. • Neutrophils, eosinophils, and monocytes are capable of phagocytosis. These phagocytes can engulf pathogens, cell debris, or other materials. Macrophages are monocytes that have moved out of the bloodstream and have become actively phagocytic. Figure17.6 Module 17.6: White blood cells • Agranular leukocytes • Monocytes • Large cells with bean-shaped nucleus • Enter tissues and become macrophages (phagocytes) • Lymphocytes • Slightly larger than RBC with large round nucleus • Provide defense against specific pathogens or toxins Module 17.6 Review a. Identify the five types of white blood cells. b. How do basophils respond during inflammation? Module 17.7: Formed element production • • Formed elements • Appropriate term since platelets are cell fragments Platelets • • • Structure: flattened discs that appear round when viewed from top but spindle-shaped in blood smear Function: clump together and stick to damaged vessel walls where they release clotting chemicals Immediate precursor cell is megakaryocyte (mega-, big + karyon, nucleus + -cyte, cell) Module 17.8: Hemostasis • Hemostasis (haima, blood + stasis, halt) • Stops blood loss from damaged blood vessel walls • Establishes framework for tissue repairs Fig. 18.1 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Monocyte Small lymphocyte Neutrophil Platelets Eosinophil Small lymphocyte Erythrocyte Young (band) neutrophil Neutrophil Monocyte Large lymphocyte Neutrophil Basophil Section 2: Functional Anatomy of Blood Vessels • • Blood vessels conduct blood between heart and peripheral tissues Two circuits 1. 2. • Pulmonary circuit (to and from lungs) Systemic circuit (to and from rest of body) Each circuit begins and ends with heart • Occur in sequence Section 2: Functional Anatomy of Blood Vessels • Specific vessels • • • Arteries (transport blood away from heart) Veins (transport blood to the heart) Capillaries (exchange substances between blood and tissues) • Interconnect smallest arteries and smallest veins Section 2: Functional Anatomy of Blood Vessels • General circulation pathway through circuits 1. Right atrium (entry chamber) from systemic circuit to right ventricle, to pulmonary circuit Pulmonary circuit 2. • 3. Pulmonary arteries to pulmonary capillaries to pulmonary veins Left atrium from pulmonary circuit to left ventricle, to systemic circuit Systemic circuit 4. • Systemic arteries to systemic capillaries to systemic veins Figure17 Section2 Module 17.10: Arteries and veins • Both arteries and veins have three layers 1. Tunica intima (tunica interna) • • Innermost layer Endothelial cells with connective tissue with elastic fibers • 2. In arteries, outer margin has layer of elastic fibers (internal elastic membrane) Tunica media • • Middle layer Contains concentric sheets of smooth muscle • • Capable of vasoconstriction or vasodilation Collagen fibers connect tunica media to other layers Module 17.10: Arteries and veins • Both arteries and veins have three layers (continued) 3. Tunica externa • • • • Outermost layer Connective tissue sheath with collagen and elastic fibers Generally thicker in veins Anchor vessel to surrounding tissues A photomicrograph of an artery and an adjacent vein Artery Vein LM x 60 Figure17.10 1 The structure of the wall of an artery Artery Tunica intima Smooth muscle Internal elastic membrane External elastic membrane Tunica media Endothelium Elastic fiber Tunica externa Figure17.10 1 The structure of the wall of a vein Vein Endothelium Smooth muscle Tunica intima Tunica media Tunica externa Figure17.10 1 Module 17.10: Arteries and veins • Five general blood vessel classes 1. Arteries • • 2. Elastic arteries (large vessels close to the heart that stretch and recoil when heart beats) Muscular arteries (medium-sized arteries, distribute blood to skeletal muscles and internal organs) Arterioles • 3. Poorly defined tunica externa and tunica media only 1–2 smooth muscle cells thick Capillaries • Thin, exchange vessels Module 17.10: Arteries and veins • Five general blood vessel classes (continued) 4. Venules (small veins lacking tunica media, collect blood from capillaries) Veins 5. • • Medium-sized veins (tunica media is thin but tunica externa is thick with longitudinal collagen and elastic fibers) Large veins (superior and inferior venae cavae and tributaries having thin tunica media) The five general classes of blood vessels: arteries, arterioles, capillaries, venules, and veins Large Veins Elastic Arteries Include the superior and inferior venae cavae and their tributaries; contain all three vessel wall layers; have a slender tunica media composed of a mixture of elastic and collagen fibers Large vessels that transport blood away from the heart; include the pulmonary trunk and the aorta and its major branches; are resilent, elastic vessels capable of stretching and recoiling as the heart beats and arterial pressures change Tunica externa Tunica media Tunica intima Internal elastic layer Tunica intima Tunica media Tunica externa Medium-sized Veins Muscular Arteries Range from 2 to 9 mm in internal diameter; the tunica media is thin and contains relatively few smooth muscle cells; the thickest layer is the tunica externa, which contains longitudinal bundles of elastic and collagen fibers Medium-sized arteries that distribute blood to the body’s skeletal muscles and internal organs Tunica externa Tunica media Tunica intima Tunica externa Tunica media Tunica intima Venules Arterioles Collect blood from capillary beds and are the smallest venous vessels; those smaller than 50 μm lack a tunica media and resemble expanded capillaries Have a poorly defined tunica externa, and the tunica media consists of only one or two layers of smooth muscle cells Smooth muscle cells Endothelium Tunica externa Endothelium Capillaries Pores Endothelial cells Basal lamina The only blood vessels whose walls permit exchange between the blood and the surrounding interstitial fluids due to thin walls and short diffusion distances Endothelial cells Basal lamina Figure17.10 2 Module 17.10 Review a. List the five general classes of blood vessels. b. Describe a capillary. c. A cross section of tissue shows several small, thin-walled vessels with very little smooth muscle tissue in the tunica media. Which type of vessels are these? Module 17.11: Capillaries • Typical capillary consists of tube of endothelial cells with delicate basal lamina • • • Neither tunica intima nor externa are present Average diameter = 8 µm • About the same as an RBC Two major categories 1. 2. Continuous capillaries Fenestrated capillaries Module 17.11: Capillaries • Continuous capillaries • • Endothelium is a complete lining Located throughout body in all tissues except epithelium and cartilage Permit diffusion of water, small solutes, and lipid-soluble materials • • • • Prevent loss of blood cells and plasma proteins Some selective vesicular transport Some capillaries have endothelial tight junctions • Restricted and regulated permeability Module 17.11: Capillaries • Fenestrated capillaries • • • Contain windows or pores penetrating endothelium Permit rapid exchange of water and larger solutes Examples: capillaries in brain and endocrine organs, absorptive areas of GI tract, kidney filtration sites The two major types of capillaries: continuous capillaries and fenestrated capillaries Basal lamina Endothelial cell Nucleus A continuous capillary A fenestrated capillary Fenestrations, or pores Vesicles containing materials transported across the endothelial cell Basal lamina Boundary between endothelial cells Boundary between endothelial cells Basal lamina Figure17.11 1 – 2 Module 17.11: Capillaries • Sinusoids • • • • • Resemble fenestrated capillaries that are flattened and irregularly shaped Commonly have gaps between endothelial cells Basal lamina is thin or absent Permit more water and solute (plasma proteins) exchange Occur in liver, bone marrow, spleen, and many endocrine organs A sinusoid Gap between adjacent cells Figure17.11 3 Module 17.11: Capillaries • Capillary bed • • • Network of capillaries with several connections between arterioles and venules Can have collateral arteries (functionally redundant) fusing to one arteriole (forming an arterial anastomosis) leading to capillary bed Can be bypassed by arteriovenous anastomosis that directly connects arteriole to venule Module 17.11: Capillaries • Capillary bed (continued) • Thoroughfare channels (direct passages through capillary bed) • • Begin with metarteriole segment that can constrict or dilate to control flow Has multiple capillaries connecting to venules • Have bands of smooth muscle (precapillary sphincters) to control flow into capillary bed • Vasomotion (cycling contraction and relaxing changing capillary bed flow) A capillary bed Collateral arteries Vein Venule Arteriole Metarteriole Smooth muscle cells Thoroughfare channel Capillaries Precapillary sphincter Small venules Arteriovenous anastomosis Precapillary sphincters KEY Continuous blood flow Variable blood flow Figure17.11 4 Module 17.11 Review a. Identify the two types of capillaries. b. At what sites in the body are fenestrated capillaries located? c. Why do capillaries permit the diffusion of materials, whereas arteries and veins do not? Module 17.12: Venous functional anatomy • Venous functional anatomy and pressure • Blood pressure in venules and medium veins is <10% of that in ascending aorta (largest artery) These vessels contain valves (folds of tunica intima) that ensure one-way flow of blood toward heart • • Malfunctioning valves can lead to varicose veins (enlarged superifical thigh and leg veins) or distortion of adjacent tissues (hemorrhoids) Figure17.12 1 Module 17.12: Venous functional anatomy • Increasing venous blood flow • • Skeletal muscle contractions squeezing veins with valves Sympathetically controlled constriction of veins (venoconstriction) • Venoconstriction can maintain arterial blood volume despite hemorrhaging Figure17.12 2 • Total blood volume distribution • Unevenly distributed between arteries, veins, and capillaries • Systemic venous system contains nearly 2/3 of total blood volume (~3.5 L) • Of that , ~1 L is in venous networks of liver, bone marrow, and skin venous The distribution of blood volume within the body Systemic venous system Pulmonary circuit Heart Systemic arterial system Systemic capillaries Module 17.12 Review a. Define varicose veins. b. Why are valves located in veins, but not in arteries? c. How is blood pressure maintained in veins to counter the force of gravity? Module 17.13: Pulmonary circuit • Arteries of pulmonary circuit differ from those in systemic circuit • Pulmonary arteries carry deoxygenated blood Right ventricle pulmonary trunk (large artery) pulmonary arteries pulmonary arterioles pulmonary capillaries (surrounded by alveoli, where gas exchange occurs) pulmonary venules pulmonary veins left atrium Fig. 19.1 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. CO2 O2 Pulmonary circuit O2-poor, CO2-rich blood O2-rich, CO2-poor blood Systemic circuit CO2 O2 The path of blood flow through the pulmonary circuit Aortic arch Ascending aorta Pulmonary trunk Superior vena cava Left lung Left pulmonary arteries Right lung Right pulmonary arteries Left pulmonary veins Right pulmonary veins Alveolus Capillary Inferior vena cava Descending aorta Figure17.13 3 Module 17.13: Pulmonary circuit • Major patterns of blood vessel organization 1. Peripheral arteries and veins are generally identical between left and right sides except near heart Vessels change names as they branch or move into new areas Tissues and organs are usually served by many arteries and veins 2. 3. • Anastomoses reduce impact of potential blockages (occlusions) Module 17.13 Review a. Identify the two circulatory circuits of the cardiovascular system. b. Briefly describe the three major patterns of blood vessel organization. c. Trace a drop of blood through the lungs, beginning at the right ventricle and ending at the left atrium. Module 17.14: Systemic vessels • Systemic vessels • Arterial system • • Originates from aorta (largest elastic vessel exiting left ventricle) Venous system • All drain into: • Superior vena cava (upper limbs, head, and neck) • Inferior vena cava (trunk and lower limbs) An overview of the systemic arterial system Vertebral Common carotid Subclavian Brachiocephalic trunk Axillary Aortic arch Ascending aorta Descending aorta Diaphragm Brachial Celiac trunk Renal Gonadal Lumbar Common iliac Radial Internal iliac Ulnar Digital arteries External iliac Palmar arches Deep femoral Femoral Popliteal Posterior tibial Anterior tibial Fibular Dorsalis pedis Plantar arch Figure17.14 1 An overview of the systemic venous system Vertebral External jugular Internal jugular Subclavian Brachiocephalic Axillary Superior vena cava Brachial Cephalic Diaphragm Basilic Inferior vena cava Renal Gonadal Lumbar Radial Median antebrachial Ulnar Common iliac Internal iliac External iliac Palmar venous arches Digital veins Deep femoral Femoral Great saphenous Popliteal Small saphenous Fibular Plantar venous arch Dorsal venous arch Posterior tibial Anterior tibial KEY Superficial veins Deep veins Figure17.14 2 Module 17.14: Systemic vessels • Systemic vessels • • Arteries and veins are usually similar on both sides of body One significant difference between arteries and veins is distribution in the neck and limbs • • Arteries: deep in skin, protected by bones and soft tissues Veins: generally two sets, one deep and one superficial • Important in controlling body temperature • Venous blood flows superficially in hot weather to radiate heat • Venous blood flows deep in cold weather to conserve heat Module 17.14 Review a. Name the two large veins that collect blood from the systemic circuit. b. Identify the largest artery in the body. c. Besides containing valves, cite another major difference between the arterial and venous systems. Module 17.15: Upper limb vessels • Upper limb vessels • Arteries • Branches of aortic arch • Brachiocephalic trunk • Right subclavian (right arm) • Right common carotid artery (right side head & neck) • • Left common carotid artery (left side head & neck) Left subclavian artery (left arm) Module 17.15: Upper limb vessels • Arteries (continued) • Right subclavian artery branches • • • Internal thoracic artery (pericardium, anterior chest wall) Vertebral artery (brain, spinal cord) Arteries of the arm • • Axillary artery (through axilla) Brachial artery (upper limb) Module 17.15: Upper limb vessels • Arteries (continued) • Arteries of the forearm • • • • Radial artery (follows radius) Ulnar artery (follows ulna) Palmar arches (hand) Digital arteries (thumb and fingers) The branches of the aortic arch and the arteries they give rise to Branches of the Aortic Arch Start Brachiocephalic trunk Left common carotid artery Left subclavian artery The Right Subclavian Artery Vertebral Internal thoracic Major branches of the subclavian artery Aortic arch Axillary Ascending aorta Deep brachial Arteries of the Arm Heart Brachial Ulnar collateral arteries Arteries of the Forearm Descending aorta Radial Ulnar Deep palmar arch Superficial palmar arch Digital arteries Figure17.15 Veins of the Neck The veins that drain into the superior vena cava External jugular vein Internal jugular vein Vertebral vein Brachiocephalic vein The Right Subclavian Vein Veins of the Arm Axillary vein Cephalic vein Veins of the Forearm Median cubital vein Superior vena cava Brachial Basilic Superior vena cava Median antebrachial vein KEY Cephalic Superficial veins Deep veins Radial Basilic Ulnar Digital veins Deep palmar arch Start Superficial palmar arch Figure17.15 Module 17.15: Upper limb vessels • Veins • • Digital veins (empty from thumb and fingers) Veins of the forearm • • • • • Superficial palmar arch (hand) Median antebrachial vein (anterior forearm) Cephalic vein Basilic vein Median cubital vein (interconnects cephalic and basilic veins) • Venous samples usually collected here Module 17.15: Upper limb vessels • Veins (continued) • Veins of the arm • • • • Cephalic vein (lateral side of arm) Basilic vein (median side of arm) Brachial vein (median area of arm) Right subclavian vein • Merging of axillary vein and cephalic vein Module 17.15: Upper limb vessels • Veins (continued) • Veins of the neck • • • • External jugular vein (drains superficial head & neck) Internal jugular vein (drains deep head & neck) Vertebral vein (cervical spinal cord and posterior skull) Veins draining into superior vena cava (SVC) • • Internal thoracic vein (intercostal veins) Brachiocephalic vein (jugular, axillary, vertebral, and internal thoracic veins) Module 17.15 Review a. Name the two arteries formed by the division of the brachiocephalic trunk. b. A blockage of which branch from the aortic arch would interfere with blood flow to the left arm? c. Whenever Thor gets angry, a large vein bulges in the lateral region of his neck. Which vein is this? Module 17.16: Head and neck vessels • Head and neck vessels • Arteries • Common carotid artery (head and neck) • Palpated alongside trachea (windpipe) • Contains carotid sinus (with baroreceptors monitoring blood pressure) • Branches of common carotid artery • External carotid artery (neck, esophagus, pharynx, larynx, lower jaw, cranium, and face on that side) • Internal carotid artery (brain and eyes) • Vertebral artery (enters cranium and fuses with basilar artery along ventral medulla oblongata) Areas supplies by the external carotid, internal carotid, and vertebral arteries Carotid canal Basilar Superficial temporal Maxillary Occipital Branches of the External Carotid Facial Internal carotid artery Lingual External carotid Vertebral artery Carotid sinus Common carotid artery Axillary Subclavian Brachiocephalic trunk Figure17.16 1 Module 17.16: Head and neck vessels • Veins • • • External jugular vein (cranium, face, lower jaw, and neck on that side) Internal jugular vein (various cranial venous sinuses) Vertebral vein (cervical spinal cord and posterior skull) Areas drained by the external and internal jugular veins Dural sinuses draining the brain Temporal Maxillary Jugular foramen Facial Branches of the External Jugular Occipital External jugular Vertebral vein Internal jugular vein Clavicle Right brachiocephalic Left brachiocephalic Axillary Right subclavian Superior vena cava Figure17.16 2 Module 17.16 Review a. Name the arterial structure that contains baroreceptors. b. Identify branches of the external carotid artery. c. Identify the veins that combine to form the brachiocephalic vein. Module 17.18: Vessels of the trunk • Vessels of the trunk • Arteries • Somatic branches of thoracic aorta • Intercostal arteries (chest muscles and vertebral column) • Superior phrenic artery (superior diaphragm) • Visceral branches of thoracic aorta • • • • Bronchial arteries (lung tissues not involved in gas exchange) Esophageal arteries (esophagus) Mediastinal arteries (tissues of mediastinum) Pericardial arteries (pericardium) Module 17.18: Vessels of the trunk • Arteries (continued) • Major paired abdominal aorta branches • • • • • Inferior phrenic arteries (inferior diaphragm and esophagus) Adrenal arteries (adrenal glands) Renal arteries (kidneys) Gonadal arteries (gonads) Lumbar arteries (vertebrae, spinal cord, abdominal wall) Module 17.18: Vessels of the trunk • Arteries (continued) • Major unpaired branches of abdominal aorta • Celiac trunk (three branches) 1. 2. 3. • • Left gastric artery (stomach and inferior esophagus) Splenic artery (spleen and stomach arteries) Common hepatic artery (arteries to liver, stomach, gallbladder, and proximal small intestine) Superior mesenteric artery (pancreas, duodenum, most of large intestine) Inferior mesenteric artery (colon and rectum) The branches of the thoracic aorta and the abdominal aorta Aortic arch Internal thoracic Thoracic aorta Somatic Branches of the Thoracic Aorta Visceral Branches of the Thoracic Aorta Bronchial arteries Esophageal arteries Intercostal arteries Mediastinal artery Superior phrenic artery Pericardial artery Diaphragm Inferior phrenic Adrenal Renal Gonadal Lumbar Common iliac Celiac trunk Left gastric Splenic Common hepatic Branches of the celiac trunk Superior mesenteric Abdomial aorta Inferior mesenteric Figure17.18 1 Module 17.18: Vessels of the trunk • Veins • Azygos and hemiazygos veins (most of thorax) 1. 2. 3. 4. Intercostal veins (chest muscles) Esophageal veins (inferior esophagus) Bronchial veins (passageways of lungs) Mediastinal veins (mediastinal structures) Module 17.18: Vessels of the • Veins (continued) trunk • Major tributaries of inferior vena cava • • • • • • Lumbar veins (lumbar portion of abdomen) Gonadal veins (gonads) Hepatic veins (liver) Renal veins (kidneys) Adrenal veins (adrenal glands) Phrenic veins (diaphragm) The major tributaries of the superior and inferior venae cavae Brachiocephalic The Azygos and Hemiazygos Veins Superior vena cava Azygos vein Hemiazygos vein Internal thoracic Tributaries: Esophageal, bronchial, and mediastinal veins Intercostal veins Inferior vena cava Hepatics Phrenic Adrenal Renal Gonadal Lumbar Common iliac Major Tributaries of the Inferior Vena Cava • Lumbar veins drain the lumbar portion of the abdomen, including the spinal cord and muscles of the body wall. • Gonadal (ovarian or testicular) veins drain the ovaries of testes. The right gonadal vein empties into the inferior vena cava; the left gonadal vein generally drains into the left renal vein. • Hepatic veins drain the sinusoids of the liver. • Renal veins, the largest tributaries of the inferior vena cava, collect blood from the kidneys. • Adrenal veins drain the adrenal glands. In most individuals, only the right adrenal vein drains into the inferior vena cava; the left adrenal vein drains into the left renal vein. • Phrenic veins drain the diaphragm. Only the right phrenic vein drains into the inferior vena cava; the left drains into the left renal vein. Figure17.18 2 Module 17.18 Review a. Which vessel collects most of the venous blood inferior to the diaphragm? b. Identify the major tributaries of the inferior vena cava. c. Grace is in an automobile accident, and her celiac trunk is ruptured. Which organs will be affected most directly by this injury? Module 17.19: Vessels of the viscera • Vessels of the viscera • Arteries • Branches of common hepatic artery • • • • • • Hepatic artery proper (liver) Cystic (gallbladder) Gastroduodenal (stomach and duodenum) Right gastric (stomach) Right gastroepiploic (stomach and duodenum) Superior pancreaticoduodenal (duodenum) Module 17.19: Vessels of the viscera • Arteries (continued) • Superior mesenteric artery • • • • • Inferior pancreaticoduodenal (pancreas and duodenum) Right colic (large intestine) Ileocolic (large intestine) Middle colic (large intestine) Intestinal arteries (small intestine) Module 17.19: Vessels of the viscera • Arteries (continued) • Inferior mesenteric artery • • • • Left colic (colon) Sigmoid (colon) Rectal (colon) Branches of the splenic artery • • Left gastroepiploic (stomach) Pancreatic (pancreas) The locations of the celiac trunk, the superior and inferior mesenteric arteries, and their branches The Celiac Trunk Common hepatic artery Left gastric artery Splenic artery The celiac trunk Branches of the Common Hepatic Artery Hepatic artery proper (liver) Cystic (gallbladder) Liver Branches of the Splenic Artery Gastroduodenal (stomach and duodenum) Right gastric (stomach) Stomach Pancreatic (pancreas) Right gastroepiploic (stomach and duodenum) Superior pancreaticoduodenal (duodenum) Ascending colon Left gastroepiploic (stomach) Spleen Panceas Inferior Mesenteric Artery Superior Mesenteric Artery Left colic (colon) Sigmoid (colon) Inferior pancreaticoduodenal (pancreas and duodenum) Right colic (large intestine) Ileocolic (large intestine) Middle colic (cut) (large intestine) Rectal (rectum) Small intestine Sigmoid colon Rectum Intestinal arteries (small intestine) Figure17.19 1 Module 17.19: Vessels of the viscera • Veins • Hepatic portal vein tributaries • Superior mesenteric vein and tributaries • • • • • Pancreaticoduodenal Middle colic (transverse colon) Right colic (ascending colon) Ileocolic (Ileum and ascending colon) Intestinal (small intestine) Module 17.19: Vessels of the viscera • Veins (continued) • Hepatic portal vein tributaries (continued) • Splenic vein and tributaries • • • • Left gastroepiploic (stomach) Right gastroepiploic (stomach) Pancreatic Inferior mesenteric vein and tributaries • • • Left colic (descending colon) Sigmoid (sigmoid colon) Superior rectal (rectum) The veins (and their tributaries) that form the hepatic portal vein Inferior vena cava Left gastric Right gastric Hepatic Liver Splenic Vein and Its Tributaries Stomach Cystic Hepatic portal Spleen Superior Mesenteric Vein and Its Tributaries Left gastroepiploic (stomach) Right gastroepiploic (stomach) Pancreatic Pancreas Pancreaticoduodenal Middle colic (from transverse colon) Right colic (ascending colon) Ileocolic (ileum and ascending colon) Intestinal (small intestine) Descending colon Inferior Mesenteric Vein and Its Tributaries Left colic (descending colon) Sigmoid (sigmoid colon) Superior rectal (rectum) Tributaries of the Hepatic Portal Vein • The inferior mesenteric vein collects blood from capillaries along the inferior portion of the large intestine. It drains the left colic vein and the superior rectal veins, which collect venous blood from the descending colon, sigmoid colon, and rectum. • The splenic vein is formed by the union of the inferior mesenteric vein and veins from the spleen, the lateral border of the stomach (left gastroepiploic vein), and the pancreas (pancreatic veins). • The superior mesenteric vein collects blood from veins draining the stomach (right gastroepiploic vein), the small intestine (intestinal and pancreaticoduodenal veins), and two-thirds of the large intestine (ileocolic, right colic, and middle colic veins). Figure17.19 2 Module 17.19 Review a. List the unpaired branches of the abdominal aorta that supply blood to the visceral organs. b. Identify the three veins that merge to form the hepatic portal vein. c. Identify two veins that carry blood away from the stomach. Module 17.20: Lower limb vessels • Lower limb vessels • Arteries • Common iliac artery • • • • • Internal iliac artery (bladder, pelvic walls, external genitalia, medial side of thigh, in females, uterus and vagina) Lateral sacral artery Internal pudendal artery Obturator artery Superior gluteal artery Module 17.20: Lower limb vessels • Arteries (continued) • Common iliac artery (continued) • External iliac artery • Femoral artery • • • • • Deep femoral artery Femoral circumflex arteries (ventral and lateral skin and deep muscles of thigh) Popliteal artery (posterior knee) Posterior and anterior tibial arteries (leg) Fibular artery (lateral leg) Module 17.20: Lower limb vessels • Arteries (continued) • Arteries of the foot • • • • • Dorsalis pedis Dorsal arch Plantar arch Medial plantar Lateral plantar The arteries that supply the pelvis and lower limb Anterior View Internal Iliac and Its Branches Common iliac Posterior View Internal iliac External iliac Femoral Deep femoral Right external iliac Lateral sacral Internal pudendal Obturator Femoral circumflex Deep femoral Femoral circumflex Superior gluteal Femoral Descending genicular artery Popliteal Popliteal Anterior tibial Posterior tibial Anterior tibial Posterior tibial Fibular Arteries of the Foot Fibular (peroneal) Dorsalis pedis Medial plantar Lateral plantar Dorsal arch Plantar arch Figure17.20 1 Module 17.20: Lower limb vessels • Veins • • • External iliac veins (lower limbs, pelvis, and lower abdomen) Internal iliac veins (pelvic organs) External and internal iliac fuse to form common iliac veins The veins that drain the pelvis and lower limb Anterior View Common iliac Posterior View External iliac Internal iliac Gluteal Internal pudendal Lateral sacral Obturator Femoral Femoral circumflex Deep femoral Convergence of the great saphenous, the deep femoral, and the femoral circumflex veins Femoral Great saphenous Femoral Popliteal Small saphenous Anterior tibial Posterior tibial Fibular Dorsal venous arch Plantar venous arch Digital Figure17.20 2 Module 17.20 Review a. Name the first two divisions of the common iliac artery. b. The plantar venous arch carries blood to which three veins? c. A blood clot that blocks the popliteal vein would interfere with blood flow in which other veins? CLINICAL MODULE 17.21: Fetal circulation and defects • Unique fetal circulation structures • • • Umbilical arteries (internal iliac arteries to placenta) Umbilical vein (placenta to ductus venosus) Ductus venosus (drains liver and umbilical vein into inferior vena cava) Ductus arteriosus (pulmonary trunk to aorta) • • • Sends blood from right ventricle to systemic circuit Foramen ovale (right to left atrium) • Has one-way valve to prevent backflow The path of blood flow in a full-term fetus before birth Foramen ovale Ductus arteriosus Aorta Placenta Pulmonary trunk Liver Umbilical vein Inferior vena cava Ductus venosus Umbilical cord Umbilical arteries Figure17.21 1 CLINICAL MODULE 17.21: Fetal circulation and defects • At birth, fetal circulation changes due to activated pulmonary circulation • Resulting pressure closes foramen ovale • • Fossa ovalis (shallow depression, adult remnant) Rising oxygen levels cause ductus arteriosus to constrict and close • Ligamentum arteriosum (fibrous adult remnant) The flow of blood through the heart upon the closing of the ductus arteriosus and foramen ovale at birth Ductus arteriosus (closed) Pulmonary trunk Left atrium Foramen ovale (closed) Right atrium Left ventricle Right ventricle Inferior vena cava Figure17.21 2 CLINICAL MODULE 17.21: Fetal circulation and defects • Congenital cardiac defects • Ventricular septal defects • • Openings in interventricular septum Patent foramen ovale • • • Passageway remains open Left ventricle must work harder to provide adequate systemic flow Patent ductus arteriosus • • Passageway remains open Blood is not adequately oxygenated and skin bluish CLINICAL MODULE 17.21 Review a. Describe the pattern of fetal blood flow to and from the placenta. b. Identify the six structures that are necessary in the fetal circulation but cease to function at birth, and describe what becomes of these structures. Module 18.4: Coronary circulation • Coronary circulation • • • Provides cardiac muscle cells with reliable supplies of oxygen and nutrients During maximum exertion, myocardial blood flow may increase to 9× resting levels Blood flow is continuous but not steady • With left ventricular relaxation, aorta walls recoil (elastic rebound), which pushes blood into coronary arteries Module 18.4: Coronary circulation • Coronary arteries • Right coronary artery (right atrium, portions of both ventricles and conduction system of heart) • • • Marginal arteries (right ventricle surface) Posterior interventricular artery (interventricular septum and adjacent ventricular portions) Left coronary artery (left ventricle, left atrium, and interventricular septum) • • Circumflex artery (from left coronary artery, follows coronary sulcus to meet right coronary artery branches) Anterior interventricular artery (interventricular sulcus) The locations of the arterial supply to the heart Pulmonary trunk Aortic arch An anterior view of the coronary arteries Left Coronary Artery Left atrium Left coronary artery Circumflex artery Right atrium Right Coronary Artery Anterior interventricular artery Right ventricle Right coronary artery in the coronary sulcus Left ventricle Marginal arteries Anterior view Arterial anastomoses between the anterior and posterior interventricular arteries The branches of the coronary arteries on the posterior surface of the heart Circumflex artery Left atrium Marginal artery Right atrium Left ventricle Posterior interventricular artery Right ventricle Posterior view Right coronary artery Figure18.4 1 – 2 Module 18.4: Coronary circulation • Coronary veins • • Great cardiac vein (drains area supplied by anterior interventricular artery, empties into coronary sinus on posterior) Anterior cardiac veins (drains anterior surface of right ventricle, empties into right atrium) The major collecting vessels on the anterior surface of the heart Aortic arch Left atrium Right atrium Anterior cardiac veins Great cardiac vein Right ventricle Left ventricle Anterior view Figure18.4 3 Module 18.4: Coronary circulation • Coronary veins (continued) • • • • Coronary sinus (expanded vein, empties into right atrium) Posterior cardiac vein (drains area supplied by circumflex artery) Small cardiac vein (drains posterior right atrium and ventricle, empties into coronary sinus) Middle cardiac vein (drains area supplied by posterior interventricular artery, drains into coronary sinus) The major collecting vessels on the posterior surface of the heart Great cardiac vein Left atrium Coronary sinus Right atrium Left ventricle Posterior cardiac vein Small cardiac vein Right ventricle Posterior view Middle cardiac vein Figure18.4 4 Module 18.4 Review a. List the arteries and veins of the heart. b. Describe what happens to blood flow during elastic rebound. c. Identify the main vessel that drains blood from the myocardial capillaries. Module 18.5: Internal heart anatomy • Internal heart anatomy • Four chambers • • Two atria (left and right separated by interatrial septum) Two ventricles (left and right separated by interventricular septum) • Left atrium flows into left ventricle • Right atrium flows into right ventricle Module 18.5: Internal heart anatomy • Right atrium • • • • Receives blood from superior and inferior venae cavae and coronary sinus Fossa ovalis (remnant of fetal foramen ovale) Pectinate (pectin, comb) muscles (muscular ridges on anterior atrial and auricle walls) Left atrium • Receives blood from pulmonary veins Module 18.5: Internal heart anatomy • Right ventricle • Receives blood from right atrium through right atrioventricular (AV) valve • Also known as tricuspid (tri, three) • • Has three flaps or cusps attached to tendinous connective fibers Fibers connect to papillary muscles • • Innervated to contract through moderator band which keeps “slamming” of AV cusps Prevents backflow of blood to atrium during ventricular contraction Module 18.5: Internal heart anatomy • Left ventricle • Receives blood from left atrium through right atrioventricular valve • • • • Also known as bicuspid and mitral (mitre, bishop’s hat) valve Prevents backflow of blood to atrium during ventricular contraction Has paired flaps or cusps Trabeculae carneae (carneus, fleshy) • • Muscular ridges on ventricular walls Aortic valve • Allows blood to exit left ventricle and enter aorta The internal anatomy of the heart and the direction of blood flow between the chambers Ascending aorta Pulmonary trunk Superior vena cava Left Atrium Right Atrium Aortic arch Receives blood from the superior and inferior venae cavae and from the cardiac veins through the coronary sinus Receives blood from the pulmonary veins Left pulmonary veins Fossa ovalis Pectinate muscles on the inner surface of the auricle Opening of the coronary sinus Left Ventricle Right Ventricle Thick wall of left ventricle Right atrioventricular (AV) valve (tricuspid valve) Chordae tendineae Papillary muscle Pulmonary valve (pulmonary semilunar valve) Left atrioventricular (AV) valve (bicuspid valve) Inferior vena cava Trabeculae carneae Interventricular septum Moderator band Aortic valve Figure18.5 1 Module 18.5: Internal heart anatomy • Ventricular comparisons • Right ventricle has relatively thin wall • • • Ventricle only pushes blood to nearby pulmonary circuit When it contracts, it squeezes against left ventricle wall forcing blood out pulmonary trunk Left ventricle has extremely thick wall and is round in cross section • • Ventricle must develop 4–6× as much pressure as right to push blood around systemic circuit When it contracts 1. 2. Diameter of chamber decreases Distance between base and apex decreases A sectional view of the heart showing the thicknesses of the ventricle walls and the shapes of the ventricular chambers Posterior interventricular sulcus The left ventricle has an extremely thick muscular wall and is round in cross section. The relatively thin wall of the right ventricle resembles a pouch attached to the massive wall of the left ventricle Fat in anterior interventricular sulcus Figure18.5 2 The changes in ventricle shape during ventricular contraction Right ventricle Left ventricle Dilated (relaxed) Contraction of left ventricle decreases the diameter of the ventricular chamber and reduces the distance between the base and apex Contraction of right ventricle squeezes blood against the thick wall of the left ventricle. Contracted Figure18.5 3 Module 18.5 Review a. Damage to the semilunar valves on the right side of the heart would affect blood flow to which vessel? b. What prevents the AV valves from swinging into the atria? c. Why is the left ventricle more muscular than the right ventricle? Module 18.6: Heart valves • Semilunar (half-moon shaped) valves • Aortic and pulmonary semilunar valves • Allow blood to exit ventricles and enter aorta or pulmonary trunk • Do not require muscular braces because cusps are stable • All three symmetrical cusps support each other Module 18.6: Heart valves • Valve action during atrial contraction and ventricular relaxation • AV valves • Open • Blood pressure from contracting atria pushes cusps apart • Chordae tendineae are loose, offering no resistance • Semilunar valves (aortic and pulmonary) • Closed • Little pressure from ventricles • Blood pressure from aorta and pulmonary arteries keep closed The positions of the valves and associated structures when the ventricles are relaxed Pulmonary veins Left atrium Right ventricle Aortic valve (closed) Left AV (bicuspid) valve (open) Left ventricle (dilated) Right AV (tricuspid) valve (open) Aortic valve (closed) Superior view of cardiac valves Pulmonary valve (closed) Chordae tendineae (loose) Papillary muscles (relaxed) KEY Oxygenated blood Deoxygenated blood Figure18.6 1 Module 18.6: Heart valves • Valve action during atrial relaxation and ventricular contraction • AV valves • Closed • Blood pressure from contracting ventricles pushes cusps together • Papillary muscles tensing prevent cusps from swinging into atria (would allow backflow or regurgitation) • Semilunar valves (aortic and pulmonary) • Open • High blood pressure from ventricles overcome blood pressures from aorta and pulmonary arteries Animation: The Heart: Valves KEY Aortic sinus Oxygenated blood The positions of the valves and associated structures when the ventricles contract Aorta Left atrium Deoxygenated blood Aortic valve (open) Left AV (bicuspid) valve (closed) Left ventricle (contracted) Right AV (tricuspid) valve (closed) Chordae tendineae (tense) Papillary muscles (contracted) Ventricular contraction Aortic valve (open) Superior view of cardiac valves Pulmonary valve (open) Frontal section through left atrium and ventricle Figure18.6 2 Module 18.6: Heart valves • Cardiac skeleton • Flexible connective tissues in which all valves are encircled and supported • Also surrounds aorta and pulmonary trunk • Separates atrial and ventricular myocardium • Contains dense bands of tough elastic tissue A superior view of the heart showing the cardiac skeleton Cardiac skeleton Figure18.6 3 Module 18.6 Review a. Define cardiac regurgitation. b. Compare the structure of the tricuspid valve with that of the pulmonary valve. c. What do semilunar valves prevent? Section 2: The Cardiac Cycle • Cardiac cycle • Period from one heartbeat to the beginning of next • Alternating periods of contraction (systole) and relaxation (diastole) • Atria contract as a pair first • • Ventricles contract as a pair next • • As ventricles are relaxed and filling As atria are relaxed and filling Cardiac pacemaker system coordinates • Typical cardiac cycle lasts 800 msec A cardiac cycle: a heartbeat (contraction) followed by a brief period of relaxation Relaxation Contraction Figure18 Section2 1 The sequence of events during a single heartbeat Relaxation Atria contract Ventricles contract Figure18 Section2 2 Relaxation The two phases of the cardiac cycle for a given chamber in the heart: systole (contraction) and diastole (relaxation) Start 0 800 msec msec 100 msec Cardiac cycle 370 msec Figure18 Section2 3 Module 18.8: Cardiac cycle phases • Steps of cardiac cycle (for 75 bpm heart rate) 1. 2. When cycle begins, all four chambers are relaxed Atrial systole (100 msec) • 3. Contracting atria fill relaxed ventricles with blood Atrial diastole (270 msec) • 4. Concurrent with ventricular systole (2 phases) Ventricular systole – first phase • • Contracting ventricles push AV valves open but not enough pressure to open semilunar valves = Isovolumetric contraction Module 18.8: Cardiac cycle phases • Steps of cardiac cycle (continued) 5. Ventricular systole – second phase • 6. As ventricular pressure rises, semilunar valves open and blood leaves ventricle (= ventricular ejection) Ventricular diastole – early • • 7. Ventricles relax and blood pressure in them drops allowing closure of semilunar valves Isovolumetric relaxation occurs with AV valves still closed Ventricular diastole – late • • All chambers relaxed Ventricles fill passively to roughly 70% Animation: The Heart: Cardiac Cycle The phases of the cardiac cycle for a heart rate of 75 beats per minute Start Ventricular diastole lasts 530 msec (the 430 msec remaining in this cardiac cycle, plus the first 100 msec of the next). Throughout the rest of this cardiac cycle, filling occurs passively, and both the atria and the ventricles are relaxed. The next cardiac cycle begins with atrial systole and the completion of ventricular filling. When the cardiac cycle begins, all four chambers are relaxed, and the ventricles are partially filled with blood. 0 800 msec msec During atrial systole, the atria contract, completely filling the relaxed ventricles with blood. Atrial systole lasts 100 msec. 100 msec Atrial systole ends and atrial diastole begins and continues until the start of the next cardiac cycle. As atrial systole ends, ventricular systole begins. This period, which lasts 270 msec, can be divided into two phases. Ventricular systole— first phase: Ventricular contraction pushes the AV valves closed but does not create enough pressure to open the semilunar valves. This is known as the period of isovolumetric contraction. Cardiac cycle Ventricular diastole —late: All chambers are relaxed. The ventricles fill passively to roughly 70% of their final volume. 370 msec Blood flows into the relaxed atria but the AV valves remain closed. This is known as the period of isovolumetric relaxation. Ventricular systole— second phase: As ventricular pressure rises and exceeds pressure in the arteries, the semilunar valves open and blood is forced out of the ventricle. This is known as the period of ventricular ejection. Ventricular diastole— early: As the ventricles relax, the pressure in them drops; blood flows back against the cusps of the semilunar valves and forces them closed. Figure18.8 1 The pressure changes within the aorta, left atrium, and left ventricle during the cardiac cycle ATRIAL ATRIAL DIASTOLE SYSTOLE VENTRICULAR DIASTOLE ATRIAL SYSTOLE ATRIAL DIASTOLE VENTRICULAR SYSTOLE VENTRICULAR DIASTOLE Aortic valve closes. 120 Aortic valve opens. Pressure (mm Hg) 90 Dicrotic notch KEY Atrial contraction begins. Atria eject blood into ventricles. 60 Atrial systole ends; AV valves close. Left ventricle Isovolumetric contraction. Ventricular ejection occurs. Semilunar valves close. 30 Isovolumetric relaxation occurs. Left AV valve closes. Left atrium AV valves open; passive ventricular filling occurs. Left AV valve opens. 0 0 100 200 300 400 500 600 700 800 Time (msec) The correspondence of the heart sounds with events during the cardiac cycle S1 S4 S2 S3 S4 Heart sounds “Lubb” “Dubb” Figure18.8 2 Module 18.8: Cardiac cycle phases • Heart sounds • • • • • • • • S1 (known as “lubb”) Start of ventricular contraction and closure of AV valves S2 (known as “dupp”) Closure of semilunar valves S3 and S4 Very faint and rarely heard in adults S3 (blood flowing into ventricles) S4 (atrial contraction) Module 18.8 Review a. Provide the alternate terms for heart contraction and heart relaxation. b. List the phases of the cardiac cycle. c. Is the heart always pumping blood when pressure in the left ventricle is rising? Explain. Module 18.9: Cardiac output and conduction system • Conduction system • • Network of specialized cardiac muscle cells Responsible for initiating and distributing stimulus to contract • • Can do so on their own (= automaticity) Components 1. Sinoatrial (SA) node • • 2. Embedded in posterior wall of right atrium Impulse generated by this pacemaker is distributed through other components Internodal pathways • Distribute signal to atria on way to ventricles Module 18.9: Cardiac output and conduction system • Conduction system (continued) 3. Atrioventricular (AV) node • • • • Located at junction of atria and ventricles Also contains pacemaker cells If SA node damaged, can maintain heart rate at 40–60 bpm Can conduct impulses at maximum rate of 230/min • 4. = Maximum heart rate AV bundle and branches • • • Located in interventricular septum Normally only electrical connection between atria and ventricles Branches relay signal to ventricles toward heart apex Module 18.9: Cardiac output and conduction system • Conduction system (continued) 5. Purkinje fibers • Large-diameter conducting cells • • As fast as small myelinated axons Final part of conduction system that triggers ventricular systole Animation: The Heart: Conduction System The components of the conducting system and their specific functions Each heartbeat begins with an action potential generated at the sinoatrial (sī-nō-Ā-trē-al) node, or simply the SA node. The SA node is embedded in the posterior wall of the right atrium, near the entrance of the superior vena cava. The electrical impulse generated by this cardiac pacemaker is then distributed by other cells of the conducting system. Purkinje fibers are large-diameter conducting cells that propagate action potentials very rapidly—as fast as small myelinated axons. Purkinje cells are the final link in the distribution network, and they are responsible for the depolarization of the ventricular myocardial cells that triggers ventricular systole. In the atria, conducting cells are found in internodal pathways, which distribute the contractile stimulus to atrial muscle cells as the impulse travels toward the ventricles. The atrioventricular (AV) node is located at the junction between the atria and ventricles. The AV node also contains pacemaker cells, but they do not ordinarily affect the heart rate. However, if the SA node or internodal pathways are damaged, the heart will continue to beat because in the absence of commands from the SA node, the AV node will generate impulses at a rate of 40–60 beats per minute. The AV node delivers the stimulus to the AV bundle, located within the interventricular septum. The AV bundle is normally the only electrical connection between the atria and the ventricles. Moderator band The AV bundle leads to the right and left bundle branches. The left bundle branch, which supplies the massive left ventricle, is much larger than the right bundle branch. Both branches extend toward the apex of the heart, turn, and fan out deep to the endocardial surface. Figure18.9 3 An action potential is generated at the SA node, and atrial activation begins. The distribution of the contractile stimulus, and how the conducting system coordinates the contractions of the cardiac cycle SA node Time = 0 The stimulus spreads across the atrial surfaces by cell-to-cell contact within the internodal pathways and soon reaches the AV node. AV node Elapsed time = 50 msec A 100-msec delay occurs at the AV node. During this delay, atrial contraction begins. AV bundle Bundle branches Elapsed time = 150 msec As atrial contraction continues, the impulse travels along the interventricular septum within the AV bundle and the bundle branches to the Purkinje fibers and, via the moderator band, to the papillary muscles of the right ventricle. Moderator band Elapsed time = 175 msec The impulse is distributed by Purkinje fibers and relayed throughout the ventricular myocardium. Atrial contraction is completed, and ventricular contraction begins. Purkinje fibers Elapsed time = 225 msec Figure18.9 4 Module 18.9 Review a. Define automaticity. b. If the cells of the SA node failed to function, how would the heart rate be affected? c. Why is it important for impulses from the atria to be delayed at the AV node before they pass into the ventricles? Module 18.11: Autonomic control of heart function • Autonomic control of heart function • Pacemaker cells in the SA and AV nodes cannot maintain a stable resting potential • Always gradual depolarization leading to threshold (= prepotential or pacemaker potential) • Fastest rate at SA node (80–100 bpm) • Brings other conduction system components to threshold Heart rate under three conditions: at rest, under parasympathetic stimulation, and under sympathetic stimulation A prepotential or pacemaker potential in a heart at rest +20 Membrane potential (mV) Normal (resting) Prepotential (spontaneous depolarization) 0 –30 Threshold –60 Heart rate: 75 bpm 0.8 1.6 Time (sec) 2.4 Figure18.11 1 Module 18.11: Autonomic control of heart function • Autonomic changes to intrinsic heart rate • Factors that change rate of depolarization and repolarization will change time to threshold • Leads to change in heart rate • Bradycardia (heart rate slower than normal, <60 bpm) • Tachycardia (heart rate faster than normal, >100 bpm) • Parasympathetic stimulation • Binding of ACh from parasympathetic neurons opens K+ channels, slows heart rate • Slows rate of depolarization • Extends duration in repolarization Module 18.11: Autonomic control of heart function • Autonomic changes to intrinsic heart rate (continued) • Sympathetic stimulation • Binding of noepinephrine to beta-1 receptors leads to opening of ion channels, and increases heart rate • Increases rate of depolarization • Shortens duration in repolarization Heart rate under three conditions: at rest, under parasympathetic stimulation, and under sympathetic stimulation A prepotential or pacemaker potential in a heart at rest Increased heart rate resulting when ACh released by parasympathetic neurons opens chemically gated K+ channels, thereby slowing the rate of spontaneous depolarization Parasympathetic stimulation +20 Membrane potential (mV) 0 –30 Threshold Hyperpolarization –60 Slower depolarization Heart rate: 40 bpm 0.8 1.6 2.4 Time (sec) Figure18.11 2 CLINICAL MODULE 18.14: Electrocardiograms (ECG) • Electrocardiograms record electrical activities of heart from body surface through time • Can be used to assess performance of: • • • • Nodes Conduction system Contractile components Appearance varies with placement and number of electrodes or leads An electrocardiogram: a standard placement of leads and the tracing that results One of the standard configurations for the placement of leads for an ECG 800 msec The features of a typical electrocardiogram P wave QRS complex T wave +1 R +0.5 T P 0 Millivolts Q S –0.5 P–R interval Q–T interval Figure18.14 1 CLINICAL MODULE 18.14: Electrocardiograms (ECG) • Typical ECG features • P wave (atrial depolarization) • • QRS complex (atrial repolarization and ventricular depolarization) • • • Atria begin contracting ~25 msec after P wave start Larger wave due to larger ventricles added to atrial activity Ventricles begin contracting shortly after R wave peak T wave (ventricular repolarization) CLINICAL MODULE 18.14: Electrocardiograms (ECG) • Typical ECG features (continued) • P-R interval (start of atrial depolarization to start of ventricular depolarization) • • >200 msec may indicate damage to conducting pathways or AV node Q-T interval (time for ventricles to undergo a single cycle) • Starts at end of P-R interval to end of T wave Module 18.16: Blood pressure and flow • Blood flow (F) is directly proportional to blood pressure • • Increased pressure = increased flow The pressure gradient (difference from one end of vessel to other) is more important • Large gradient from aorta to capillaries • Smaller, more numerous vessels produce more resistance, reducing pressure and flow • • At aorta: 2.5 cm diameter and 100 mm Hg pressure At capillaries: 8 µm diameter and 25 mm Hg pressure Module 18.16: Blood pressure and flow • Arterial pressure is variable • • Rising during ventricular systole (systolic pressure) Declining during ventricular diastole (diastolic pressure) • Commonly written with a “/” between pressures • • Pulse pressure (difference between systolic and diastolic) • • Example: 120/90 Example: 120 – 90 = 30 mm Hg Mean arterial pressure (MAP) • • Adding 1/3 of pulse pressure to diastolic pressure Example: 90 + (120 – 90)/3 = 100 mm Hg The calculation of mean arterial pressure Pulse pressure, the difference between systolic and diastolic pressures Systolic 120 Mean arterial pressure (MAP), the sum of the diastolic pressure and one-third of the pulse pressure 100 80 Here, MAP is Diastolic 60 mm Hg 90 + (120 – 90 )/3 or 90 + 10 = 100 mm Hg 40 20 0 Aorta Elastic Muscular Arterioles Capillaries Venules Medium- Large Venae sized veins veins cavae arteries arteries Figure18.16 4 Module 18.16: Blood pressure and flow • Capillary exchange • Involves: • Filtration • • • • • Capillary hydrostatic pressure (CHP) provides driving force Water and small solutes leave capillaries Larger molecules (like plasma proteins) remain in blood Diffusion Osmosis The effect of capillary hydrostatic pressure on water and small solutes Capillary hydrostatic pressure (CHP) Amino acid Blood protein Glucose Ions Interstitial fluid Small solutes Hydrogen bond Water molecule Endothelial cell 1 Endothelial cell 2 Figure18.16 5 Module 18.16 Review a. Define blood flow, and describe its relationship to blood pressure and peripheral resistance. b. In a healthy individual, where is blood pressure greater: in the aorta or in the inferior vena cava? Explain. c. For an individual with a blood pressure of 125/70, calculate the mean arterial pressure (MAP).